


Abstract
We present the case of a 76-y-old man with mixed (type III) paraesophageal hernia confirmed by endoscopy and CT of the chest who underwent a radionuclide gastric-emptying study that showed accumulation of the radiotracer in the herniated stomach and esophagus in the thorax and accelerated gastric emptying. A scintigraphic gastric-emptying study may be an option for noninvasively demonstrating gastroesophageal accumulation of tracer in patients with hiatal hernia.
- gastroenterology
- radiopharmaceuticals
- gastric-emptying study
- gastroesophageal reflux
- hiatal hernia
- scintigraphic
In a 76-y-old man with repaired type III hiatal hernia documented by esophagogastroduodenoscopy and radiography, including 2 CT examinations of the chest, scintigraphy showed rapid gastric emptying and evidence of tracer regurgitation in the herniated stomach and esophagus in the left mediastinum. The abnormal tracer accumulation could be quantified by a noninvasive radionuclide gastric-emptying study, as described in this case report.
CASE REPORT
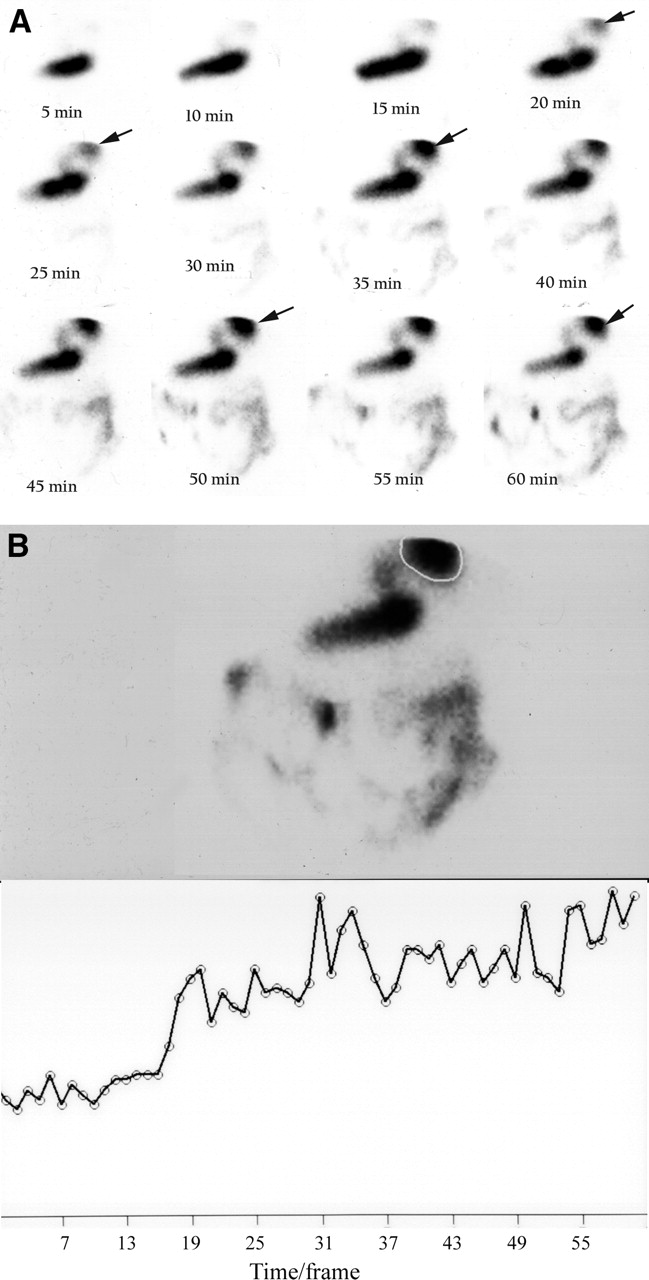
A 76-y-old man with a paraesophageal hernia and a 5-y history of deglutition disorder with gastroesophageal reflux was referred for a gastric-emptying study, which was performed using 99mTc-macroaggregated albumin (MAA)–labeled beef stew (3 pieces of beef stew [Hormel Food Corp.] injected with 37 MBq of 99mTc-MAA and microwaved for 30 s). The patient experienced some difficulty in swallowing the test meal. He was upright while swallowing the meal and then lay supine for thoracoabdominal imaging. Radiotracer appeared in the stomach initially; however, an area of gradually increasing activity was noted in the intrathoracic region above the normal position of the stomach, on the left side of the thorax (Fig. 1A). Activity in the region steadily increased during the 60-min imaging study (Fig. 1B); the activity was calculated at 9% of the ingested test dose. Substantial radiotracer from the stomach was also transported to the small bowel (Fig. 1B), and gastric-emptying half-times were calculated at 28 min (n = 45–80 min).

