


Abstract
Objectives: The increasing use of PET for assessing cerebral blood flow, oxygen metabolism, and blood volume in critically ill patients has created a need for reliable technical solutions for delivering 15O-tracer gases to mechanically ventilated subjects. Our objective was to create such a solution.
Methods: We designed a ventilator add-on unit that enables complex functional brain studies using labeled oxygen and carbon monoxide gases as tracers. The unit manages both steady-state and bolus inhalations, and the latter can be manually initiated using a remote trigger. All parts conducting breathing gases can be sterilized. The unit can be operated during both spontaneous pressure support breathing and volume-controlled ventilation. It supports the standard safety features and alarms of the ventilator and includes an overflow valve in the bolus reservoir.
Results: The count rate curves obtained using the new unit were similar to those from the standard bag-inhalation method.
Conclusion: The unit we describe offers an economical and easily operated solution for providing uninterrupted ventilator treatment while performing PET brain studies, and the provided treatment meets intensive care criteria.
With PET using 15O-labeled water, oxygen, and carbon monoxide, it is possible to noninvasively quantify the main contributors of brain homeostasis: regional cerebral blood flow, regional cerebral metabolic rate of oxygen (rCMRO2), and regional cerebral blood volume. The short half-life (2 min) of 15O enables repeated measurements, which are often crucial in brain studies. Although PET has extensively been used in studying cerebrovascular diseases such as stroke and hemorrhage, the technical details for delivering tracer gases to the subjects are generally poorly documented, especially during mechanical ventilation. With ventilator-dependent subjects, safety during the PET studies is essential. The use of an intensive care ventilator possessing various breathing modes and all the standard alarms and safety features should be preferred over temporary solutions. Uninterrupted ventilator treatment during administration of the gaseous PET tracers is valuable, as interruptions always mean potential hazards due to unintentional hyper- or hypoventilation. To minimize imaging time, the system should also be able to perform a bolus inhalation of 15O2 to enable faster rCMRO2 assessments. Additionally, many factors may alter the subjects’ level of ventilator dependence between the PET assessments. The same setup should be applicable both for spontaneously breathing subjects and for those requiring assisted ventilation. To our knowledge, no publications have yet described the technical solutions that would fulfill all these requirements.
Our aim was to develop an anesthesia ventilator add-on that would enable administration of gaseous PET tracers to conscious subjects during spontaneous face-mask ventilation, as well as to anesthetized, paralyzed, or intubated subjects during mechanical ventilation. The administration needed to be possible both continuously and as a bolus inhalation. The normal operation of the ventilator needed to be undisturbed and all safety features and alarms preserved.
MATERIALS AND METHODS
Initial Resources and Procedures
PET Tracer Production.
The 15O isotope is produced with a Cyclone 3 (IBA) by the 14N(d,n)15O reaction on natural nitrogen gas with 1% oxygen. The 15O2 gas from the target output either is used as such or is processed to C15O in a charcoal oven at 950°C (1). When not needed for administration to patients, the products are directed to a decay coil and a gas disposal unit.
Traditional Tracer Use in rCMRO2 Imaging.
The assessment can use either steady-state inhalation (2) or the bolus inhalation technique described here (3,4). A 500-mL bolus (350 MBq) of 15O2 is collected into a rubber ventilation bag (2 L) connected to a face mask by 1-way valves. On command, the subject actively inhales the bolus and holds the breath for 20 s. Exhaled gases are scavenged to gas disposal.
Tracer Use in Regional Cerebral Blood Volume Imaging.
A 700-MBq (1,000 mL) total dose of C15O is administered as a steady stream (maximum concentration, 0.07%) via a face mask during 2 min of normal breathing (5). Exhaled gases are scavenged to gas disposal.
Standard Features of the Ventilator.
We used a Servo 900C ventilator (Siemens-Elema), which needs an electric power source (alternating current, 220 V) and a hyperbaric gas source for air, oxygen, and (optionally) nitrous oxide. The semiopen (no rebreathing) gas circle system is well suited for delivering radioactive gases, as exhaled gases are ejected to the gas disposal system of the facility. Two types of ventilator breathing are applicable in PET. The first is involuntary, volume-controlled (VC) ventilation. The user sets the minute volume (L/min) and the frequency (/min) of ventilation, and the ventilator calculates the tidal volume (mL). By pressing the inspiratory pause button, one can pause the breathing cycle until the next full inspiration (without bypassing the apnea alarm). In the second applicable breathing type, the ventilator gives pressure support (PS) to assist the subject’s spontaneous breathing. The user sets the triggering sensitivity and the amount of support (cm H2O). The normal safety functions include the apnea alarm (zero pressure in patient circuit for 15 s), user-definable alarms for minute volume and airway pressure, and the safety relief valve of the inspiratory circle.
