


Abstract
Neuroreceptor imaging is a promising area of brain imaging used to investigate various neurodegenerative and neuropsychiatric disorders. In the research setting, radiopharmaceuticals targeted to specific areas of the brain are used along with SPECT to assess and analyze functional mechanisms within brain structures. Utilization of the data that are collected from these studies may aid in the development of drug therapies that can be used to relieve symptoms or delay progression of certain disease states. After reading this article, the nuclear medicine technologist should be able to identify and describe the role of structures in the brain, identify various radiopharmaceuticals used and the disease states they demonstrate, and become familiar with the drugs used in treatment of these disorders.
The field of neuroscience has continued to evolve since the first known usage of the word “neuro” in ancient Egypt (1). Ironically, the ancient Egyptians had a limited appreciation of the importance of the brain, opting not to preserve this organ along with other viscera during the mummification process. However, over time, fascination with the complexities of the brain and speculation as to its functions have encouraged the development of many theories and techniques used to observe and analyze brain structures. Today, an increased understanding of the molecular mechanisms associated with brain function has driven interest in neuroreceptor imaging.
STRUCTURES OF BRAIN
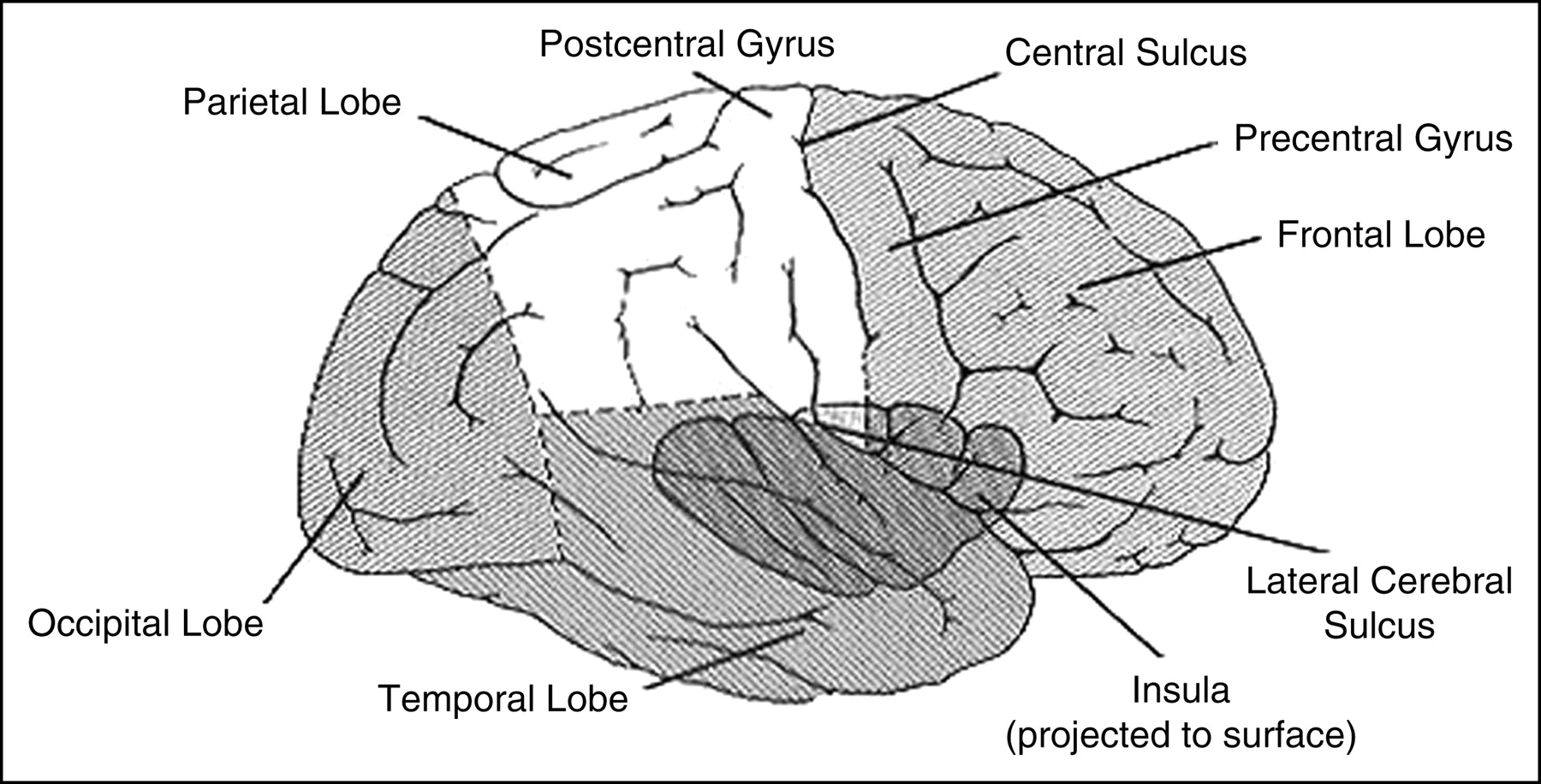
In the 17th Century, the English anatomist Thomas Willis (known for the circle of Willis, the vascular structure in the brain that bears his name) first divided the brain into cortical and subcortical structures (2). Cortical structures include the lobar regions of frontal, parietal, temporal, and occipital cortices and have been implicated in higher functioning, including the initiation of movement, memory, reason, speech, and so forth (Fig. 1).