(A) 99mTc-MAA–labeled beef for gastric-emptying study shows gradual accumulation of radiotracer in right upper corner (arrows); area of faint activity between reflux esophageal activity (arrows) and body of stomach is hiatus-herniated stomach and esophagus. Radiotracer in stomach is also rapidly transported to small bowel. (B) Time–activity curve for herniated stomach and esophagus. Top: image taken at end of 60-min course. Region of interest is plotted in herniated stomach and esophagus. Bottom: Time–activity curve shows gradually increased counts during 60-min imaging study. Region accumulated at least 9% of ingested radiotracer dose. Part of esophageal reflux area was not included in view of region of interest.
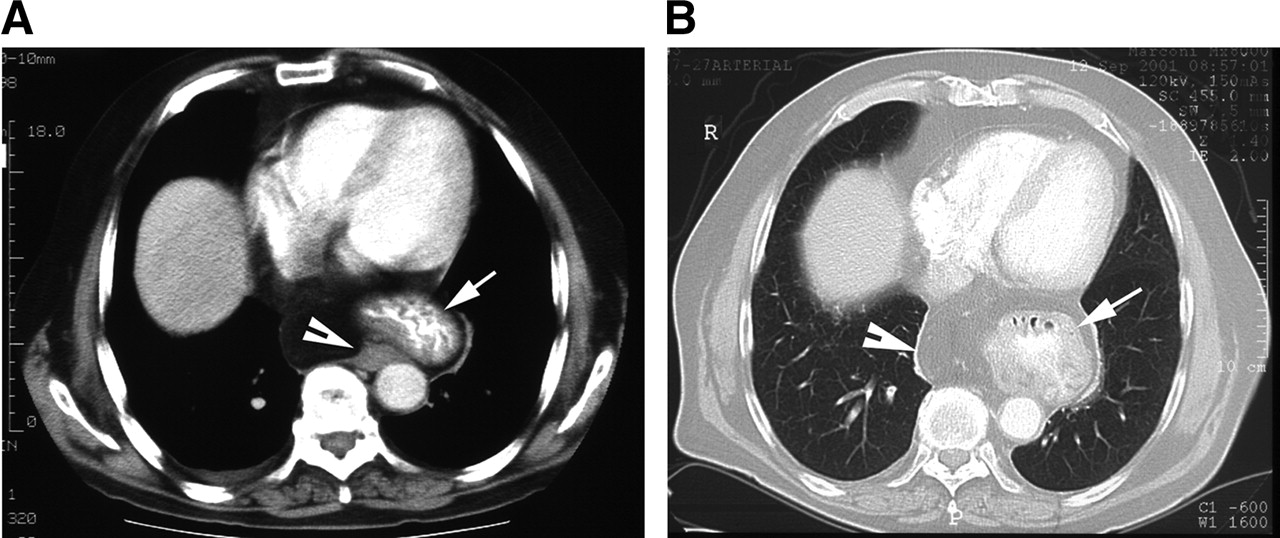
CT of the chest had shown a predominantly left-sided large hiatal hernia in the posterior mediastinum 3 y previously (Fig. 2A). Concurrent CT of the chest and abdomen during the present investigation showed a large hiatal hernia and dilated esophagus secondary to a stricture of the distal esophagus (Fig. 2B). He had undergone laparoscopic cholecystectomy 8 y previously and esophagogastroduodenoscopy 3 y previously, which revealed a large hiatal hernia and a benign intrinsic stenosis in the lower third of the esophagus 38 cm from the teeth. An upper-gastrointestinal series with barium performed 1 y previously revealed a moderately large sliding hiatal hernia with associated gastroesophageal reflux and esophageal dysmotility. A second esophagogastroduodenoscopy, which was performed about a month after the first, again showed a hiatal hernia; friable and erythematous mucosa at the gastroesophageal junction; erosive gastritis; multiple nonbleeding erythematous linear ulcers in the antrum, body of the stomach, cardia, and fundus; a moderately deformed pylorus; edematous and erythematous mucosa in the pylorus; and duodenitis. About 3 mo later, a third esophagogastroduodenoscopy was performed and found a big, baggy, tortuous esophagus; a type III paraesophageal hernia with the hiatus 34 cm from the gums and the diaphragm 41 cm from the mouth; and esophagitis, antritis, and duodenitis. About 2 mo later, a fourth esophagogastroduodenoscopy was performed and revealed a large, baggy, tortuous esophagus; a large, axial hiatal hernia; the esophageal hiatus 45 cm from the mouth and the gastroesophageal junction 34 cm from the gums; and prolapsed gastropathy.

(A) Contrast CT of thorax and abdomen shows predominantly left-sided large hiatal hernia containing contrast medium in stomach (arrow), in posterior mediastinum, and in herniated omentum (arrowhead). (B) CT of chest with lung window shows hiatal hernia with contrast medium in stomach in left posterior mediastinum (arrow); herniated omentum is seen at midline (arrowhead).
Two months after the gastric-emptying scintigraphic study, the patient underwent mixed (type III) hiatal hernia repair and gastrostomy tube placement. The postoperative course was uneventful, and the patient was discharged on the 22nd postoperative day.