The New Tracer Delivery Unit (TDU)
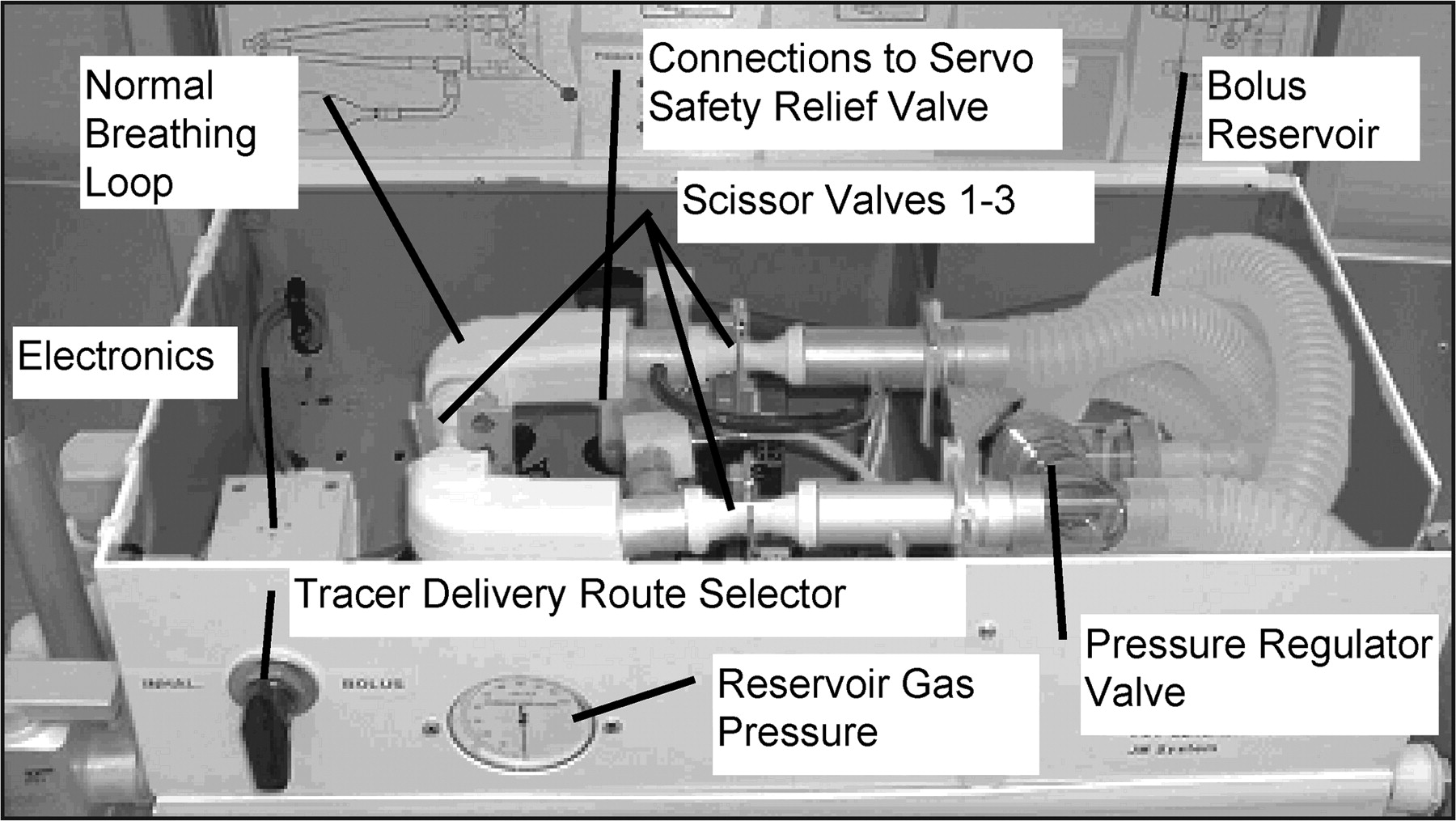
To avoid modifying the original ventilator shown in Figure 1B, only the safety relief valve was customized. All gases coming from the bellows were redirected through the TDU by blocking the original duct to the relief valve and by adding new connector pipes on either side of the blockade (Fig. 1A). Hence, all the pneumatic and electronic devices of the TDU (Fig. 2) could be accommodated into a spare casing attached to the lid of the ventilator. Most parts of the TDU are original spare parts from the manufacturer, and all parts conducting gases can be sterilized.