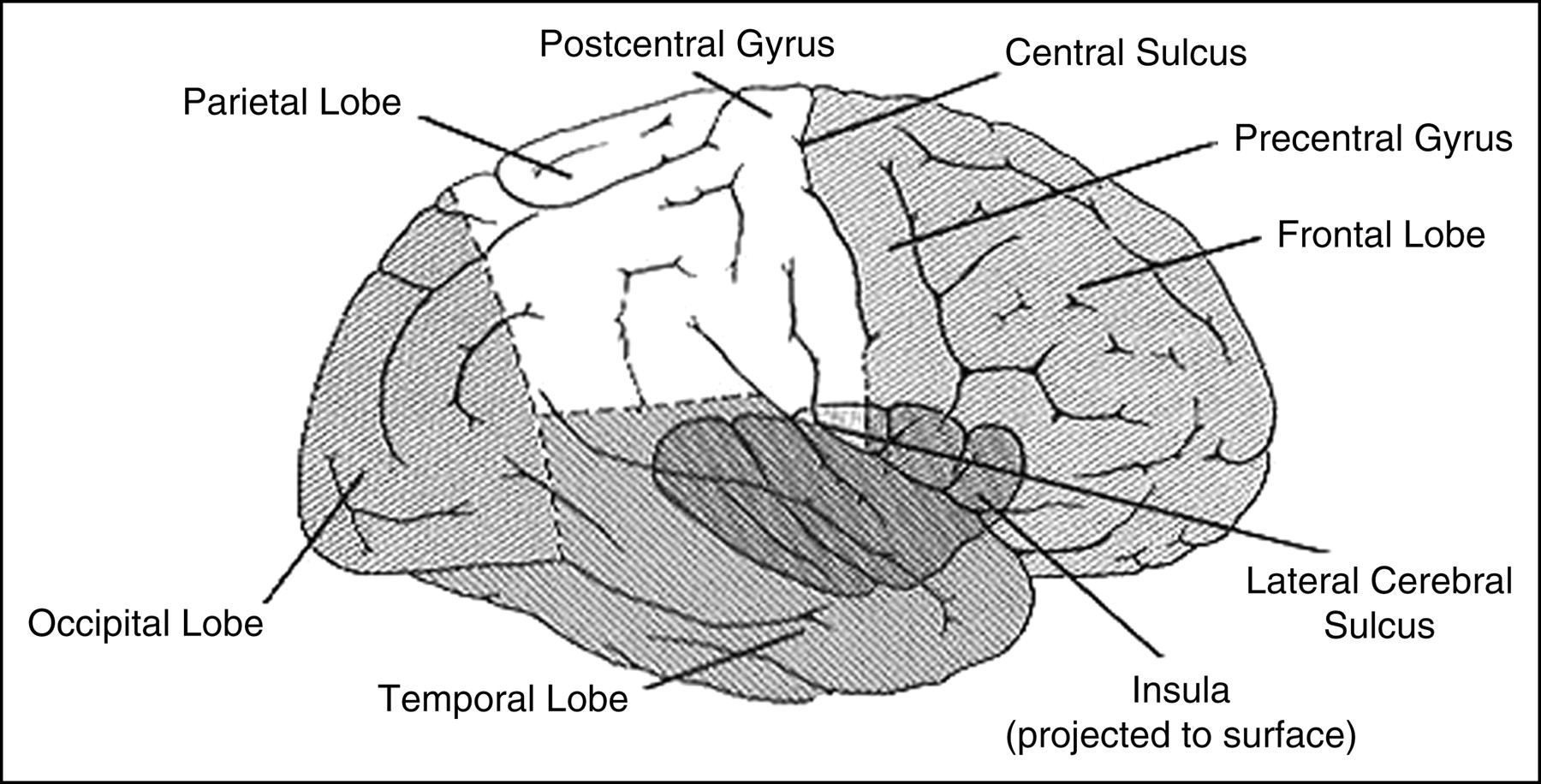
Lobes and fissures of cerebrum. (Reprinted with permission from (3).)
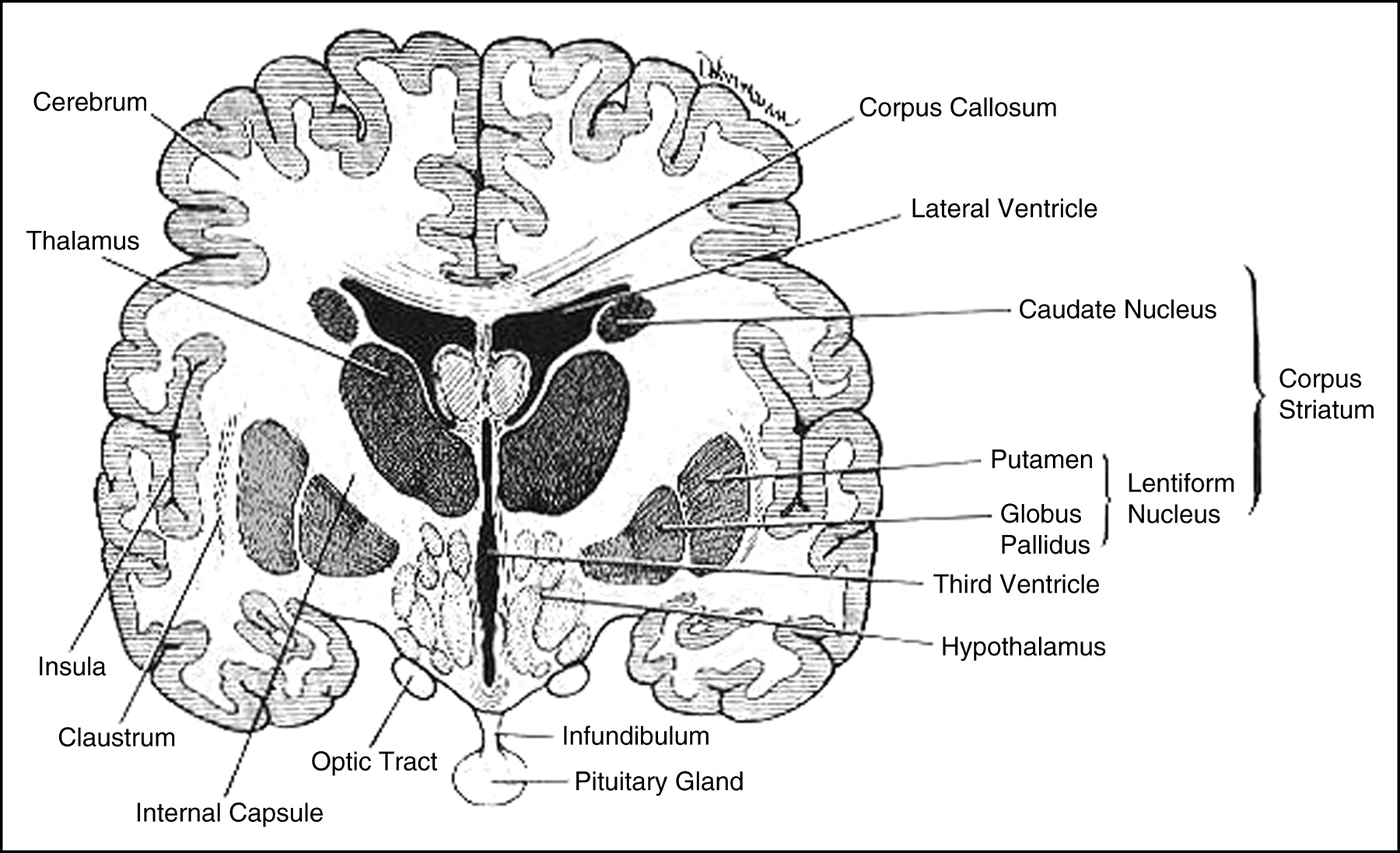
Subcortical regions are generally thought to subserve more administrative functions; serving as the seat of regulation of autonomic function and affect, as well as serving important relaying and processing functions between the central nervous system and peripheral organs of the body (3). One important subcortical region from the perspective of disease is the basal ganglia, which lies within the core of the forebrain. The basal ganglia consist of 5 interconnected nuclei: the caudate and putamen (collectively called the striatum), globus pallidus, substantia nigra, and the subthalamic nuclei located below the area of the thalamus (4) (Fig. 2).
