


Abstract
The purpose of this article is to give a basic understanding of imaging setup, postprocessing procedures, and anatomy for brain SPECT. After reading the article, the nuclear medicine professional should be able to describe the normal anatomy of the brain; the localization of radiopharmaceutical complexes within the brain; good techniques for image acquisition; and the concepts of filtered backprojection, smoothing filters, and attenuation correction in reconstruction.
Brain SPECT has become an important diagnostic and research tool in nuclear medicine. The ultimate value of this procedure depends on good technique in acquisition setup and proper data reconstruction. A review of these methods and practices will help the reader better understand how to optimize brain SPECT acquisition, image reconstruction, and image processing.
STRUCTURES AND FUNCTIONS
Basic knowledge of the structures and functions of the brain is important to the technologist performing SPECT. Having an understanding of basic anatomy enhances the collection of imaging data and improves the quality of images. The brain has 4 principal parts: the brain stem, the diencephalon, the cerebrum, and the cerebellum. The brain stem consists of the medulla oblongata, the pons, and the midbrain. The diencephalon consists of the thalamus and the hypothalamus. The cerebrum, or cerebral cortex, is divided into right and left hemispheres. The cerebellum occupies the posterior cranial fossa behind the brain stem.
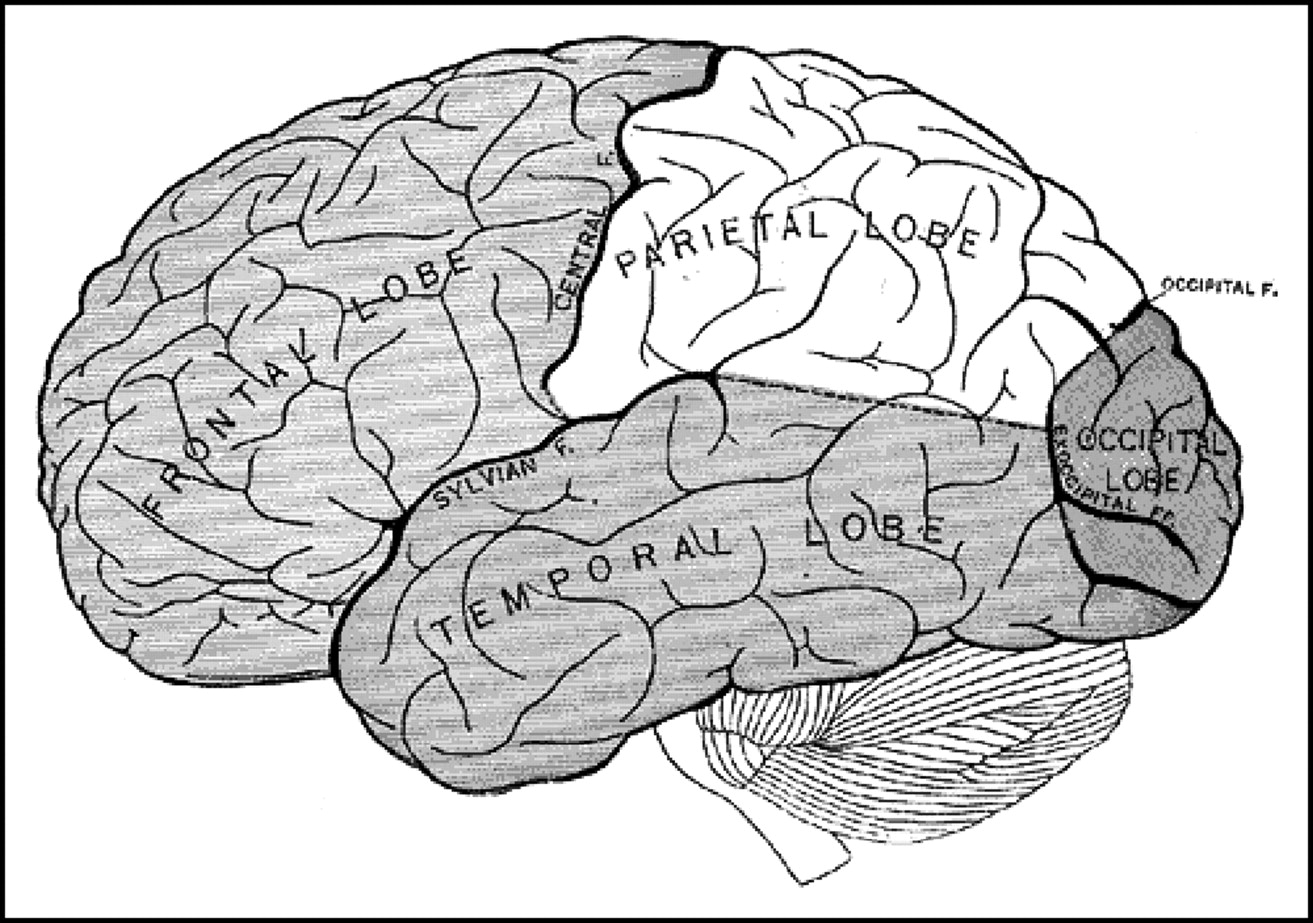
In perfusion imaging, the cerebrum, the cerebellum, and subcortical structures such as the thalamus and basal ganglia are visualized. The cerebrum is composed of gray matter 2–4 mm thick and is also referred to as the cerebral cortex. Gray matter contains dense collections of neuronal cell bodies, whereas white matter (underlying the cortex) is composed primarily of neuronal axons that project between regions of the cortex and subcortical structures. The white matter derives