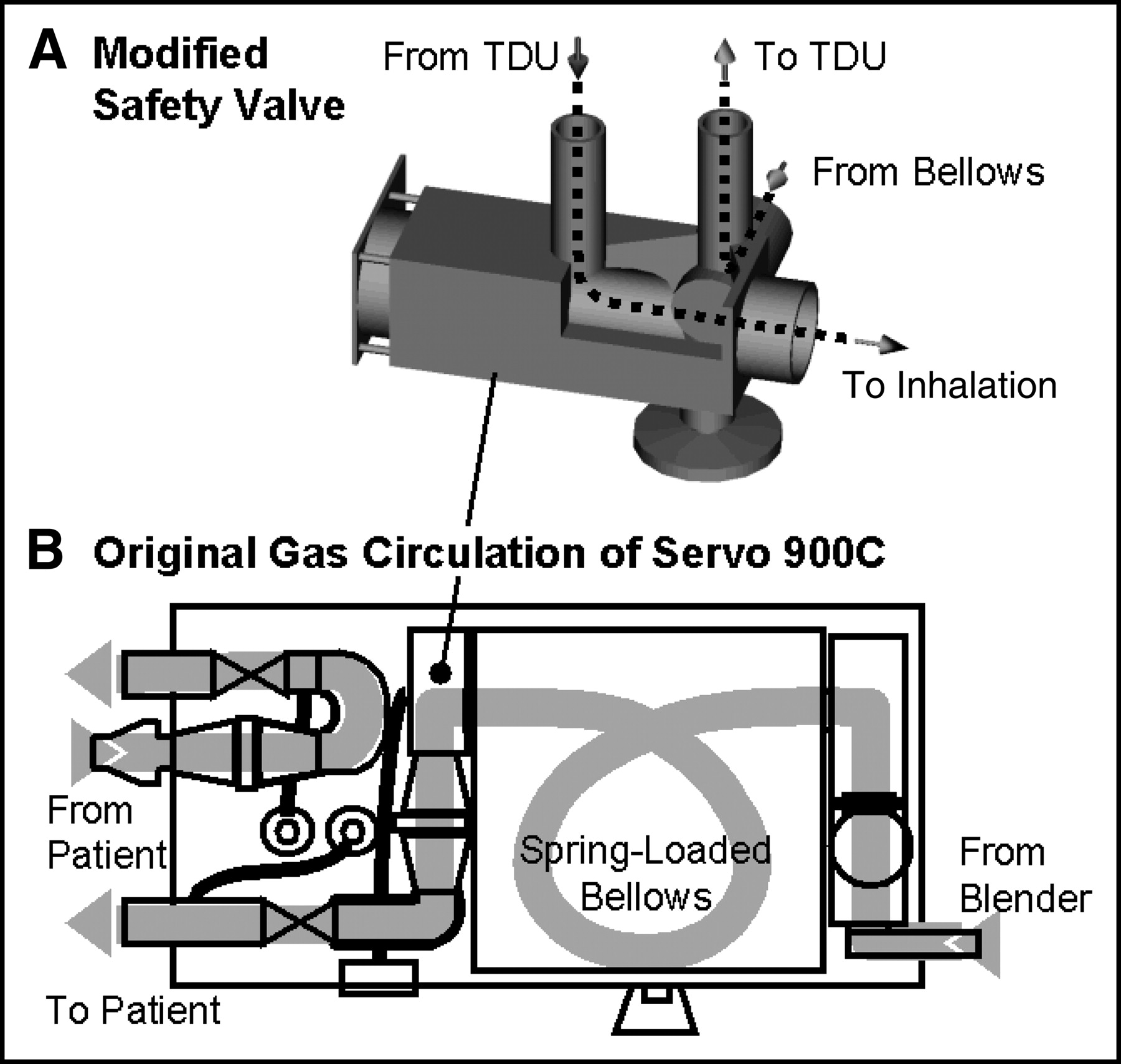
Diagram of the travel of breathing gases in the standard ventilator. The inhalation produced by the bellows passes via the safety relief valve into the patient circle. (A) The safety relief valve modified by attachment of 2 new ducts. The first duct is a custom-made L-shaped pipe that reroutes gases from the bellows straight into the TDU. The gas returning from the TDU enters the safety valve via the second new connector and passes through the valve into the patient circle, retaining the safety function of the valve. (B) The original configuration, which can easily be restored by interconnecting the 2 new ducts with silicone hose, thus bypassing the TDU.

The new TDU, enclosed in spare pneumatic casing. The production line of tracer gases is attached to the tracer delivery route selector. This selector directs the tracer gas either into the short normal breathing loop (for continuous administration) or into the scissor valve controlled reservoir (for collecting the tracer gas bolus). The pressure in the reservoir is displayed on the manometer, and a pressure regulator valve maintains the pressure at a level below the working pressure of the ventilator.
To manage both steady-state and bolus inhalations, 2 optional routes were constructed. The tracer gas from the production line was taken through a delivery route selector to the tracer gas inlet of either route. Standard PS or VC ventilation can be performed without affecting any features of the ventilator, and breathing gases pass through the short route while the reservoir remains isolated by scissor valves (Fig. 3A). C15O can also be administered by turning the delivery route selector to the continuous position, presuming that proper tracer production is online.