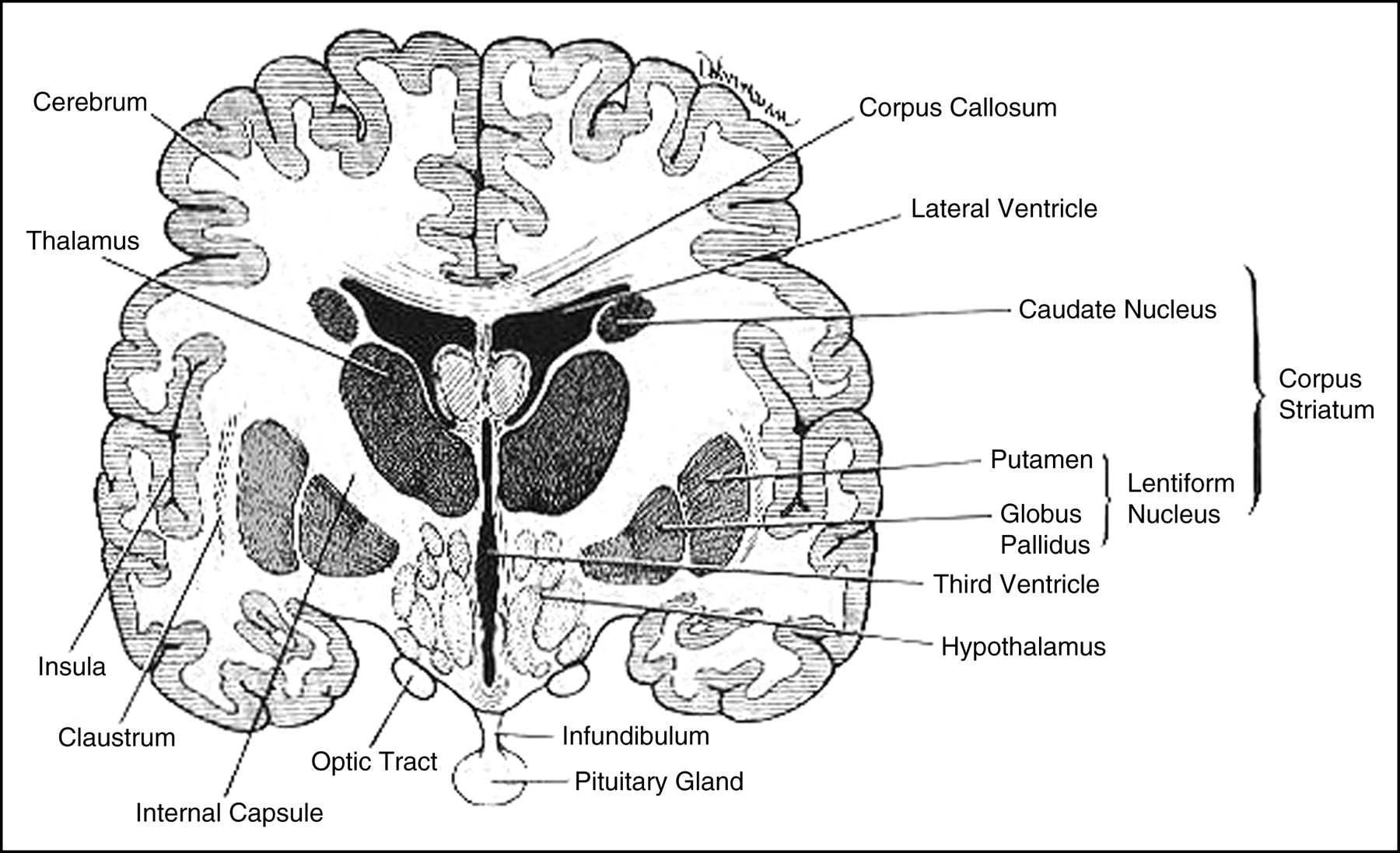
Diagram of frontal section of brain shows basal ganglia and associated structures. (Reprinted with permission from (3).)
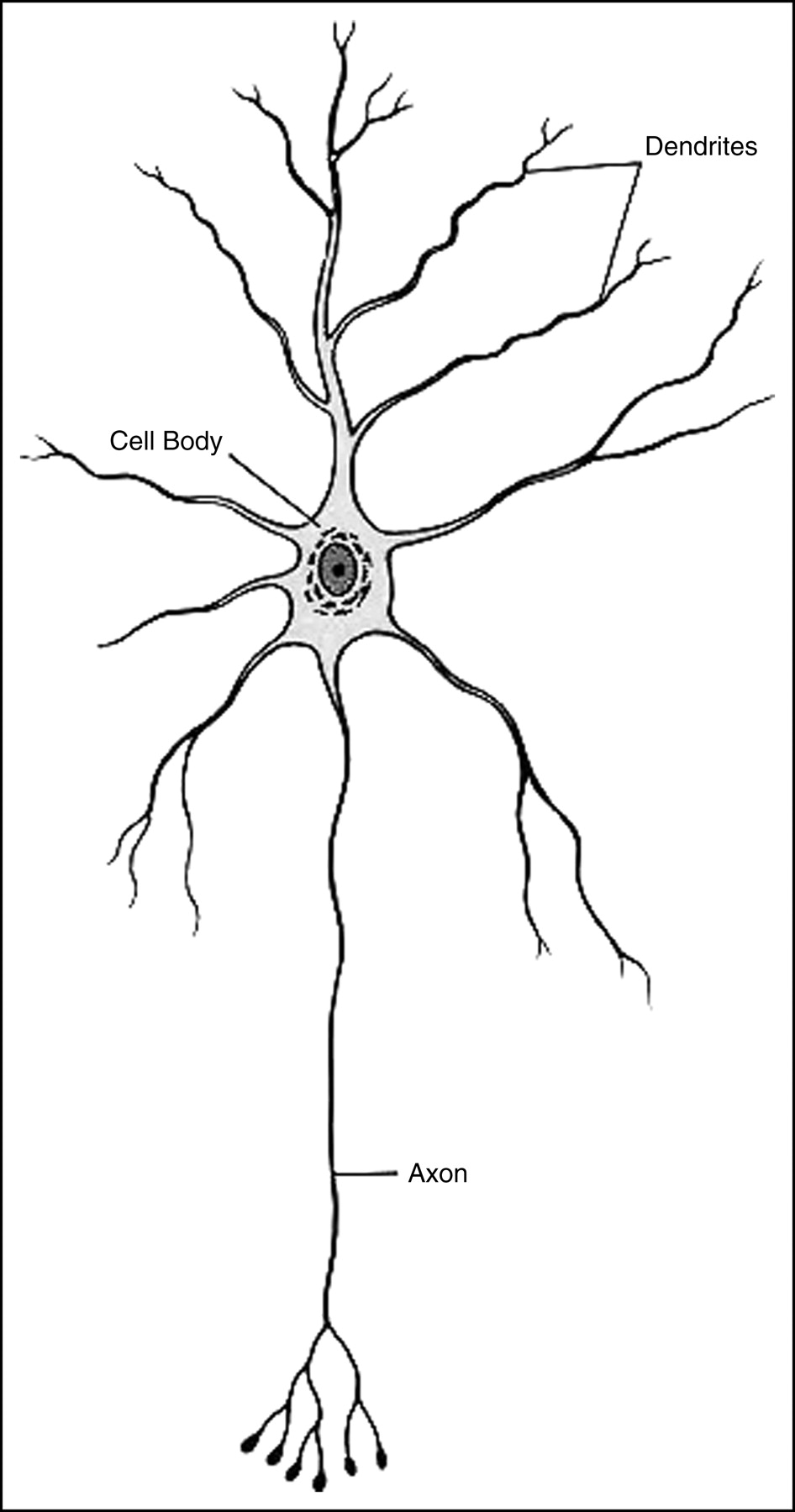
Considering the brain on a more microscopic level, these structures are made up of billions of cells called neurons and supporting cells called glia. The neurons consist of a cell body, or soma, with its associated nucleus and dendrites, an axon, and an axon terminal (Fig. 3). These neurons communicate with each other to ensure proper brain function via transfer of electrical impulses called action potentials.