its name from its appearance on gross anatomic inspection; white fatty myelin sheaths coat the long neuronal axons similarly to the insulation on a wire. The cerebral cortex is divided into sensory, motor, and association areas. The longitudinal fissure separates the cerebrum into right and left halves, or hemispheres, which are further subdivided into the frontal, parietal, temporal, and occipital lobes (Fig. 1). The frontal lobe, the most anterior portion of the brain, is responsible for reasoning, emotion, judgment, thinking, learning, and memory. The posterior portion of the frontal lobe also controls the voluntary or skeletal muscles. The central sulcus separates the frontal lobe from the parietal lobe, which is located in the posterosuperior portion of the cerebral cortex. The anterior portion of the parietal lobe controls the sensory functions of the brain. In conjunction with the sensory function of the parietal lobe, it interprets the sense of touch. The understanding of speech and the formulation of words are also controlled by this part of the brain. Inferior to the parietal and frontal lobes is the temporal lobe, which is responsible for audition, visual memory, some language functions, and some speech functions. The posteroinferior portion of the cerebral cortex contains the occipital lobe, which is responsible for vision, visual recognition, and conscious perception of vision.
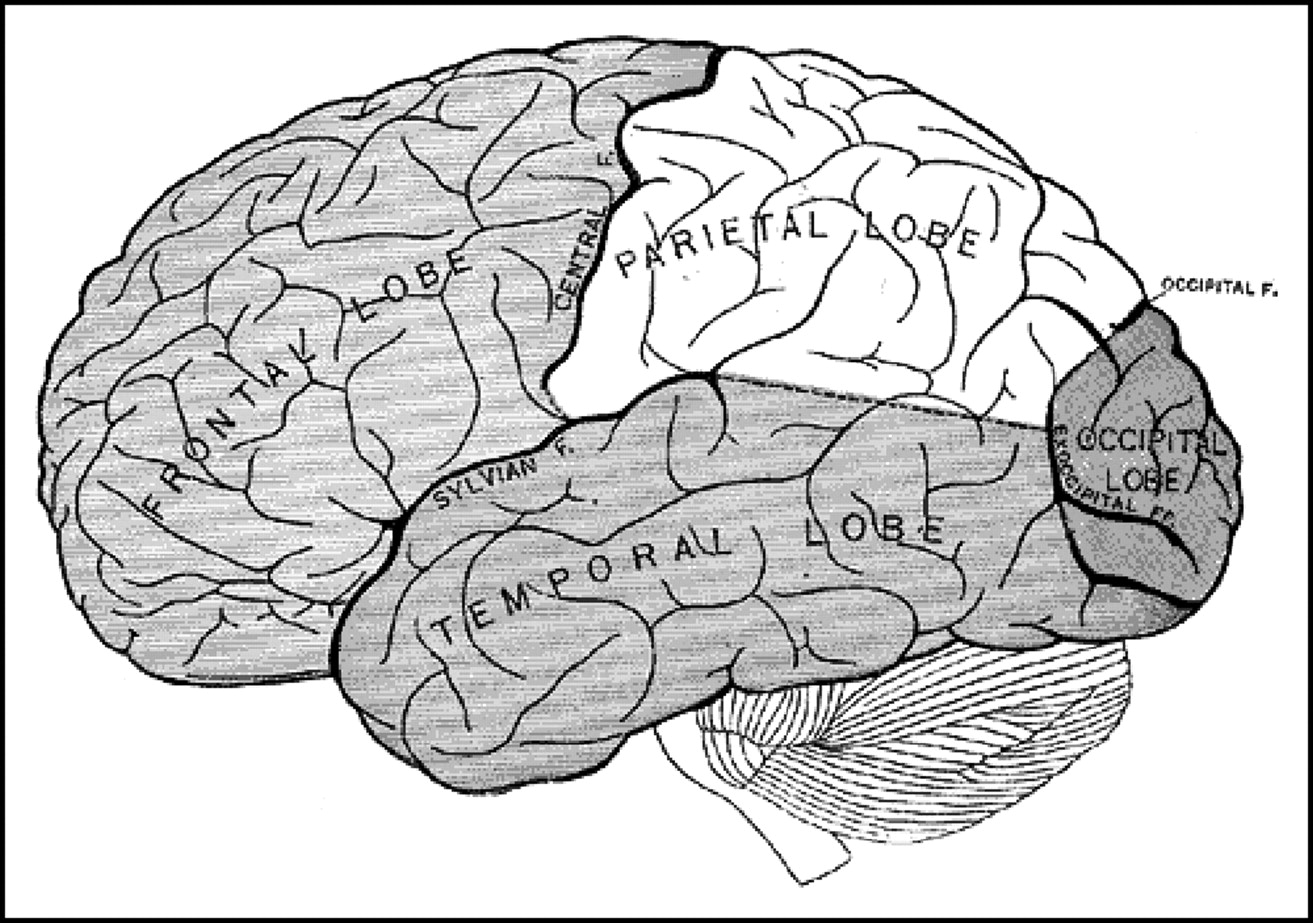
Functional regions of human cerebrum.
Deep within each cerebral hemisphere is the thalamus. These paired masses consist primarily of gray matter and are the principal relay station for sensory impulses from the peripheral nervous system and for neural signals from the central nervous system to the periphery.
