


Abstract
The method of quality control (QC) described on the package insert for 99mTc-tetrofosmin requires meticulous attention to technique for accurate radiochemical purity results. About 30 min are needed. Other proposed methods have been validated only with pertechnetate. We developed a convenient new method using silica cartridges.
Methods: A silica cartridge with 70:30 methanol:water was determined to be acceptable. The method was validated against sodium pertechnetate (99mTcO4), 99mTc-glucoheptonate, 99mTc-sulfur colloid, and low-purity 99mTc-tetrofosmin. The validations were made by using a small volume of concentrated 99mTcO4 with expired kits. Instant thin-layer chromatography (ITLC) showed 6 impurities after an hour or two. The effects of sample size and flow rate were determined. The precision of repeated tests was determined by comparison with the results of 8 replications on the same batch. The 2 methods were compared at a hospital and at 2 commercial nuclear pharmacies, for a total of 134 replications, with 21 preparations being of <90% radiochemical purity.
Results: Volumes between 25 and 100 μL did not affect the silica-cartridge method but did affect the ITLC method. Flow rate is critical and must be ≤5 mL/min with the silica cartridges. The SD and variance by ITLC were 7 and 51 times larger, respectively. Using the package insert technique as the gold standard, all batches of <90% radiochemical purity were rejected and those of >90% radiochemical purity were accepted. Linear regression gave the following equation: ITLC = 1.0051 × silica cartridge (R = 0.99). One- and 2-binned χ2 analyses gave P values > 0.999999. A 2 × 2 contingency table showed 100% sensitivity, accuracy, and specificity, with a Fisher’s exact test P value of 5.7 × 10−25. Correlation was nearly perfect.
Conclusion: According to the published rating criteria for alternate radiochemical purity tests (American Pharmacists’ Association), the silica-cartridge method has a score of 90.2, versus 65.8 for ITLC. On the basis of published criteria for alternate radiochemical purity testing methods, the new method is clearly seen to be superior. Furthermore, alternate methods were validated only with free 99mTcO4 and colloidal impurities. We showed that these are not the significant radiochemical impurities with 99mTc-tetrofosmin and that those methods are not valid. This new method is fast, convenient, accurate, safe, and economical, but careful control of flow rate is required.
The instant thin-layer chromatography (ITLC) method of quality control (QC) described on the package insert for 99mTc-tetrofosmin is slow and requires particular attention to technical details to achieve accurate results. The 30 min or more needed for the entire process is not practical in a demanding nuclear medicine environment where timely injection of patients is critical. This time commitment and inaccuracy can result in delays and increased costs because of additional vial reconstitutions and repeated scans.
Motivated by these problems with the ITLC method, we have developed a new analytic method for separating potential impurities from the desired complex. We have completed approximately 100 trials using Sep-Pak column (Waters) chromatography with different media (silica, alumina N, and C-18) and various concentrations and combinations of solvents (saline, water, methanol, acetone, ethanol, isopropanol, dichloromethane [also known as methylene chloride], and acetonitrile) to develop a new procedure, which was then rated according to published criteria for alternate methods of radiochemical purity testing (1).
Ethanol successfully separates pertechnetate (99mTcO4−) from the desired complex (2) but fails to discriminate other commonly found impurities. We found a silica-cartridge technique that accurately quantifies all common impurities identified by the method on the package insert. This paper describes our technique, along with its validation and clinical importance.
MATERIALS AND METHODS
The following procedure was used for each experiment. First, a silica cartridge was slowly equilibrated with 5 mL of normal saline followed by 1 cm3 of air. Second, 50 μL of sample were loaded onto the longer-necked side of the column, with care taken to place the sample on the column and not in the tube neck. Third, 10 mL of 70:30 methanol:water were pushed dropwise through the column into a test tube at a flow rate of 5 mL/min (the maximum rate according to the manufacturer; purity is underestimated if this rate is exceeded). We used a syringe pump (model 200 series pump; KD Scientific) to control this flow rate while developing the method. Finally, the cartridge was placed in a second test tube and each tube was assayed for 99mTc activity in a dose calibrator. The package-insert ITLC method was used as a control for each experiment. Pipettes were used to control sample spot size and measure solvent, and strips were counted with an Instant Imager (Packard BioScience Co.) to accurately determine the percentage of activity that lay between an Rf of 0.2 and 0.8.
Experiment 1
The first experiment determined the behavior of sodium pertechnetate (99mTcO4) (molybdenum–99mTc generator; Bristol-Myers Squibb) on silica cartridges using 70:30 methanol:water as an eluent. The silica-cartridge procedure was repeated 5 times using different 99mTcO4 samples.
Experiment 2
The second experiment determined the behavior of 99mTc-glucoheptonate on silica cartridges using 70:30 methanol/water as an eluent. 99mTc-Glucoheptonate (Mallinckrodt Medical) from commercial kits was used as a surrogate for gluconate. The silica-cartridge procedure was repeated 4 times using different 99mTc-glucoheptonate samples.
Experiment 3
The third experiment determined the behavior of high-purity 99mTc-tetrofosmin Tc(V)O2(TF)2 on silica cartridges using 70:30 methanol:water as an eluent. The silica-cartridge procedure was repeated 4 times using different high-purity 99mTc-tetrofosmin Tc(V)O2(TF)2 samples.
Experiment 4
The fourth experiment determined other impurities on silica cartridges using 70:30 methanol:water as an eluent. A low-purity batch of 99mTc-tetrofosmin was prepared by using expired 99mTc-tetrofosmin kits (which had not been refrigerated) and adding high concentrations and small volumes of 99mTcO4. This method resulted in a preparation in which 5–6 different impurities were identified on ITLC and that degraded rapidly over the course of 2–3 h. The same impurities were reproducible, but the relative amount of each impurity was not. The silica-cartridge procedure was repeated 11 times using different low-purity batches of 99mTc-tetrofosmin.
Experiment 5
The fifth experiment validated the separation method. The silica-cartridge procedure was repeated 134 times using different 99mTc-tetrofosmin samples of varying purity, including 21 preparations of <90% purity. These samples included clinical batches sampled at various times until 36 h after preparation. Seventy of these trials were eluted by hand, rather than by using a syringe pump to control the flow rate. These trials were performed at pharmacies of Amersham, which used its routine ITLC method as a control. Correlation between the silica-cartridge method and the insert method was analyzed using a 1- and 2-binned-data χ2 test and a 2 × 2 contingency table with the associated Fisher exact test. An α-value of 0.05 was used to determine the validity of the new procedure.
Experiment 6
The sixth experiment validated the precision of the silica-cartridge procedure. The procedure was repeated 8 times using samples from a single preparation of 99mTc-tetrofosmin.