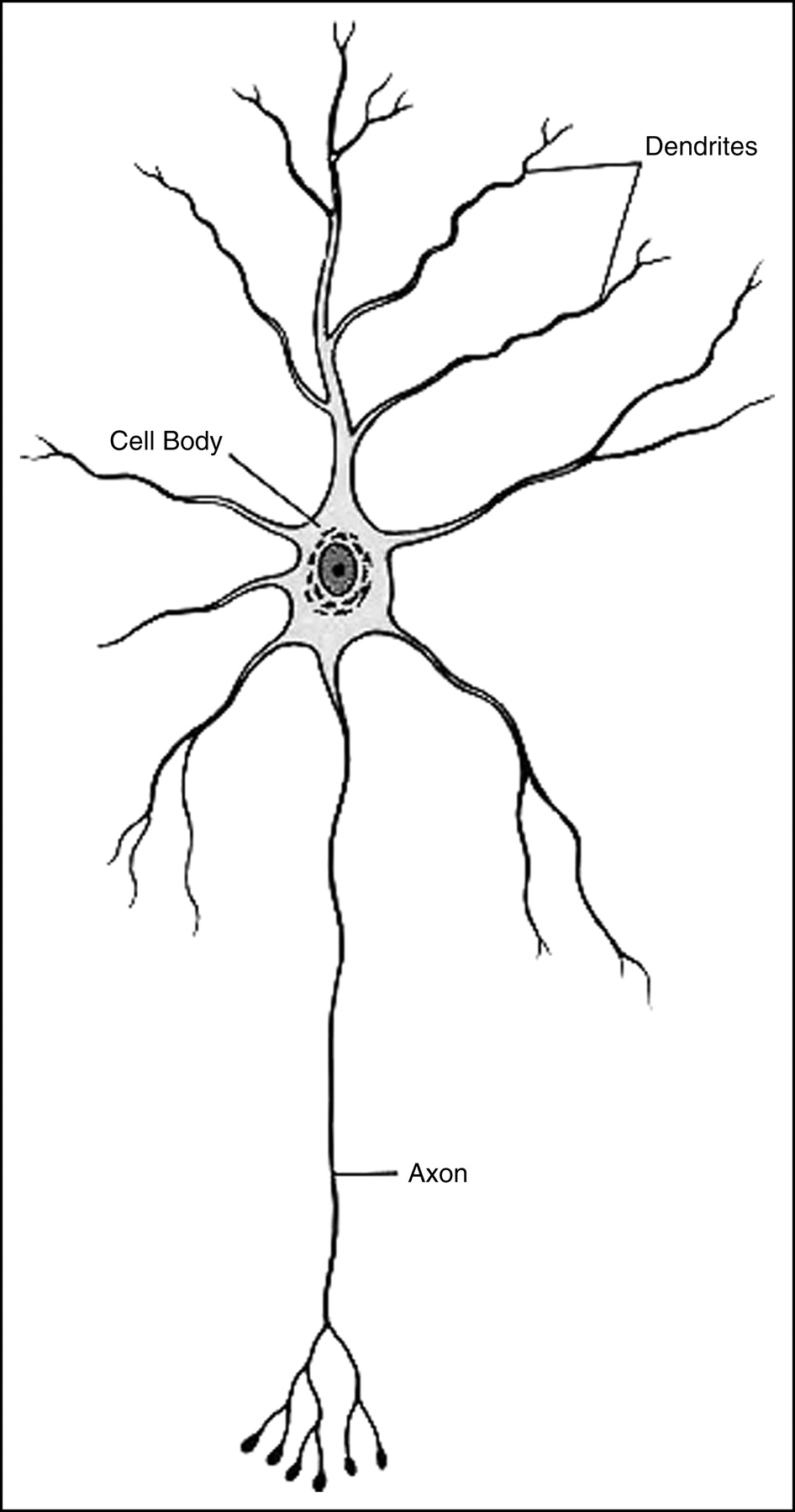
Typical neuron consisting of central cell body, axon, and dendrites. (Reprinted with permission from (3).)
Each neuron exists at a resting state or voltage. This voltage can be changed by the introduction of another action potential or voltage from a neighboring neuron at the dendrites of the cell body that is the receiving end of the neuron. If the incoming potential is strong enough to raise the voltage of the receptor neuron from its resting state and above its threshold for conduction, the voltage will travel down the axon to the axon terminal where a series of events will occur in order for the message to be transferred (5). This transfer of information between neurons occurs at a junction or gap that exists between neurons called the synapse.