The basal ganglia are connected by many fibers to the cerebral cortex, thalamus, and hypothalamus. The basal ganglia consist of paired masses of gray matter in each cerebral hemisphere. The corpus striatum is the largest portion (of gray matter) in each hemisphere. It consists of the caudate nucleus and the lentiform nucleus. The lentiform nucleus is further subdivided into a lateral portion called the putamen and a medial portion called the globus pallidus. The caudate nucleus and the putamen control the coordination of gross movements of skeletal muscles, and the globus pallidus regulates muscle tone required for specific body movements.
The cerebellum is the second largest portion of the brain and is located below the occipital lobes of the cerebrum. The cerebellum controls the coordination of movements required for fine and gross motor tasks and maintenance of posture and balance (1).
RADIOPHARMACEUTICAL CHARACTERISTICS
Typically, brain SPECT uses perfusion agents to assess blood flow patterns in the brain. Agents for this type of imaging are optimized to provide the most favorable characteristics for diagnostic applications. The ideal agent or radiopharmaceutical must cross the intact blood-brain barrier, the protective barrier that permits only certain substances to pass from the blood to the brain. The radiopharmaceutical has to be lipophilic to cross the blood-brain barrier in adequate amounts to provide high-quality brain scans. Optimal brain perfusion agents localize in the brain tissue, with only limited washout and redistribution. The lipophilic compound transported across cell membranes into the cell (neurons and glia, or support cells) is metabolized into a lipophobic compound, hence becoming effectively trapped. Finally, clearance of the radiopharmaceutical from the vascular pool enhances the target (brain)-to-nontarget (scalp and blood pool) ratio, improving image contrast (2). Two commonly used brain SPECT agents that provide these characteristics are 99mTc-hexamethyl propyleneamine oxime (HMPAO) and 99mTc-bicisate ethyl cysteinate dimer (ECD). These agents are rapidly taken up within the brain and allow for imaging of perfusion to the cerebral cortex and related structures during the brief period (90–120 s) when uptake occurs.