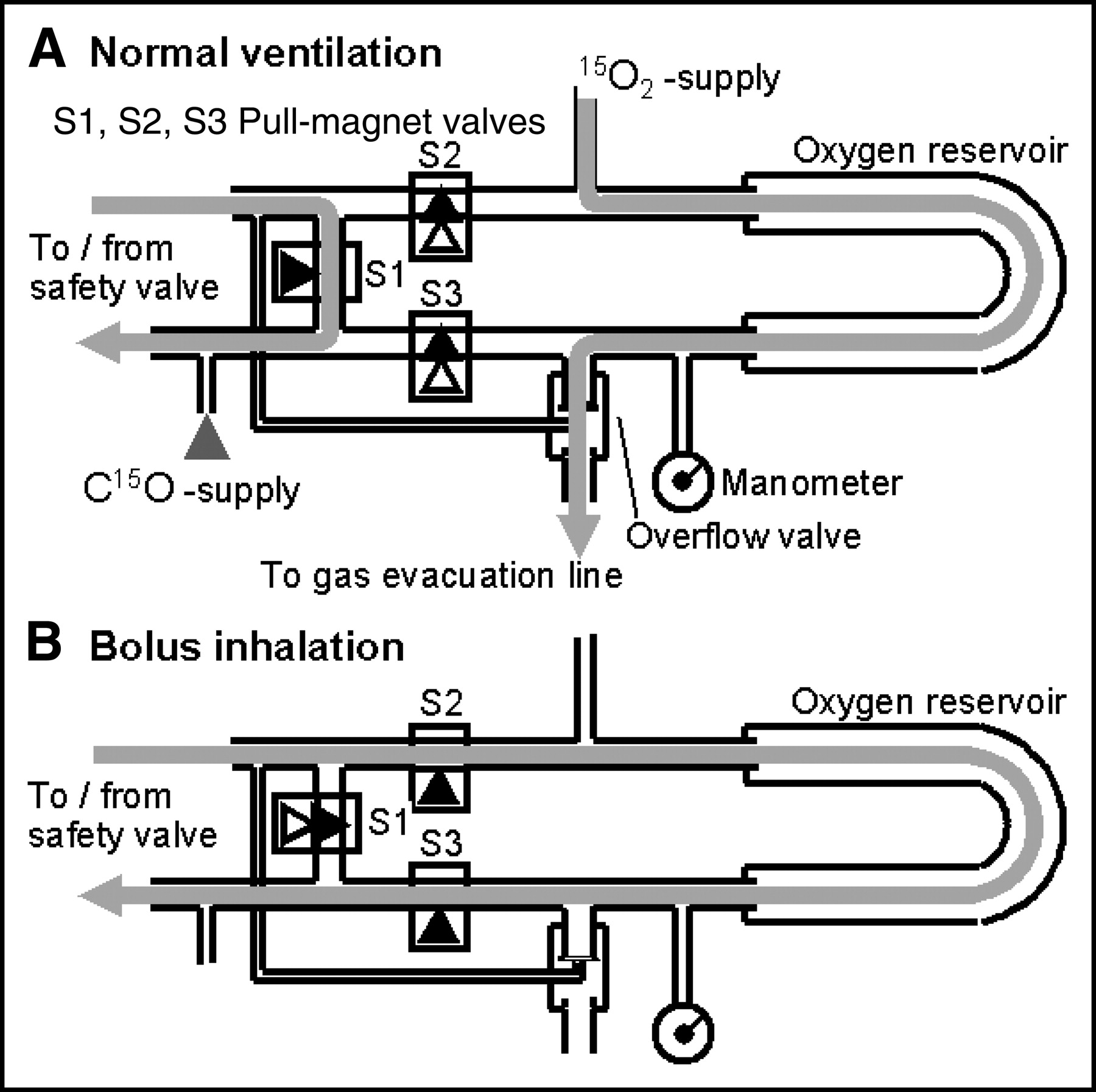
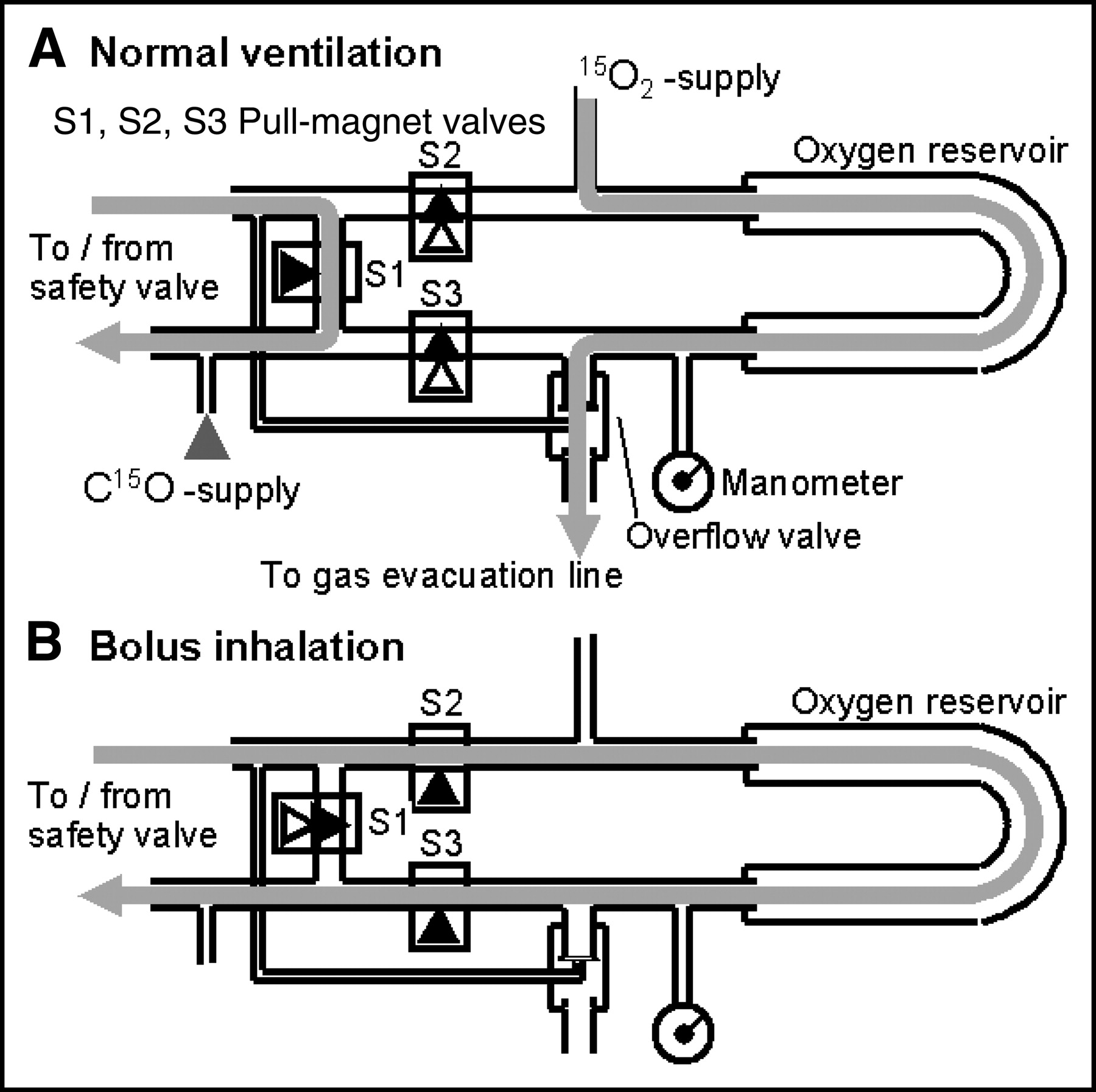
(A) During standard VC or PS ventilation, the breathing gases from the bellows are directed via an open scissor valve S1 back to the ventilator. Steady-state inhalation of C15O does not affect the ventilation. In 15O2 bolus studies, collection does not affect ventilation. (B) For delivery of the 15O2 bolus during VC or PS ventilation, the unit is manually triggered into the bolus delivery mode, causing the next inhalation to pass through the reservoir into the ventilated subject.
The bolus can also be collected without affecting the ventilation by turning the delivery route selector to the bolus position (Fig. 3A). The bolus reservoir constitutes the main part of the long route. It is made of ordinary disposable corrugated ventilation tubing (207 mL/47-cm segment). The reservoir was equipped with a pneumatic overflow valve (Lifecare PLV; Respironics) to ensure that the reservoir pressure (displayed by the manometer) remained below the working pressure of the ventilator and to direct the excess gases to gas disposal. After collecting for a predefined time to achieve the desired bolus volume, the user can trigger the TDU into the bolus delivery mode using a remote push button. The control electronics will then, during expiration, swap the configurations of the 3 TDU scissor valves, directing the next inhalation through the reservoir (Fig. 3B). This feature enables the subject, during PS breathing, to actively inhale when instructed. During VC ventilation, however, the TDU electronics also increase (defined with an adjustable resistor) the tidal volume and activate the inspiratory pause until the trigger button is released. The electronics shown in Figure 4 that also drive the pull-magnet scissor valves were connected to the serial connector N28 of the ventilator and were thus powered by the ventilator.