Experiment 7
The seventh experiment validated the use of the second solvent, 80:20 methanol:saline, for the analysis of colloidal impurities. Various activities of 99mTc-sulfur colloid were mixed with high-purity 99mTc-tetrofosmin. Eighteen samples were analyzed using the 2-solvent system and compared with ITLC analysis or actual activity assays in a dose calibrator. A 2 × 2 contingency table and the Fisher exact test were used to establish validity.
Experiment 8
The eighth experiment validated the reuse of silica cartridges. Twenty-two paired analyses were done using new columns paired with used columns. The used columns had previously been applied up to 5 times for this same procedure over the course of 3 mo. All columns were equilibrated with normal saline as described in the procedure. Linear regression analysis was performed to compare the results for the new and used columns.
RESULTS
Experiment 1
When 99mTcO4 was loaded onto the column and eluted with 10.0 mL of 70:30 methanol:water, 98.9%–100% of the resultant activity came off the silica cartridge and the remaining 0%–1.1% of the activity remained on the silica cartridge. Thus, essentially all 99mTcO4 was removed on elution with 10.0 mL of 70:30 methanol:water.
Experiment 2
When 99mTc-glucoheptonate was loaded onto the column and eluted with 10.0 mL of 70:30 methanol:water, 97.1%–98.3% of the resultant activity came off the silica cartridge and the remaining 1.7%–2.9% of the activity remained on the silica cartridge. This remaining activity, although minute, was thought to be hydrolyzed reduced technetium (HRTc), indicating that nearly all 99mTc-glucoheptonate was removed on elution with 10.0 mL of 70:30 methanol:water.
Experiment 3
When high-purity 99mTc-tetrofosmin Tc(V)O2(TF)2 was loaded onto the column and eluted with 10.0 mL of 70:30 methanol:water, 2.0%–6.0% of the resultant activity came off the silica cartridge and the remaining 94.0%–98.0% of the activity remained on the silica cartridge. Thus, nearly all high-purity 99mTc-tetrofosmin Tc(V)O2(TF)2 remained on the column on elution with 10.0 mL of 70:30 methanol:water.
Experiment 4
When a low-purity batch of 99mTc-tetrofosmin was loaded onto the column and eluted with 10.0 mL of 70:30 methanol:water, 21.5%–37.0% of the resultant activity came off the silica cartridge and the remaining 53.0%–68.5% of the activity remained on the silica cartridge. This finding indicates that impurities were removed on elution with 10.0 mL of 70:30 methanol:water. HRTc was not eluted from the column, but HRTc was not seen on any of the ITLC strips and is not a significant impurity with this radiopharmaceutical.
Experiment 5
The results of 134 elutions using 70:30 methanol:water are shown in Figure 1. These trials included 21 preparations of <90% purity. The 0.99 correlation coefficient shows a strong association between the silica-cartridge method and the insert method (3). Further statistical analysis of the data shows a 1-binned-data χ2 test probability of 0.99999999999993, whereas the 2-binned data χ2 test probability was 0.999999999999991. A 2 × 2 contingency table showed 100% sensitivity, 100% accuracy, and 100% specificity for these 134 trials. The associated Fisher exact test produced a P value of 5.7 × 10−25. One can conclude that each determination of purity using the silica-cartridge method reflected the ITLC purity value.
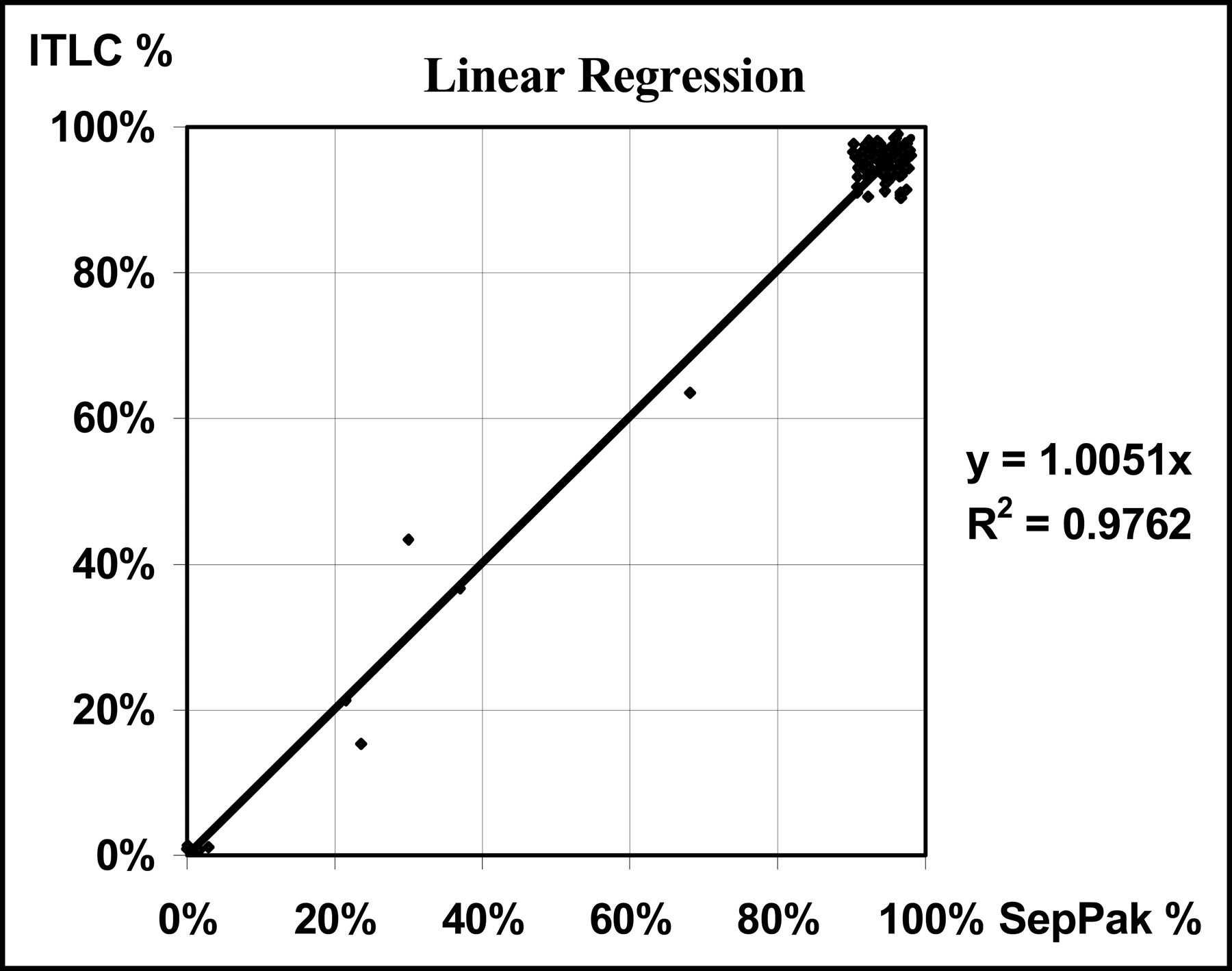
The results of 134 elutions using 70:30 methanol:water. These trials included 21 preparations of <90% purity. The high correlation coefficient (0.99) shows a large strength of association between the silica-cartridge method and the ITLC method.