RADIOPHARMACEUTICAL LOCALIZATION
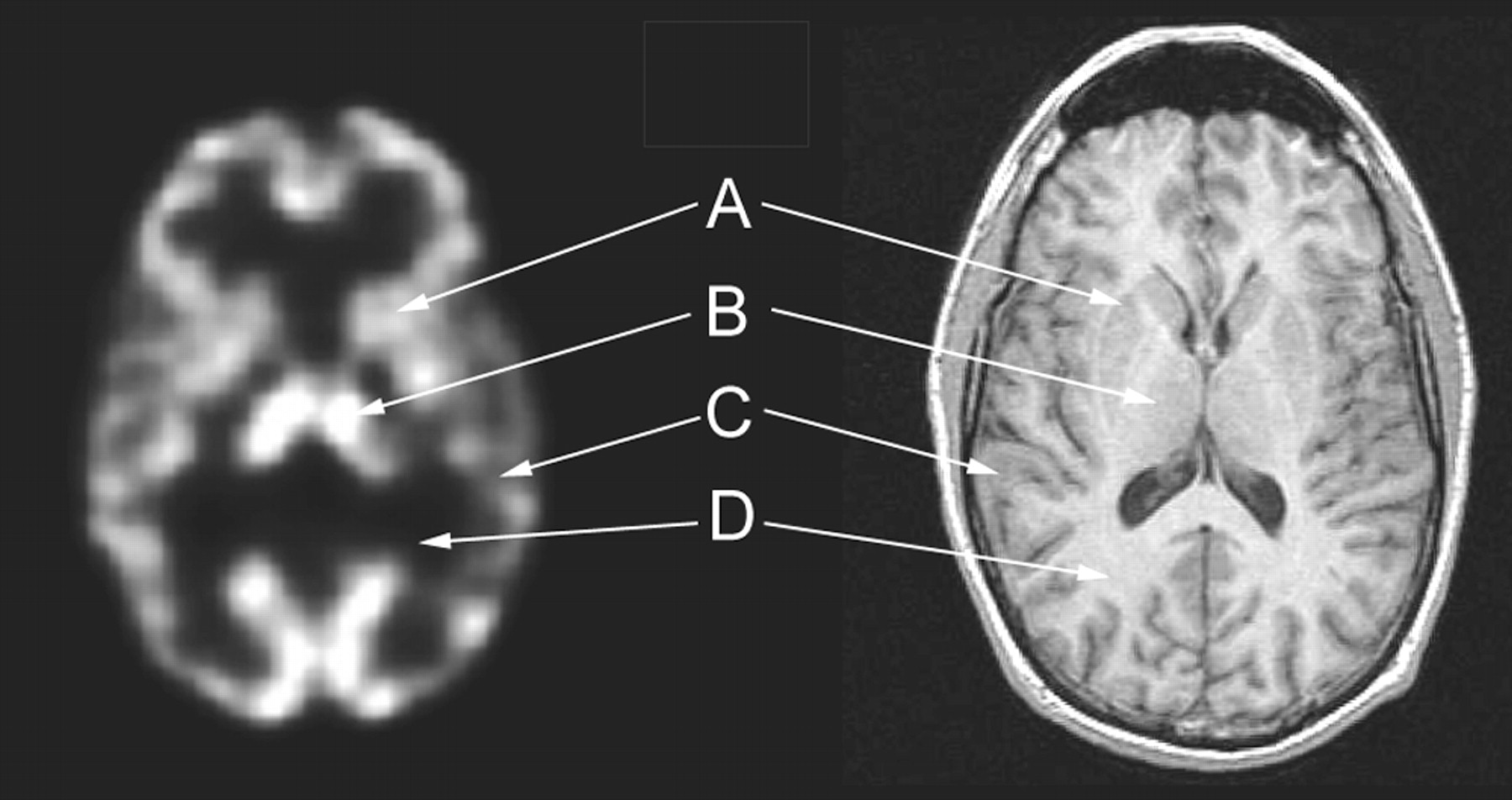
Typically, the normal distribution of a blood perfusion radiopharmaceutical in the brain is symmetric uptake in both hemispheres (Fig. 2). Compared with white matter, gray matter is well visualized because of a higher rate of blood flow. The gray matter-to-white matter flow ratio is approximately 4:1. This general pattern of radiopharmaceutical distribution can be affected by factors such as the visual, auditory, and somatosensory stimuli that the patient experiences during radiopharmaceutical administration. To eliminate differences, clearly defined clinical practices should be used to control environmental variables.