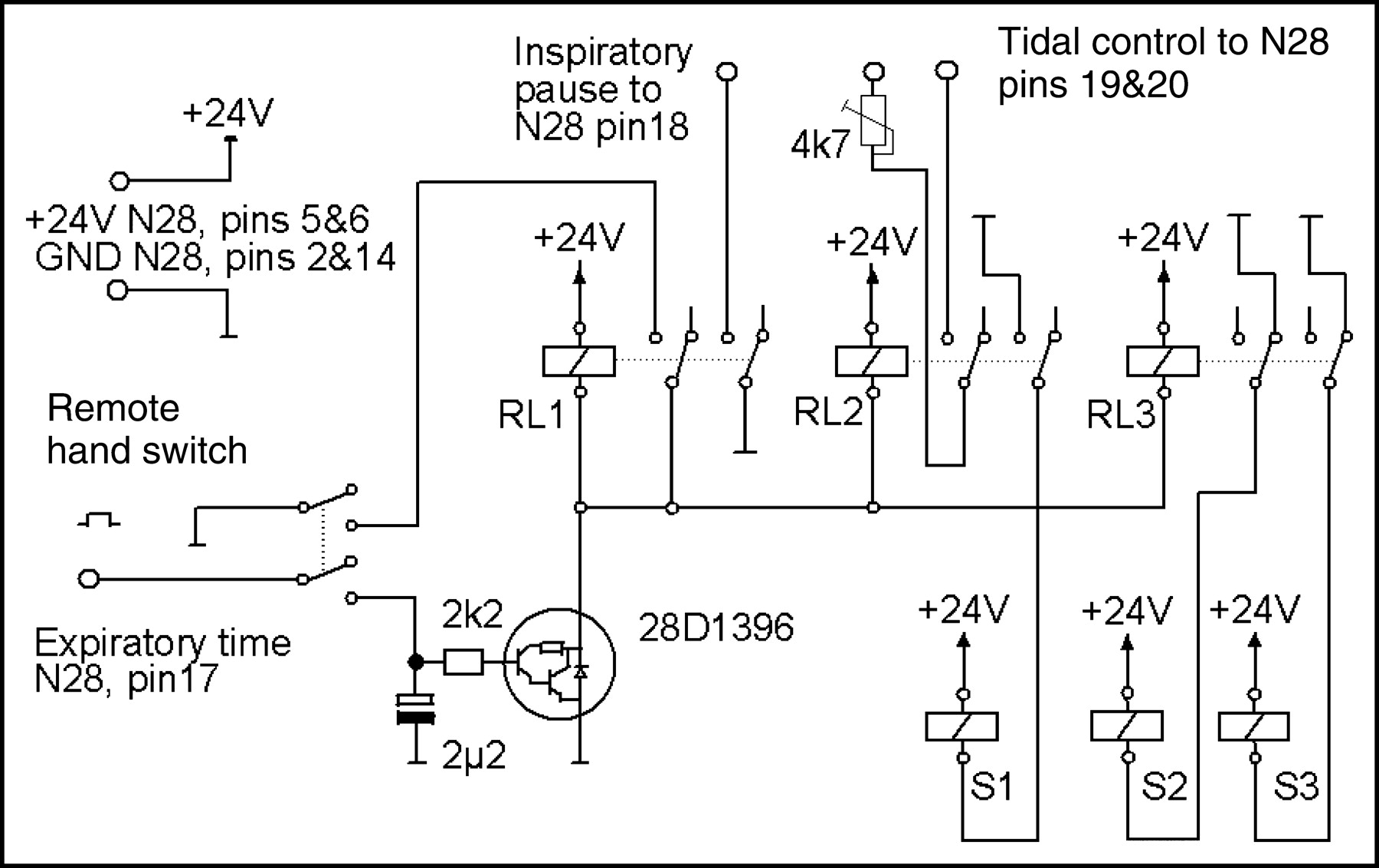
The control electronics of the TDU are connected to serial port N28 of the ventilator. The remote trigger switches the TDU into bolus delivery mode. If the expiration-phase signal is present in pin 17, the relays RL1–3 change the open/closed status of the pull-magnet valves S1–S3, redirecting the next inspiration through the reservoir. If the ventilator is performing VC type ventilation, the tidal volume setting (pins 19 and 20) is increased (by the resistor) and the inspiratory pause (pin 18) is activated until the trigger is released.
Before clinical use, the performance and patient safety of the modified ventilator and the TDU were inspected by certified ventilator maintenance personnel of Turku University Hospital. Compared with the functions of the original ventilator, the functions of the modified ventilator were altered only during active delivery of the bolus, and even then the standard alarm and safety features were retained. Radioactive insulation of the reservoir was not considered necessary because the remote trigger allows personnel to step away from the ventilator during the 1-min bolus collection.