Experiment 6
The results of 8 QC replications on a single batch of 99mTc-tetrofosmin using 70:30 methanol:water are shown in Table 1. The SD and the sample variance of the ITLC method were 2.08% and 0.044%, respectively. The silica-cartridge method gave an SD and sample variance of 0.292% and 0.001%, respectively. In this experiment, the ITLC had an SD larger by a factor of 7 and a variance larger by a factor of 51. One can therefore conclude that the silica-cartridge method was more precise.
Precision Between ITLC and Silica Cartridge QC
Experiment 7
A 2 × 2 contingency table showed 100% sensitivity, 100% accuracy, and 100% specificity for these 18 analyses. The associated Fisher exact test yielded a P value of 0.00002 and perfect correlation.
Experiment 8
Twenty-two analyses pairing new columns with used columns were performed. The linear regression equation is as follows: old % = (0.992 × new %) − 0.005%, with a correlation coefficient of 0.99. The used columns behaved identically to the new columns and could be reused at least 5 times over a 3-mo period.
These results show that 99mTcO4 and all other common impurities in 99mTc-tetrofosmin were removed from the silica cartridge on elution with 10.0 mL of 70:30 methanol:water. The distribution of impurities changed as a transient 99mTc-tetrofosmin peak degraded into impurities over time. The common impurities from a low to a high Rf, and their associated numbers, are shown in Figure 2. Nearly all the activity of the high-purity 99mTc-tetrofosmin, peak 5, Tc(V)O2(TF)2, remained on the column while the impurities were eluted. Most notably, the results show a strong correlation between QC methods (Fig. 1). In addition to being accurate, the silica-cartridge method was more precise (Table 1).
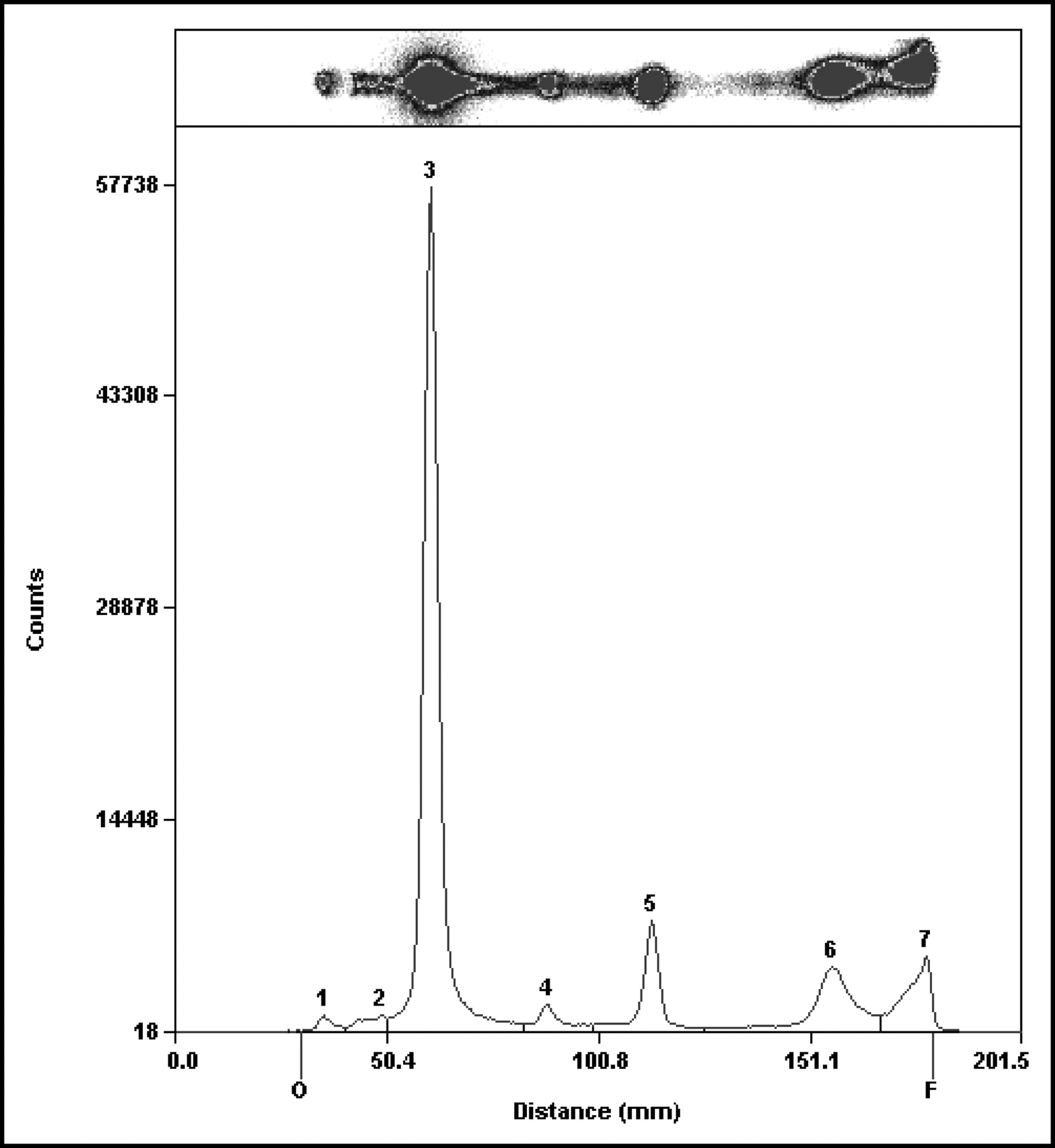
The numbered impurities are 99mTc-gluconate and HRTc (peak 1), unknown (peak 2), reduction impurity (maybe a Tc(IV) product) (peak 3), unknown (peak 4), high-purity Tc(V)O2(TF)2 (peak 5), Tc(III)Cl2(TF)2 or Tc(I)(TF)3 (peak 6), and 99mTcO4 (peak 7). Any variance among Rf values may be large enough to be the difference between the passing and failing of a QC sample with impurities lying near a cut line Rf of 0.2.
DISCUSSION
In clinical practice, radiochemical purity is often measured by thin-layer or paper chromatography (4,5). Column chromatography is an increasingly popular QC method because of its speed, ease of use, and ability to detect an array of radiochemical impurities (1,2,6,7). Radiochemical impurities in 99mTc radiopharmaceuticals can often be separated with column chromatography (4,5,8). In addition, errors associated with other types of chromatography may be reduced (2,6,9,10).