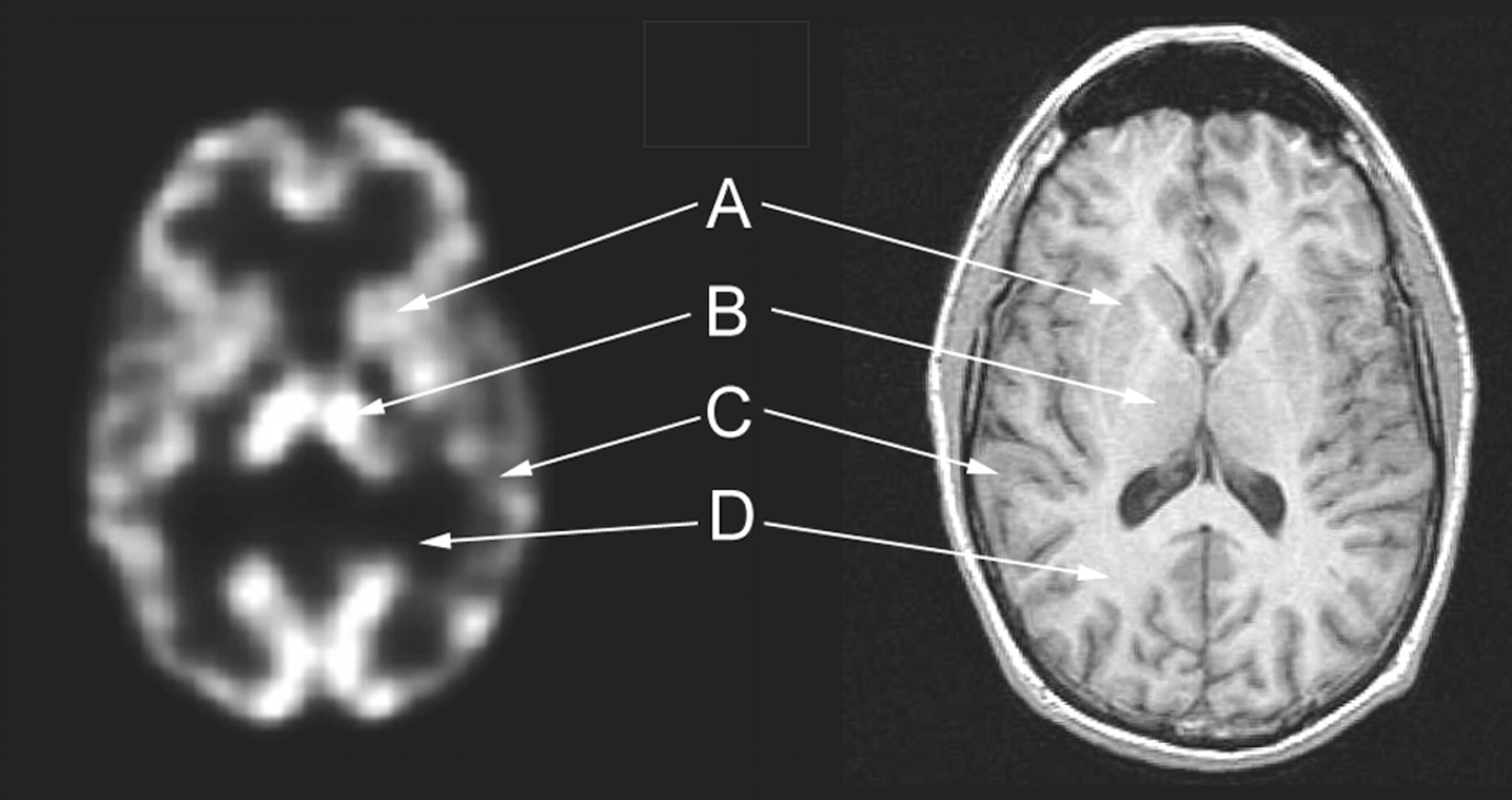
Brain scan and MR image of normal cerebral blood flow: striatum (A), thalamus (B), gray matter (C), and white matter (D).