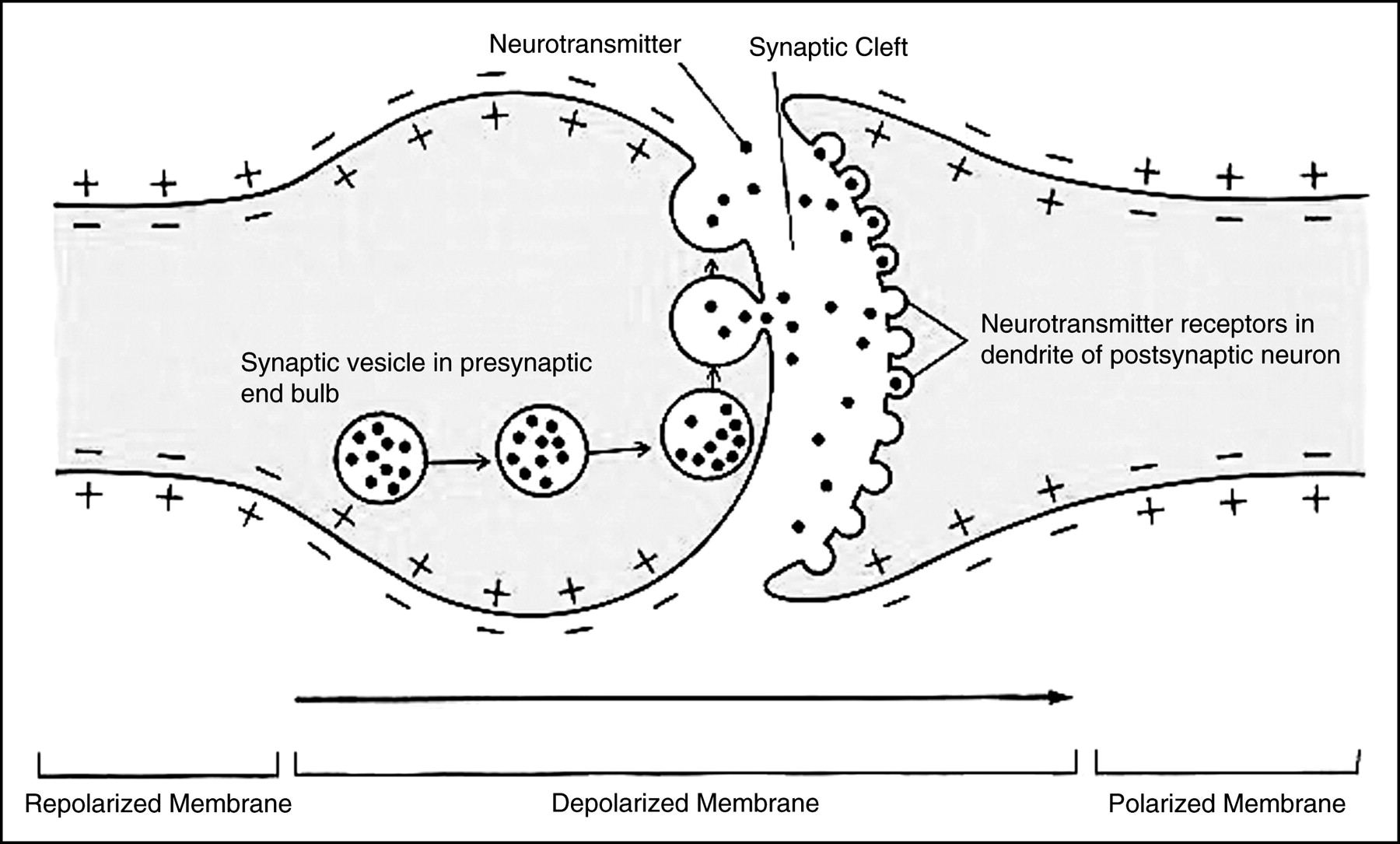
At the synapse, there is no direct contact between the presynaptic transmitting neuron and the postsynaptic receptor neuron at their junction. Therefore, there must be some way for the traveling impulse to reach the receiving neuron. The ability of nerve impulses to cross the synaptic cleft, or simply the synapse, to communicate with neighboring neurons is made possible by a process called neurotransmission (Fig. 4).
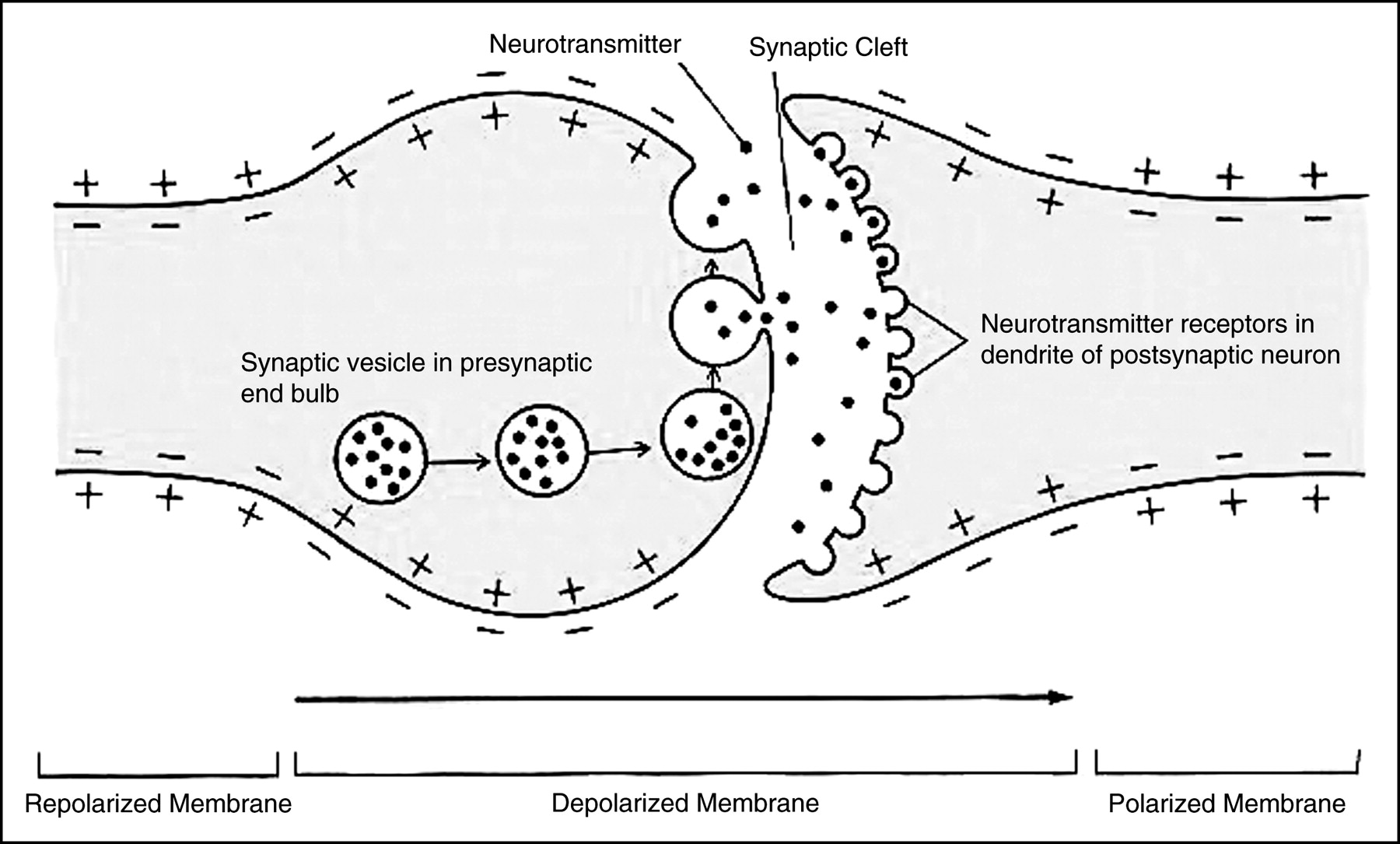
Impulse conduction at synapses. Shown is impulse conduction from presynaptic end bulb across synapse to postsynaptic dendrite in which synaptic vesicles fuse with presynaptic membrane and discharge neurotransmitter into synaptic cleft. (Reprinted with permission from (3).)
CHEMICAL MESSENGERS OF BRAIN
How does neurotransmission occur? In the presynaptic neuron, there are substances that are stored in small structures called storage vesicles. These substances are chemical messengers called neurotransmitters, which are released from their vesicles on arrival of an action potential. With energy drawn from mitochondria, they are released into the synapse and diffuse across the gap, where they will bind to receptors on the postsynaptic membrane in a lock-and-key fashion (6,7). Only certain configurations of neurotransmitters will fit onto specific receptor sites. Once the connection is made, changes in the permeability of the postsynaptic membrane allow the neurotransmitter to activate the neuron. Activation of the receptor neuron will result in either an excitatory or inhibitory response depending on the nature of the attached neurotransmitter. An excitatory response will excite the neuron to make actions happen—hence, continuing the action potential—whereas an inhibitory response will reduce the activity to keep it under control—hence, halting the action potential (6). After transmission is complete, any excess neurotransmitter still within the synapse is broken down by enzymes or reabsorbed back into the presynaptic neuron by transporters on its membrane for restorage into the vesicles for later use. The basis of neuroreceptor imaging is the ability to capture this functional chemistry occurring within the synapse.