Our new method, as described in the Materials and Methods, leaves a theoretic possibility of contamination by HRTc, although it has not been a significant contaminant with this formulation. If HRTc is suspected, it can be quantified with the following 3 additional steps:
Elute the same cartridge dropwise with 10 mL of 80:20 methanol:normal saline, collecting the eluate in a test tube. The use of normal saline, not water, is critical.
Place the silica cartridge in a test tube. The HRTc will be on the cartridge and the labeled 99mTc-tetrofosmin will be in the 80:20 methanol:saline.
Assay each test tube in a dose calibrator and calculate the purity using the following equation: % labeled = (total activity on the cartridge/total activity) × 100%. The 70:30 methanol:water contains 99mTcO4, 99mTc-gluconate, and the other impurities seen with the package-insert ITLC method. The 80:20 methanol:saline contains all complexes associated with the 99mTc-tetrofosmin peak. The cartridge total contains HRTc and possibly an additional unidentified impurity.
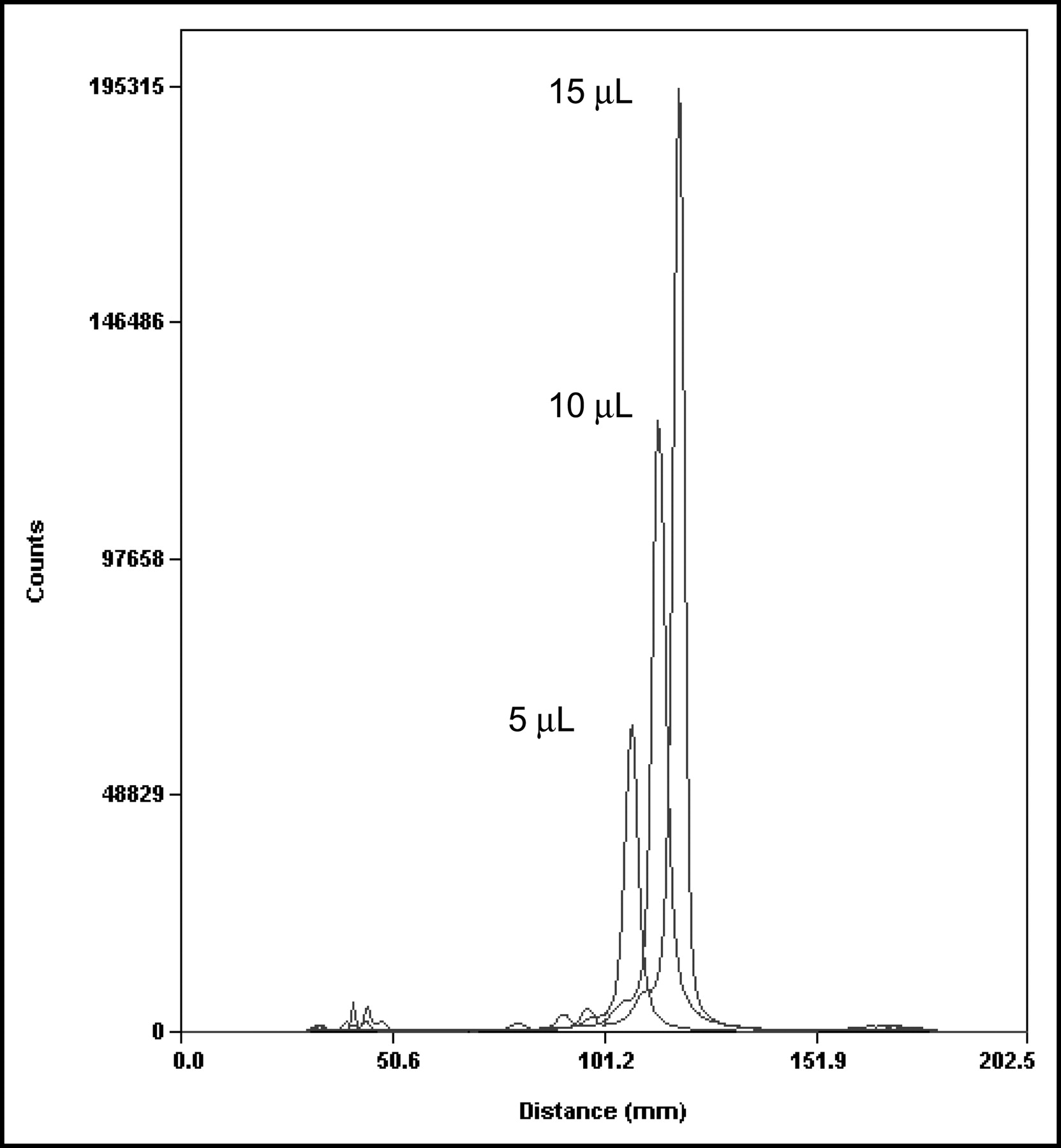
The package-insert method of chromatography for 99mTc-tetrofosmin has several significant limitations. For example, the required sample volume is in the range of 10–20 μL. Figure 3 demonstrates the effect of increasing spot size from 5 to 15 μL. Within this range, the Rf variance may be large enough to mean the difference between the passing and failing of a QC sample when impurities lay near a cut line (Fig. 2). Sample volume is not an issue with the silica-cartridge method. Duplicate runs of 25, 50, 75, and 100 μL gave a narrow range of 96.4%–96.9% in a standard QC test. The Pearson correlation coefficient and z score (−0.128) show that sample volume has little or no effect (P = 0.76). Flow rate is, however, a potential source of error, but not if kept below the maximum of 5 mL/min as stated in the procedure. Table 2 shows the effect of increasing the flow rate past the threshold in the average of 2 runs normalized to ITLC. High flow rates will underestimate purity.