DISCUSSION
Gradual thoracic accumulation of radiotracer from solid food (99mTc-MAA–labeled beef stew) occurred in the region of the herniated stomach (gastric fundus) and dilated esophagus in the left mediastinum as shown in Figures 1 and 2. When the patient’s position changed from upright to supine after he had swallowed the test meal, his stomach and esophagus were sliding toward the mediastinum. The accumulation of radiotracer in the herniated stomach and esophagus might explain the patient’s progressive deglutition. This patient underwent 4 esophagogastroduodenoscopic examinations, which revealed acute and chronic esophageal and gastric inflammation in a type III esophageal hiatal hernia—a combined sliding and paraesophageal hiatal hernia.
Type III hiatal hernia is defined as displacement of the esophagogastric junction above the diaphragm (sliding component) and the fundus and rolling of the greater curvature of the stomach through the hiatus to form a large, bulbous, supradiaphragmatic gastric loculus (paraesophageal component) (1,2). Paraesophageal (type II) hernias are rare compared with the more commonly diagnosed sliding hiatal (type I) hernia. Type II hernia accounts for about 5%, and type I hernias accounts for approximately 95%. As with our patient, most paraesophageal hernias are in fact type III or of mixed type (1,2).
Paraesophageal hiatal hernias, whether in isolation or in combination with sliding hernias (type III), are associated with a significant risk of life-threatening complications such as bleeding, obstruction, or incarceration/strangulation (1,2). Therefore, surgical repair or laparoscopic repair for type II or III is indicated (1,2). Laparoscopic repair of type III hiatal hernia is associated with a high prevalence (42%) of recurrent hernia (2); our patient underwent surgical repair.
The hiatal hernia radiographic examinations, including upper-gastrointestinal series and radiography and CT of the chest, exhibited protrusion of a part of the stomach into the mediastinum. The characteristic location of hiatal hernia creates a mass in the posteroinferior mediastinum, which is usually on the left side; but larger hernias can cross the midline from the left to the right side (3). By providing a cross-sectional image of the esophageal hiatus and the adjacent region, CT plays an important role in the early diagnosis of hernias and their actual size and content by depicting stomach and omental fat (3). Herniated portions of the type III hiatal hernia seen on our patient’s chest CT scan included the stomach and omentum, as shown in Figure 2.
Hiatal hernias play a role in the pathogenesis of reflux disease (4,5). Using pH monitoring, Ott et al. found that 94% of patients with reflux esophagitis had a hiatal hernia in a population with a 51% prevalence of disease (6). The positive predictive value of hiatal hernia in patients with reflux esophagitis was 62%, and the negative predictive value of the absence of hernia in excluding esophagitis was 68% (4). Patients with larger hiatal hernias (>2 cm) were more likely to have abnormal findings using pH monitoring; smaller hiatal hernias were poorer predictors of the presence of abnormal gastroesophageal reflux (4). Our patient’s gastroesophageal reflux was detected directly on a radionuclide gastric-emptying study, and his hiatal hernia could certainly be classified as “larger” because it was more than 2 cm.
The use of radionuclide gastric-emptying scintigraphy to demonstrate hiatal hernia has been reported (7). In that study, most radiotracer lodged and hanged intrathoracically and little radiotracer was noted in the stomach subdiaphragmatically; therefore, gastroesophageal reflux was not detected. Our patient’s scintigraphic gastric images initially demonstrated the stomach, though he had had difficulty swallowing the test meal. Apparently, the test meal arrived smoothly in his stomach, and the gastric activity was then diverted upward and downward. The upward diversion was radiotracer regurgitating to the supradiaphragmatic esophagus; 9% of the ingested test dose appeared to be underestimated because the detector of the γ-camera did not cover the entire region of reflux. The downward diversion represented the normal pathway for emptying to the small bowel. Also, this patient’s gastric emptying was accelerated.
Delayed gastric emptying in gastroesophageal reflux in patients with hiatal hernia has previously been documented (8). In contrast to previous reports, our patient’s gastric emptying was rapid; a possible explanation was his severe, acute and chronic esophageal and gastric inflammation, as characterized by a friable and erythematous mucosa at the gastroesophageal junction, by gastritis, and by antritis—consequences of gastroesophageal reflux.
The prevalence of hiatal hernia increases with age (9). Paraesophageal hiatal hernia rarely presents before middle age (11) and has therefore been hypothesized to be an acquired abnormality (12). As with our patient, the average age of patients at diagnosis of paraesophageal hernia is the seventh decade (10). However, the size of our patient’s hiatal hernia did not change during a 3-y interval.
Acknowledgments
We thank Vickie Kiefer for technical assistance with the computer process and Mark Ingram for diligently and extensively researching the references.
Footnotes
For correspondence or reprints contact: Wei-Jen Shih, MD, 1101 Veterans Dr., Lexington, KY 40502.
E-mail: wei-jen.shih@med.va.gov





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.