RESULTS
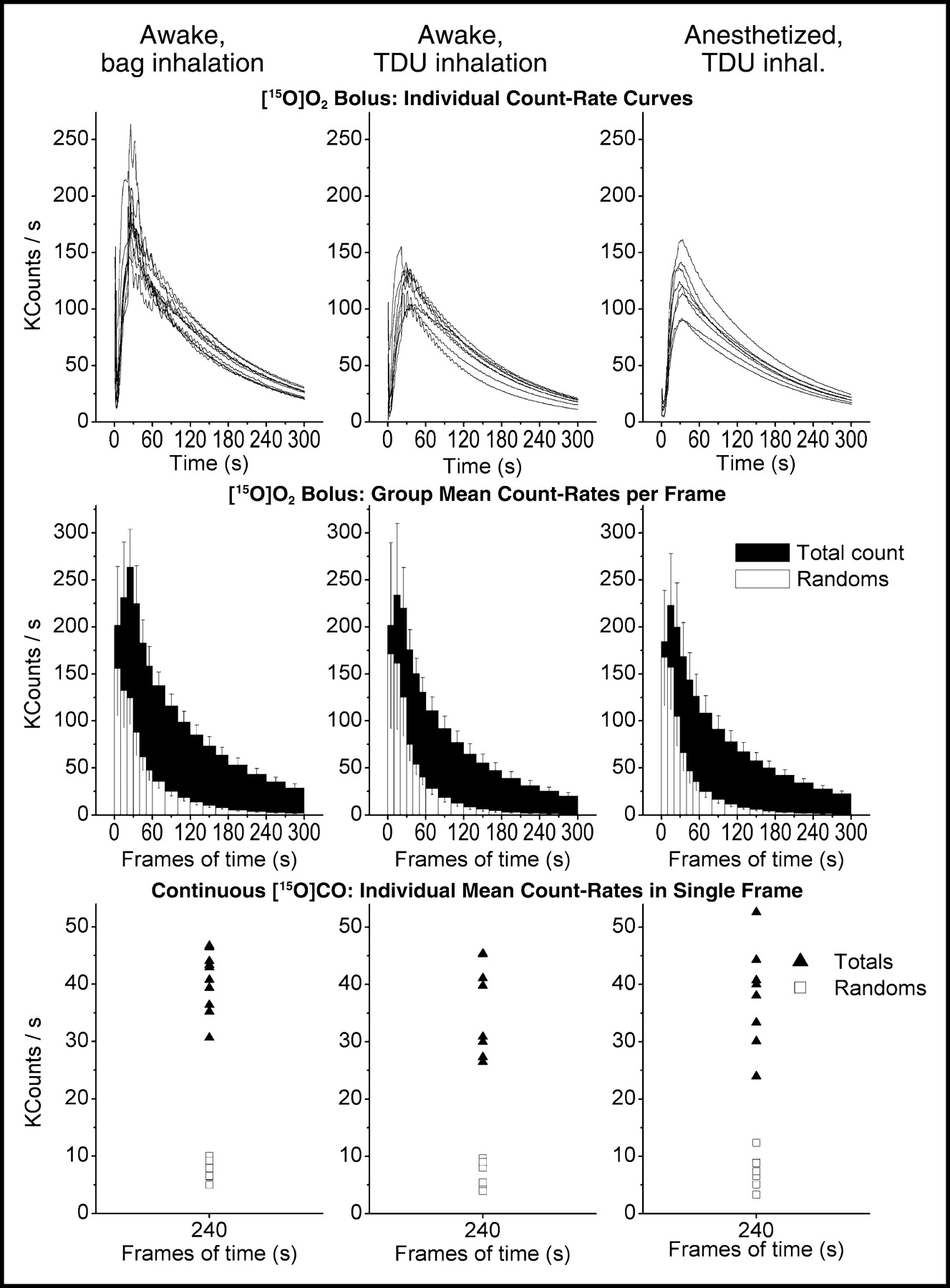
With a 15O2 production rate of 500 mL/min and a 700-mL reservoir volume, no radioactivity was detected in the gas removal line before the 1 min collection (plus 10 s for filling the line) was completed. This finding ensures that the bolus did not leak from the pressure regulator valve before a sufficient volume was achieved. We found the minimum tidal volume for a complete bolus washout to be approximately 1,000 mL, and the electronics were adjusted to double the tidal volume (normally 600–700 mL) of the ventilator during bolus mode. Comparison between the standard administration method (inhalation from a ventilation bag) and use of the TDU during the awake state showed that identical tracer doses (15O2) resulted in similar total count rate curves with the TDU method (Fig. 5). Using the remote trigger, a single investigator could handle both the tracer delivery and the arterial sampling (while also marking the timing of samples with a foot pedal). According to our measurements, the investigator will receive a maximum dose of 0.8 μSv/min using the traditional unshielded rubber bag at a close distance (1.2 m). Using the new TDU at a 3-m distance, the dose would be only 0.13 μSv/min without any insulation.