It is important to keep in mind that the speed is on the order of milliseconds for an action potential to induce synaptic release of a neurotransmitter and for a postsynaptic response to occur (8). In addition, any particular postsynaptic neuron may receive input from many other neurons and, hence, serves to integrate the effects of multiple neurons impacting it within the circuit. There are many types of neurotransmitters and, hence, many types of receptors, each specific to a particular neurochemical. Examples of some common neurotransmitters are acetylcholine (Ach), γ-aminobutyric acid (GABA), dopamine (DA), norepinephrine, and serotonin.
NEURORECEPTOR IMAGING
With this basic machinery in mind, it is possible to develop highly selective targets that may be imaged with PET or SPECT. The radioactive tracer that is injected will bind to sites in the brain reflecting the distribution of the related neurochemistry. These tracers, called radioligands, are formulated to be chemically similar to biologically active compounds that target specific areas of interest.
Focusing on SPECT, many successful radioligands have been labeled with a radioactive atom of 123I. This radionuclide is preferred because of its relatively short half-life (13.2 h) and low γ-energy (159 keV) for imaging. By using techniques such as SPECT with radioligands, the ability to noninvasively assess and measure the functions of the brain as well as examine a diversity of disorders that affect normal brain function are possible.
As an example of how these radioligands can be used, 4 123I-radiolabeled ligands are discussed that are specific for either the receptors or the transporters at the synapse of brain neurons that can be used for neuroreceptor imaging: 123I-iodobenzamide (123I-IBZM), 123I-iomazenil (123I-IOM), 123I-5-I-A-85380 (123I-5-IA), and 123I-2β-carbomethoxy-3β-(4-iodophenyl)tropane (123I-β-CIT). The basic acquisition and technical parameters for each of these studies have similar requirements, which include an acquisition with sufficient time for ample counts per step, 360° rotation, and a triple-head camera with fanbeam collimation. Studying the uptake patterns of these compounds will aid in diagnosing and monitoring illnesses as well as development of new or improved treatments.
123I-IBZM is an imaging agent used to image the postsynaptic D2 or D3 DA receptors of the brain that are located in the area of the striatum (9) (Fig. 5).

Transaxial 123I-IBZM images show cortical uptake and specific binding to D2 or D3 DA receptors. Striatum is well visualized with this radiotracer because of high density of DA receptors in region. Focal areas of activity inferiorly in image are external fiducial markers placed along canthomeatal line.
Uptake of the radiotracer is greater and more stable in this area than in other areas of the brain because of the abundance of receptors that are located here. Some uptake within the cortex of the brain is also seen. This activity reflects nonspecific, unstable binding of the tracer that will washout rapidly in comparison with striatal uptake.
This agent can be used in the study of cocaine dependence, bipolar and obsessive-compulsive disorders, and schizophrenia. Using schizophrenia as an example, one can obtain images and measurements of the inhibitory effects of antipsychotic drugs on the DA receptors. These drugs are used to reduce schizophrenic symptoms by reducing DA levels in the synapse.
Quantitative information is obtained by kinetic modeling of the specific uptake after bolus injection of the radioligand. An alternative approach is to model the modified pharmacokinetic conditions that result from the steady-state administration of the radioligand. The steady-state administration results in an equilibrium condition between the concentration of radioligand in the blood and its binding to neuroreceptors in the brain (9). Simple semiquantitative ratio measurements of a target-to-background region at a specified time after bolus injection are sometimes used, but this method gives only a gross measurement of receptor density and the ratio is affected by factors unrelated to the number of target states, such as regional blood flow, hydration of the patient, and so forth.
One method used in research clinics for reducing the influence on tracer delivery is to administer the radiopharmaceutical over a prolonged time (hours) until an equilibrium state is achieved at the receptor. This is simply when the rate of the radioligand’s binding to the target site is equal to the rate of the radioligand’s release from the target for tracers that bind reversibly. An initial bolus injection is followed by a continuous intravenous flow of the agent over a period of time until equilibrium is reached.
123I-IOM is another imaging agent that can be used to image the benzodiazepine receptors in the brain (10) (Fig. 6).
123I-IOM uptake reflects distribution of benzodiazepine receptors in cortex of brain. Medications such as diazepam bind to this site.
These receptors, located in the cortex, exert their effect by increasing the inhibitory action of the neurotransmitter GABA on the postsynaptic neuron. This inhibitory effect blocks the firing of the postsynaptic neuron or moderates its strength. Benzodiazepine receptors and GABA together form a complex that is known to be involved in regulation of stress, anxiety disorders, and epilepsy. As an example, in epilepsy there may be insufficient GABAminergic regulation, resulting in excessive and uncontrolled neuron firing (11), which manifests clinically as a seizure.