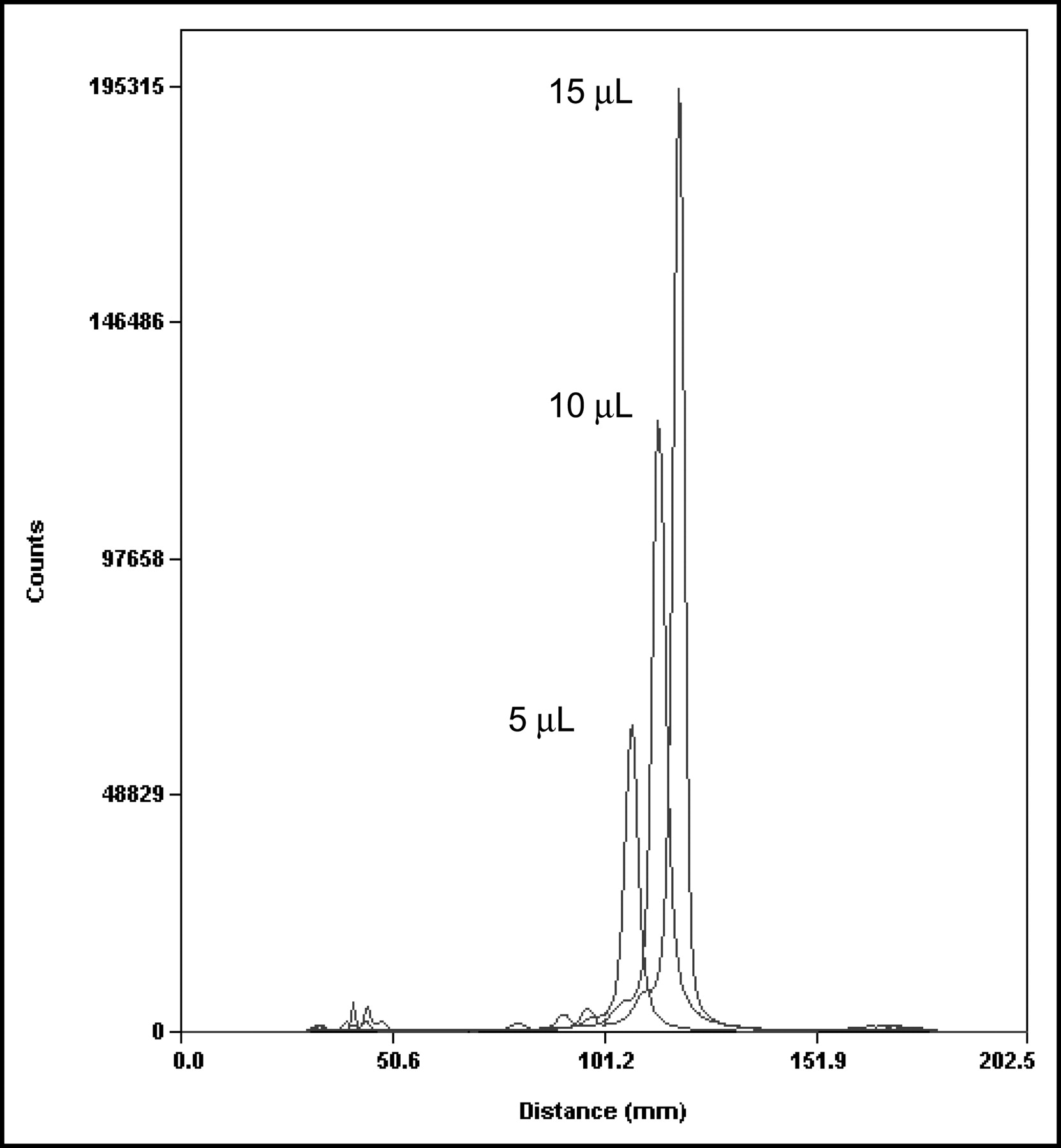
Sample volume effect on ITLC. Five-, 10-, and 15-μL spot size profiles are shown from left to right.
Flow Rate Effect on Silica Cartridge Method
A key to successfully performing the package-insert method of QC is the use of a freshly and accurately prepared solvent, with meticulous attention given to the ratio of acetone to dichloromethane. Any deviation could lead to false results. Dichloromethane poses its own problems as a noxious solvent. It may harm the central nervous system if safety precautions are not observed. A method using solvents that are easier to work with would be advantageous. Stable, common solvents make the silica-cartridge method convenient for QC of 99mTc-tetrofosmin.
Another cause of ITLC failure when using the package-insert method is defective chromatography strips. The source of the problem, although often unknown, may be humidity. Some strips may become damaged to such an extent that heat activation will not rectify the problem. Disparity was commonly seen in our experiment during trials using the same batch of 99mTc-tetrofosmin and the same time, solvent, lot of ITLC strip, and drop size (Fig. 4). This problem is evidenced by the very different Rf values of the peaks as well as the ink used to mark the origin. Heat activation of the medium helped but did not eliminate the problem. When this pattern was observed, the results were discarded and a new heat-activated ITLC strip was used to repeat the analysis.
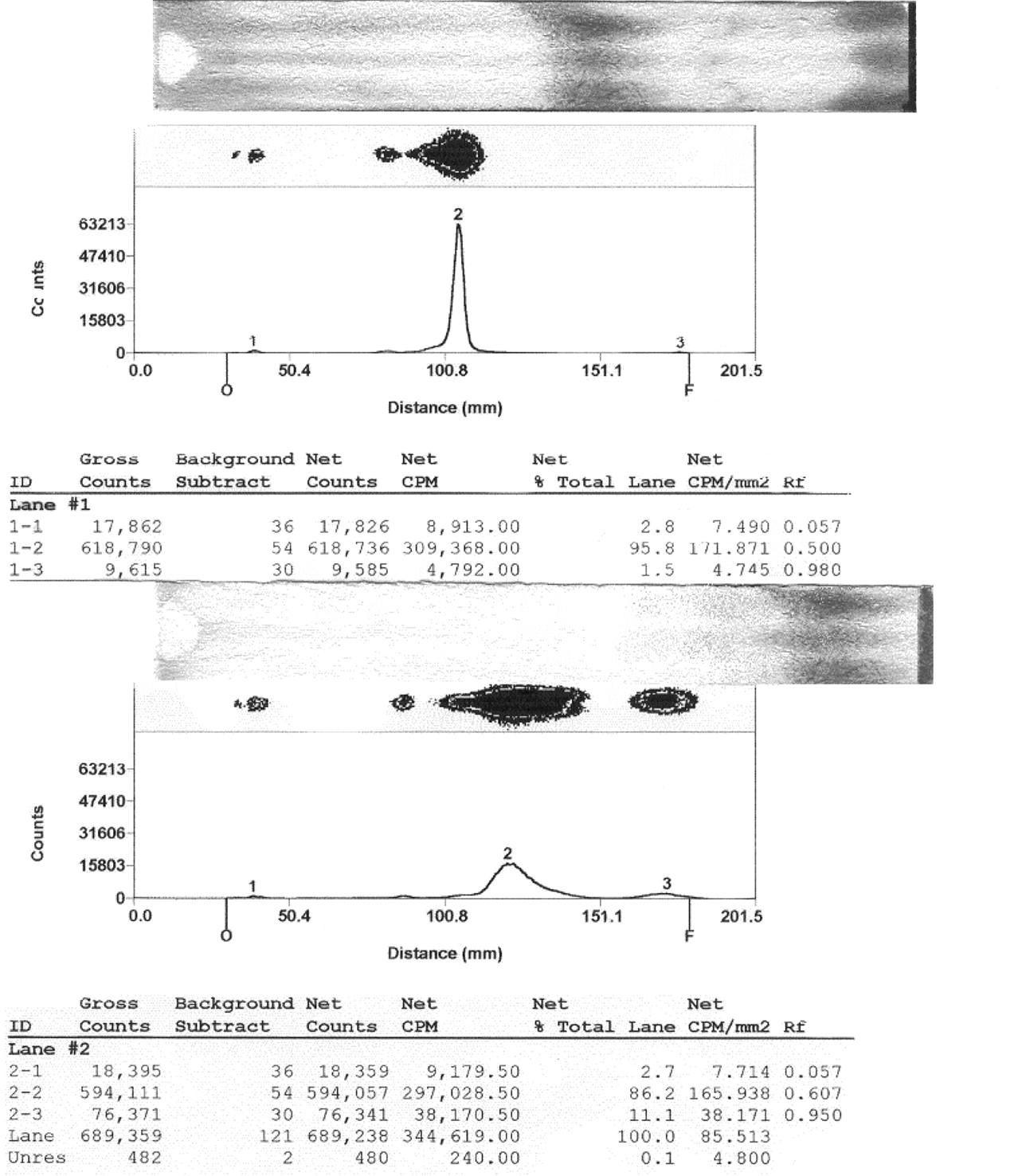
Note the difference in ink color Rf during trials with the same batch of 99mTc-tetrofosmin, time, solvent, lot of ITLC strip, and drop size. Ink had the same variability with and without sample present: 95.8% between Rf 0.2 and 0.8 (top) and 86.2% between Rf 0.2 and 0.8 (bottom).