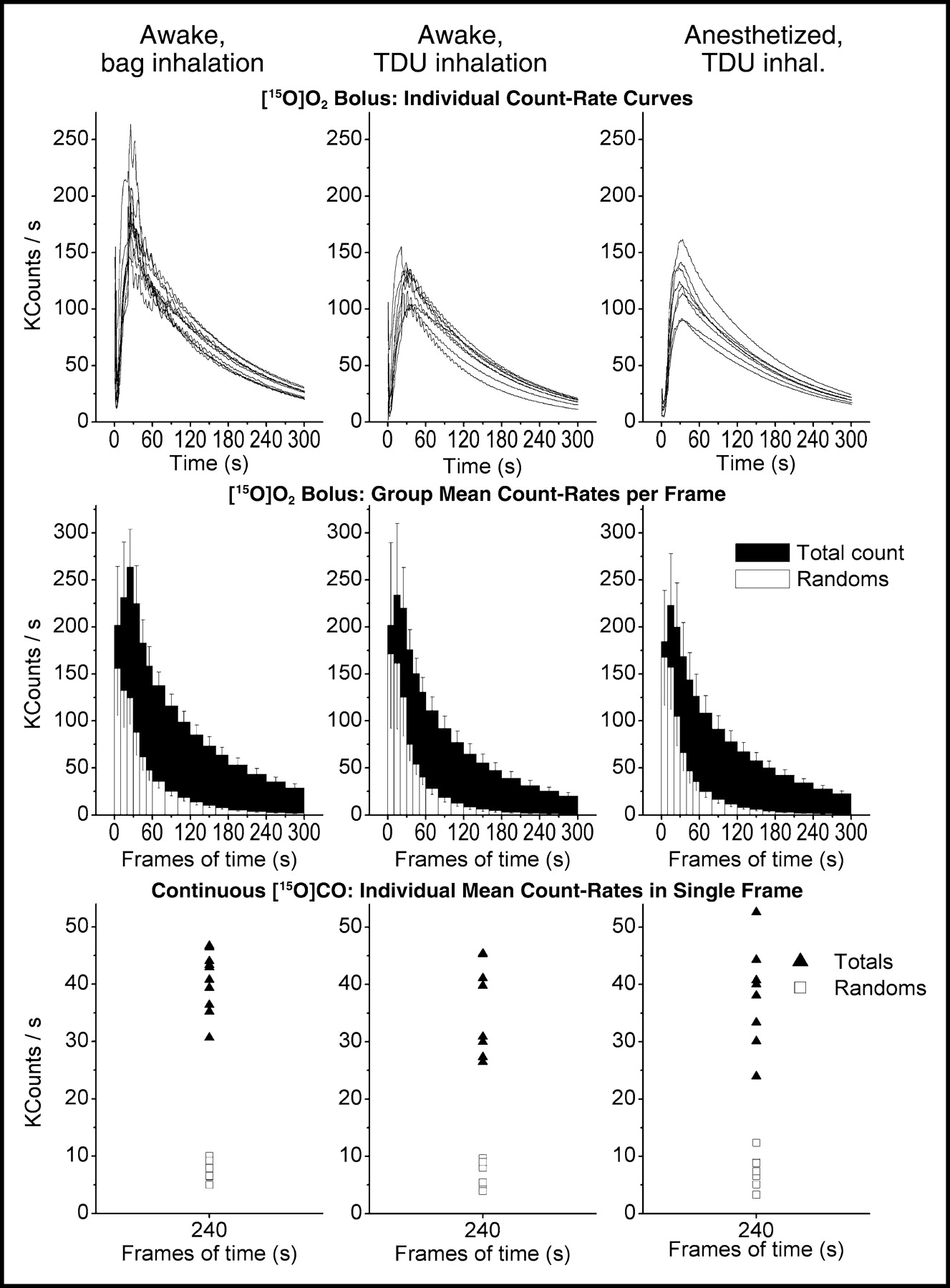
Comparison of detected counting rates after tracer delivery using 3 different dosing methods: spontaneous inhalation from bag (left column, n = 10), ventilator-assisted spontaneous inhalation using the TDU (middle column, n = 8), and involuntary inhalation in mechanically ventilated, anesthetized, or paralyzed subjects using the TDU (right column, n = 8). Counting rates after 15O2 bolus are seen in the top (continuous individual rates, corrected for dead time and randoms) and middle rows (group mean ± SD for total and random counting rates in each frame). The bottom row shows individual mean rates of total and random counts during the single 240-s time frame after 2 min of C15O inhalation.
DISCUSSION
For optimal performance, a few things must be kept in mind. Detailed instructions and brief prestudy training are required to ensure the subject’s ability to breathe normally (i.e., to avoid hyperventilation) during measurements taken while the subject is awake, despite the PS from the ventilator. Because of the short half-time of 15O, the inhalation should also occur immediately after the bolus collection has been completed. Furthermore, the investigator should have an unobstructed view of the chest and epigastrium of the subject to accurately detect the phase of breathing and to trigger the TDU in end-expiration.
CONCLUSION
The results obtained with the new construction match those obtained with the standard method. Furthermore, repeated measurements of rCMRO2 and regional cerebral blood volume are now equally safe and easy to manage during spontaneous, partially assisted, or mechanical ventilation. Uninterrupted ventilator treatment of critically ill patients is thus ensured, and the possibility opens of changing the level of ventilation support—particularly helpful for studying the effects of drugs or procedures that may suppress breathing.
Footnotes
For correspondence or reprints contact: Kaike K. Kaisti, MD, Turku PET Centre, P.O. Box 52, FIN-20521, Turku, Finland.
E-mail: kaike.kaisti{at}tyks.fi





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.