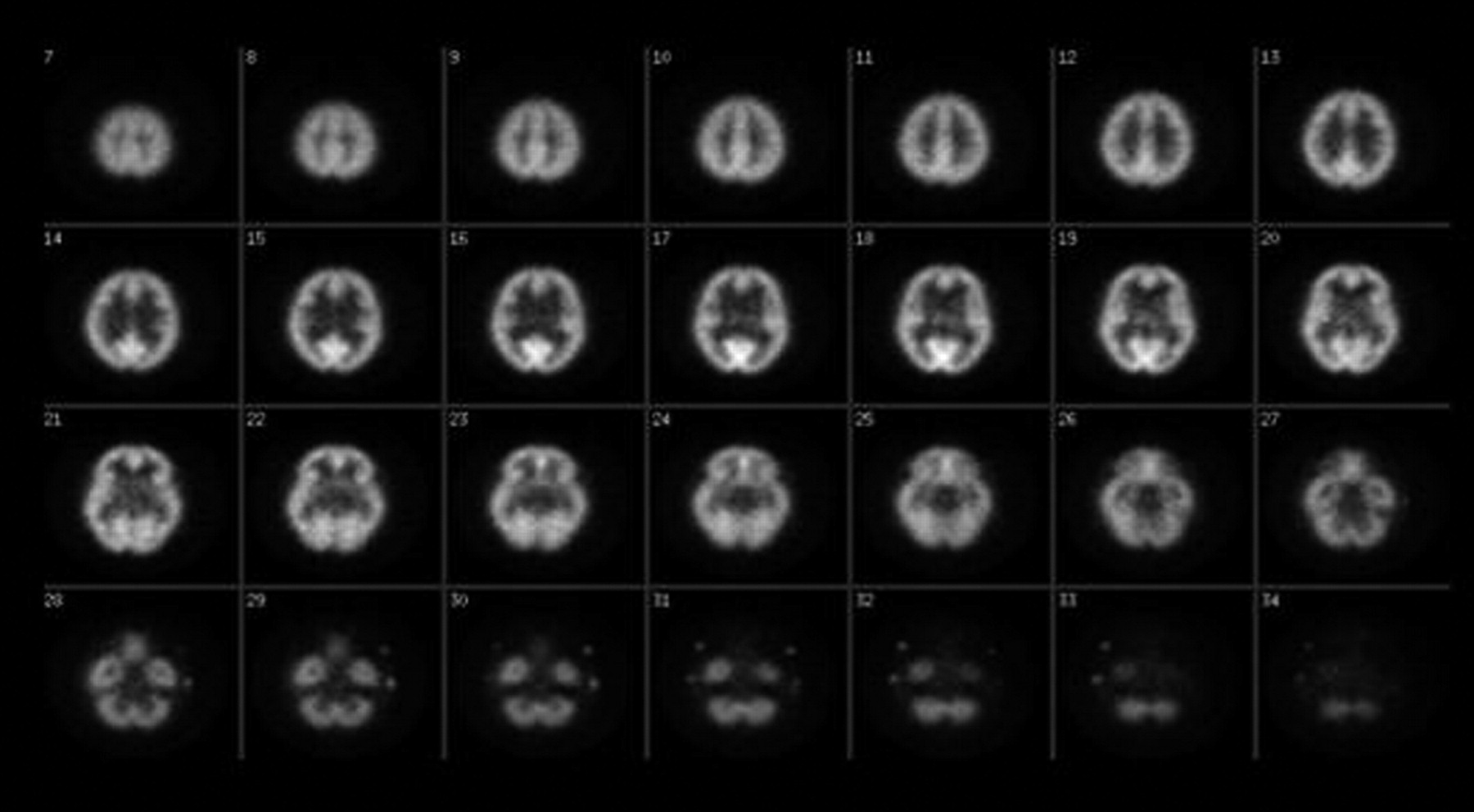
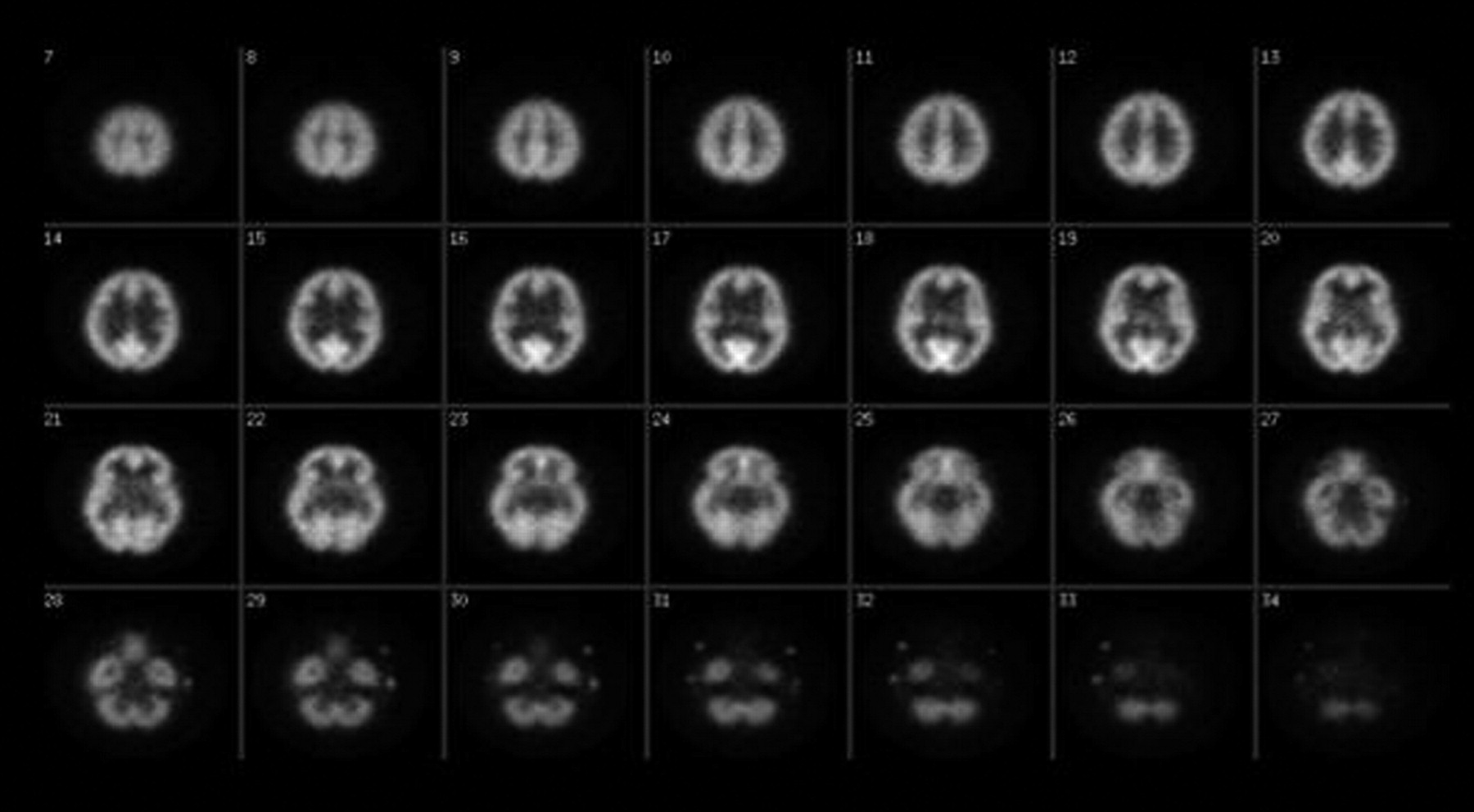
123I-5-I-A is a new radioligand used to image the nicotinic cholinergic receptors located mainly in the area of the thalamus (12) (Fig. 7).

123I-5-I-A distribution within thalamus indicates location of nicotinic cholinergic receptors, where drugs such as nicotine bind.
These receptors are excitatory in nature and are normally activated by a neurotransmitter called Ach. They have been implicated in the mediation of cognitive functions, particularly those associated with Alzheimer’s disease and schizophrenia, and also play an important role in tobacco dependence (12).
When nicotine enters the body, either by smoking or chewing, it activates these receptors because of its chemical similarity to Ach. But unlike Ach, it disrupts the normal functioning of the brain, causing changes in the number and sensitivity of the receptors. These changes may be responsible for the development of tolerance to nicotine as well as its dependence.