As proposed by the American Pharmacists’ Association (APhA) Section on Nuclear Pharmacy, the suitability of an alternative method for testing radiochemical purity is determined by a point score based on ability to meet the following criteria: “Fast, ALARA [radiation exposure kept as low as is reasonably achievable], Safe, True, Economical, and Reasonable” (1). Our silica-cartridge technique shows improvements in most of these areas. Using the APhA criteria, ITLC scored a total of 65.8 points, whereas the silica-cartridge method was superior, with a score of 90.2. The ITLC scoring breaks down as follows: a score of 0 for Fast, 2.5 for ALARA, 5.3 for Safe, 55 for True, 3 for Economical, and 0 for Reasonable. The scoring of the silica-cartridge method breaks down as follows: a score of 20 for Fast, 0 for ALARA, 7.2 for Safe, 55 for True, 3 for Economical, and 5 for Reasonable.
The greatest benefit of the silica-cartridge method is the speed with which it can be completed. The package-insert method uses ITLC strips, which take approximately 20 min to develop, and also requires time for preparation of fresh solvent, heat activation of strips, and other setup procedures. Because of the significant time required by the package-insert QC method for development of the ITLC strip, observation of the entire process is not practical. Consequently, one can become tempted to accept a strip on which the solvent front has passed the intended line, despite the potential inaccuracy of such results. In addition, because of the inherent variability with the ITLC procedure, whenever an analysis indicates unacceptable purity the entire process must be repeated using freshly made solvents and heat-activated ITLC strips. Silica-cartridge chromatography with a single solvent can be completed in 5 min. The time commitment and inaccuracy of the ITLC method, with the consequent delays and increased costs due to additional vial reconstitutions and repeated scans, can be eliminated with the silica-cartridge method.
Rest images of the same patient obtained with 99mTc-tetrofosmin preparations of varying purity have shown the importance of a high-purity scan. Figure 5 shows a high-purity scan on the left and a low-purity scan, obtained 3 h after radiopharmaceutical preparation, on the right. Both 99mTc-tetrofosmin samples had passed QC testing 30 min after preparation, yet the lower-purity batch failed to show clinically useful results because of degradation of the 99mTc-tetrofosmin.
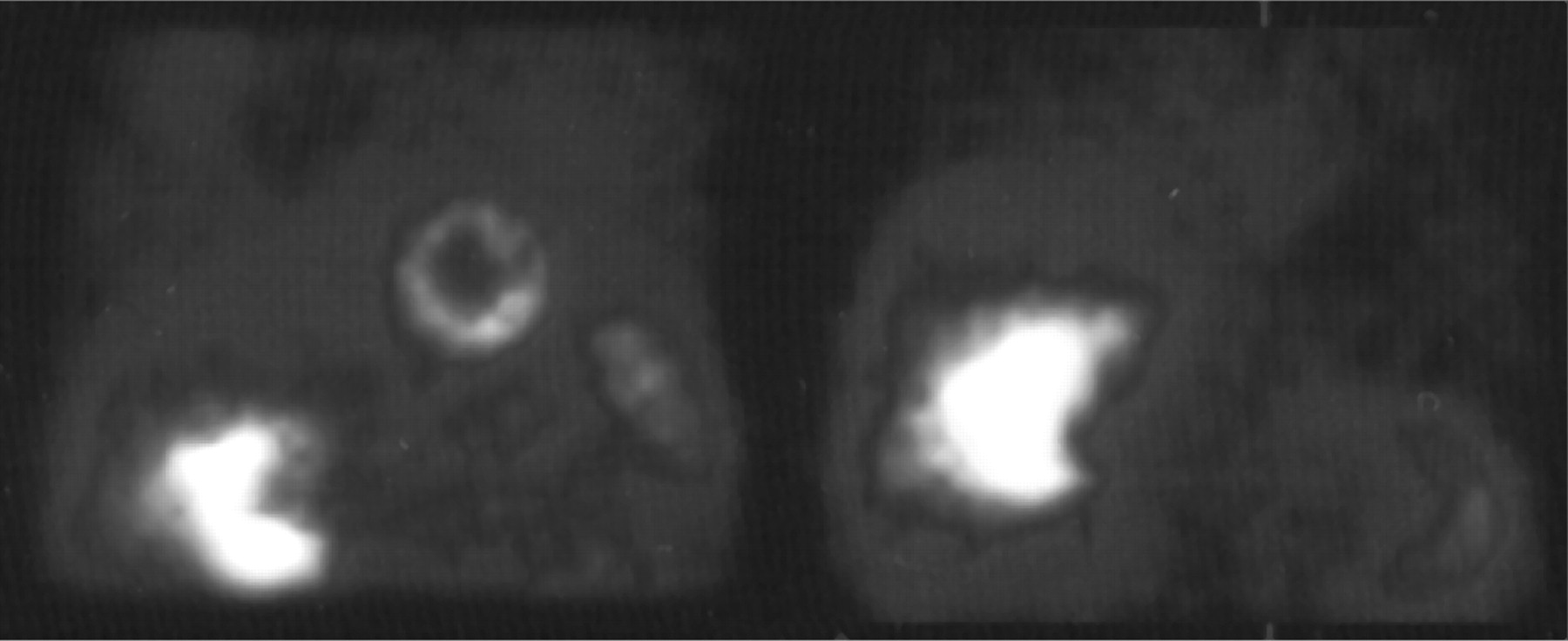
99mTc-Tetrofosmin images of the same patient during rest injections. A high-purity scan is shown on the left, and a low purity, 3-h-postpreparation scan, on the right. Both 99mTc-tetrofosmin samples had passed QC testing 30 min after preparation.
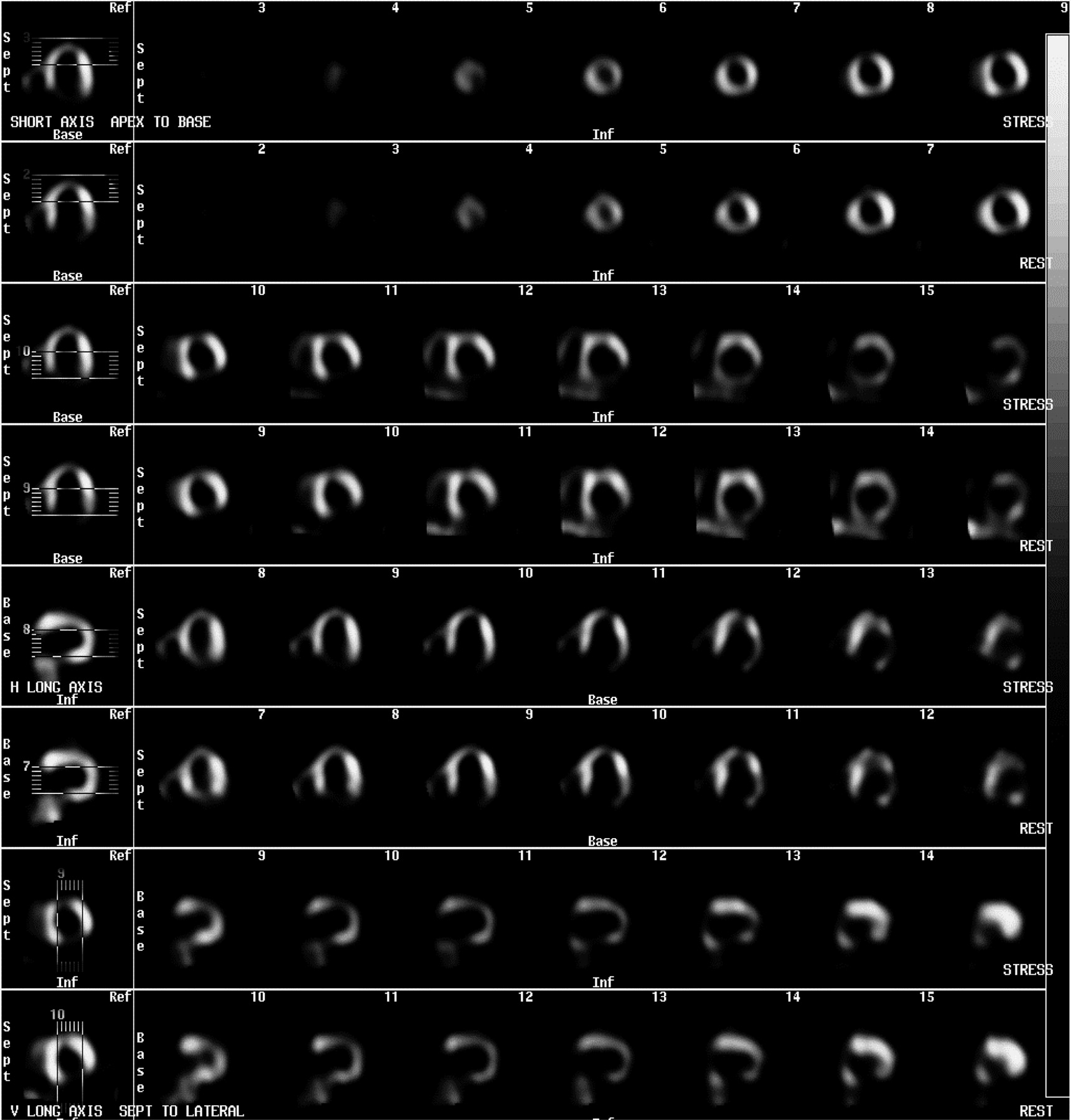
The silica-cartridge method has been shown to have accuracy similar to and precision better than the ITLC method. ITLC strips can fail from unknown causes. Trials in which all variables were identical found drastically different results (Fig. 5). A reduction impurity found near an Rf of 0.2 is likely to be a culprit in failed scans (Fig. 2). The multiple unidentified peaks found between an Rf value of 0.2 and 0.8 (Fig. 6) are not, however, clinically significant (11). The rest/stress myocardial SPECT images seen in Figure 7 used 99mTc-tetrofosmin, which produced the chromatogram in Figure 6. Note that 94.5% of the activity is between Rf values of 0.2 and 0.8 but only 83% of activity is within the main 99mTc-tetrofosmin peak. Three nuclear medicine physicians verified the clinical acceptability of these scans.
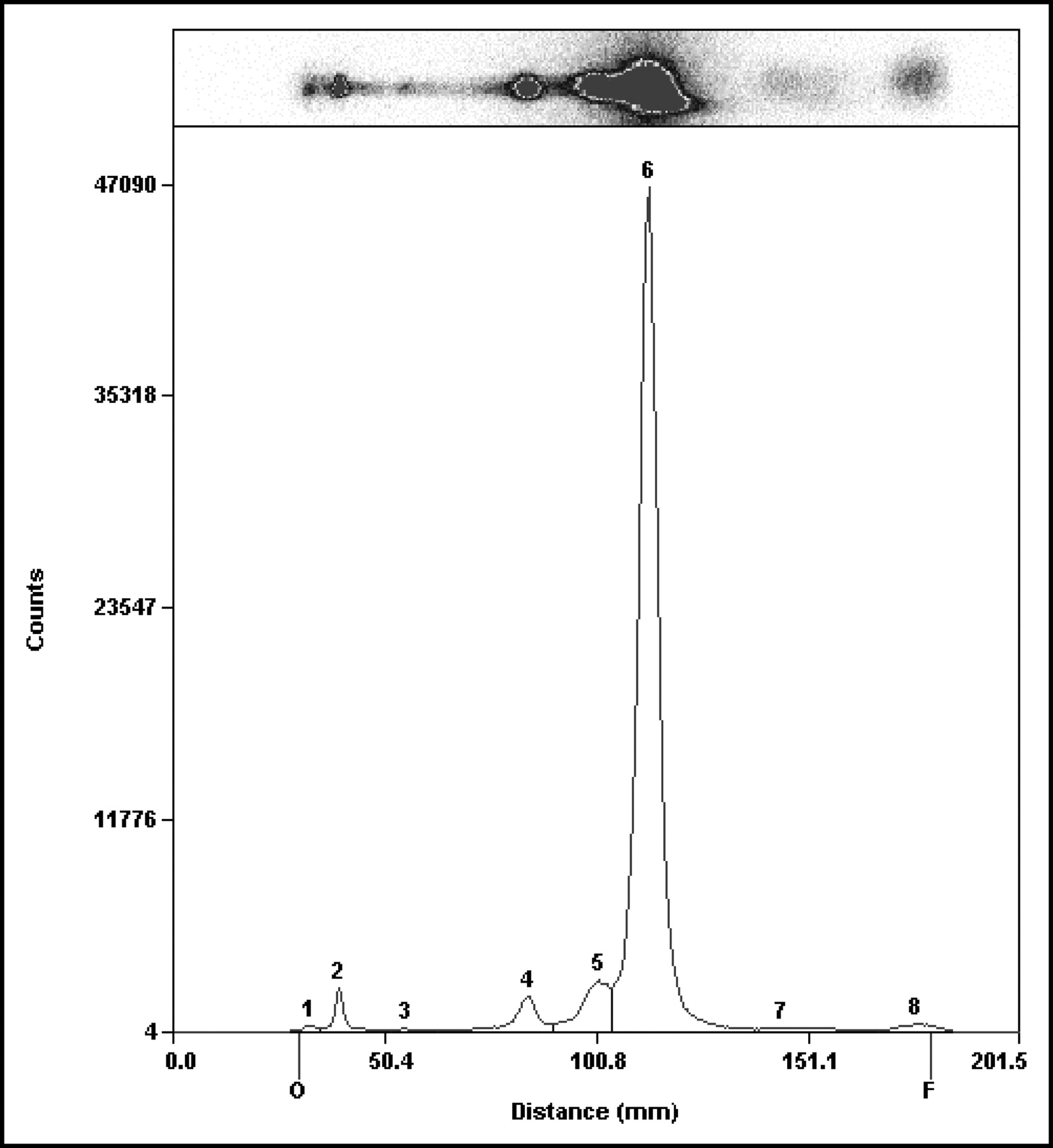
Multiple peaks. Between Rf values of 0.2 and 0.8 lies 94.5% of the activity, whereas only 83% of the activity lies within the main 99mTc-tetrofosmin peak.