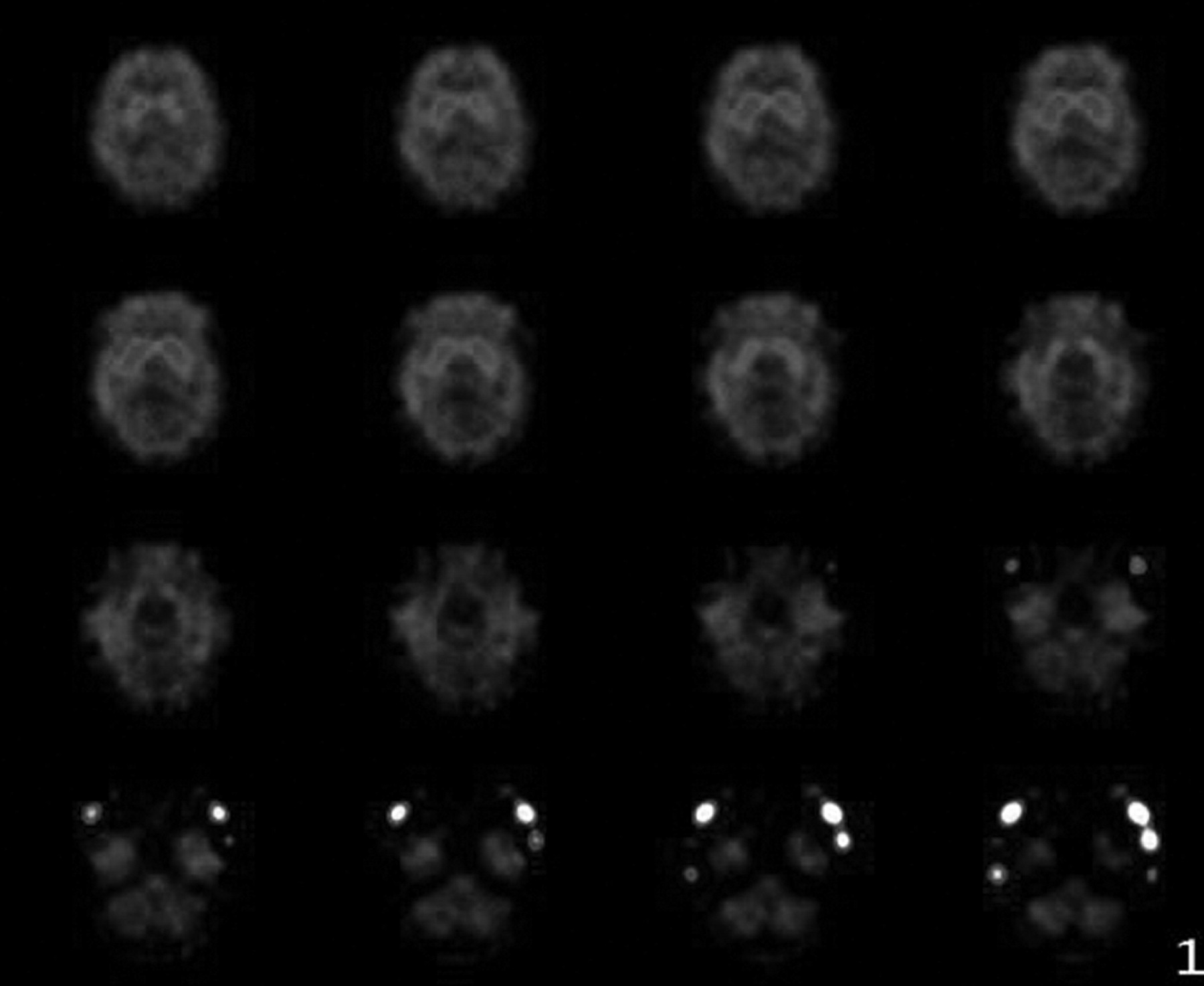
123I-β-CIT is an agent used to image the DA transporters in the presynaptic neurons in the striatum of the brain (13) (Fig. 8).

123I-β-CIT images of neuronal loss over time in patient with Parkinson’s disease. (A) Striatal uptake of radiotracer. (B) Decreased uptake in left striatum.
These transporters regulate the amount of the neurotransmitter DA circulating within the synapse. If there is a decrease in DA-producing presynaptic neurons, there will be a decrease in the amount of DA available within the synapse as well as a decrease in the number of transporter or reuptake sites. The availability of these sites as well as their loss over time can be shown using 123I-β-CIT (13). Therefore, this agent is used as a clinical tool to detect the degeneration of dopaminergic neurons in Parkinson’s disease, in which an unexplained progressive loss of these presynaptic neurons occurs. This and its associated DA loss cause patients to lose control of their movements.
EFFECTIVE TREATMENTS
By researching and studying the processes that occur at the synapse with radioligands, it is possible to formulate drugs that can mimic their affinity for and uptake in specific areas of the brain where they can exert their effects. More important, neuroreceptor radioligands are useful for characterizing new pharmaceuticals that work at similar target sites. For example, in early-phase studies it is possible to evaluate whether a new drug penetrates the blood–brain barrier and binds to the target site with adequate occupancy to suggest a good clinical response. The percentage occupancy of the target site can be used for development of appropriate drug dosing strategies for subsequent clinical trials. The studies are generally performed by obtaining a baseline scan, then treating the research subject for a period of time with the medication of interest (usually after steady state has occurred), and repeating the neuroreceptor scan. The on-medication treatment scan will show reduced uptake of the radiotracer because the target sites are occupied by the treatment drug. Hence, the percentage reduction or displacement reflects the occupancy of the treatment at the target.
A different paradigm using receptor radioligands may also be used to evaluate the effects of a single dose of a drug at the brain target site. In this case, the drug of interest is given after the radiotracer has been administered, and serial dynamic images are obtained to demonstrate the active competition of the study drug with the radioligand. Serial imaging shows the washout of the radiotracer from the brain produced by this competition.
Another application of brain receptor scinitigraphy is the use of the radiopharmaceutical as a biomarker of disease. Large studies of patients with Parkinson’s disease have used the DA transporter ligand 123I-β-CIT as an objective putative measure of disease progression in trials of patients treated with medications that may retard the progression of disease. Although clinical measures of disease are the ultimate standard for assessing the efficacy of neuroprotective treatments, these clinical assessments are confounded by the fact that it is not possible to washout moderately severe Parkinson’s disease patients from their symptomatic treatment. Hence, imaging may provide another measure of disease severity and serial progression. In this regard, adequate algorithms for quantification of the imaging are critical as well as understanding the effects of any treatments themselves on the imaging outcome measures. As an example, antipsychotic drugs that bind to and block the D2 or D3 DA will produce upregulation, or increases, in the number of target sites in the synapse, as the DA system attempts to compensate for the receptor blockade.
The role of receptor-based imaging techniques in the evaluation of these drugs is becoming increasingly important. Ultimately, the information from imaging studies may aid in identification of new treatments and provide a better understanding of the mechanism of the effect exhibited by many central nervous system drugs.
CONCLUSION
Technologic and scientific advancements have made it possible to better understand the brain and its intricate operations. Modern brain imaging techniques allow for noninvasive targeting and monitoring of brain structure and function with the possibility of curing disease or at least improving a patient’s quality of life. Information gained from studies of the brain can halt disease progression or alleviate the associated symptoms. Knowledge of how different medications and disease processes affect the nervous system will help in the development of better treatments and allow for a better prognosis for affected patients.
Acknowledgments
The authors thank Eileen O. Smith for her continuous encouragement in preparation of this manuscript.
Footnotes
For correspondence or reprints contact: Stacey A. Ross, CNMT, RT(N), Molecular NeuroImaging, LLC, 60 Temple St., Suite 8A, New Haven, CT 06510.
E-mail: sross{at}mnimaging.com





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.