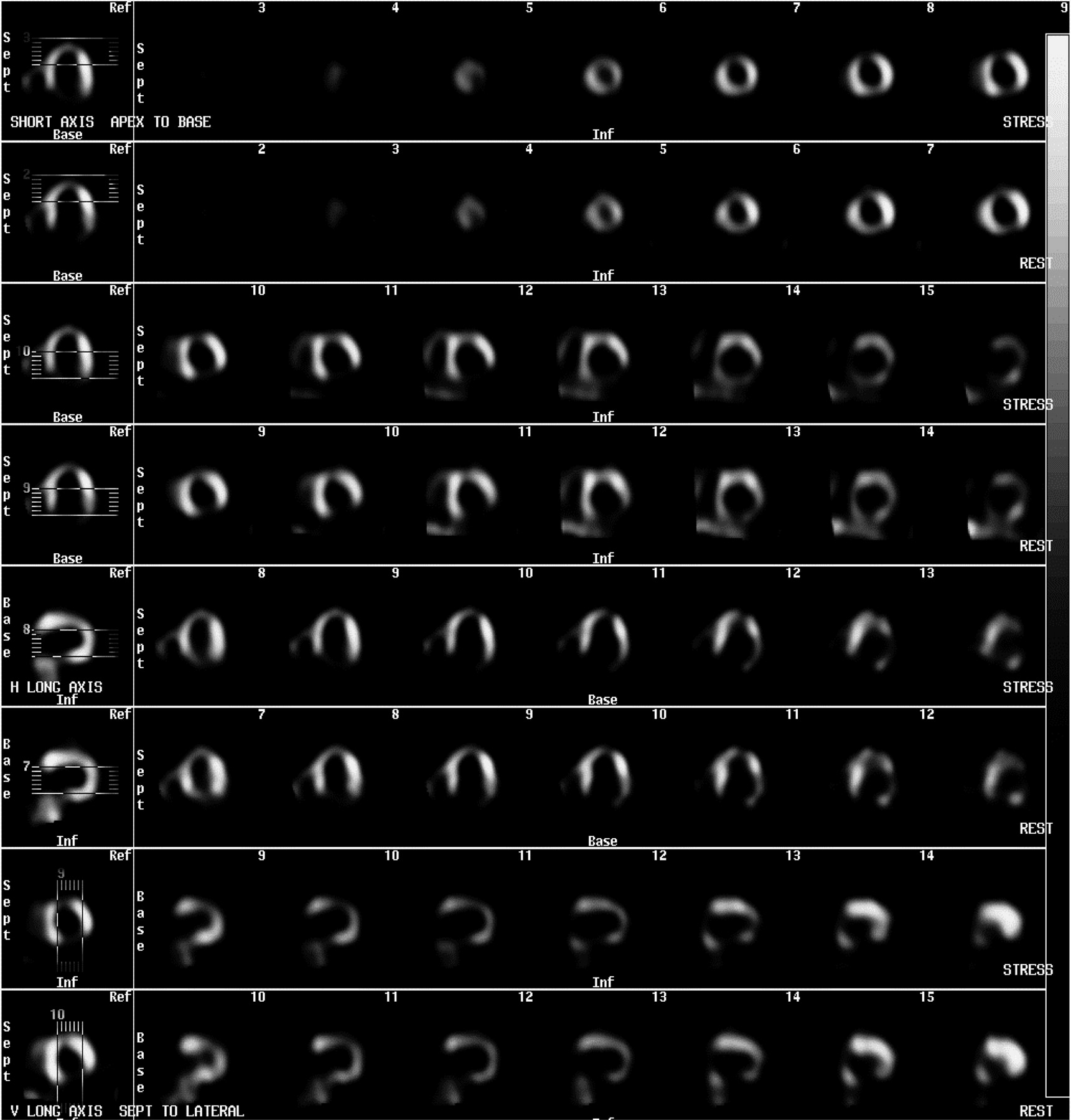
Rest/stress SPECT. Using 99mTc-tetrofosmin with multiple peaks (Fig. 6), 3 nuclear medicine physicians verified the acceptability of these scans.
The silica-cartridge method can be economical. The higher cost of silica cartridges over ITLC strips is offset by savings of time and of solvent costs. Reuse of the silica cartridge after decay of the 99mTc also decreases costs.
CONCLUSION
The technically simple and reproducible silica-cartridge technique satisfies the APhA criteria for an appropriate alternative QC method for 99mTc-tetrofosmin.
Acknowledgments
This research was supported in part by a grant from Amersham Healthcare, Buckinghamshire, U.K.
Footnotes
For correspondence or reprints contact: Richard Hammes, RPh, MS, BCNP, FAPhA, UW Hospital and Clinics, Nuclear Medicine E1/382C, Madison, WI 53706.
E-mail: rj.hammes{at}hosp.wisc.edu





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}