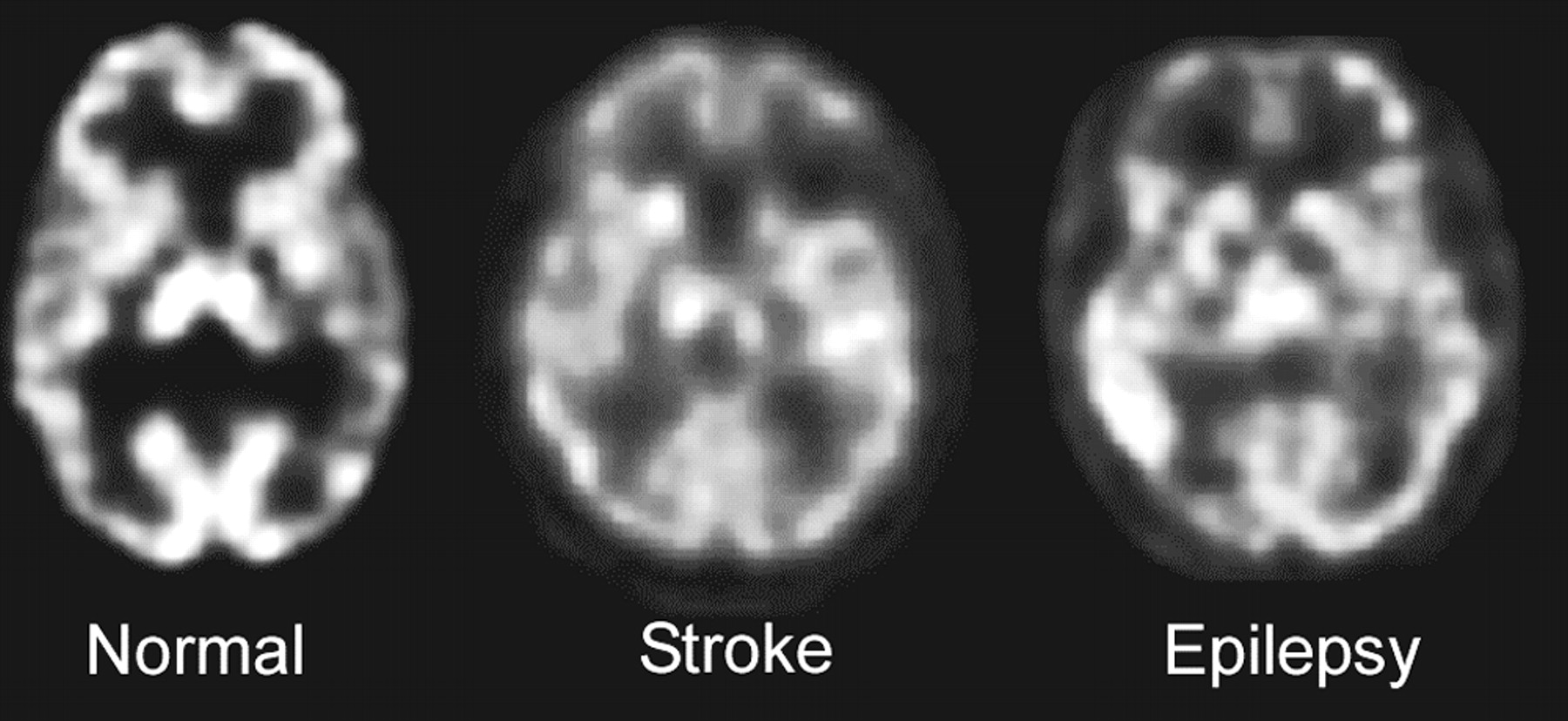
Abnormal brain scan findings include inhomogeneous distributions of the radiopharmaceutical within the brain (Fig. 3). These inhomogeneous patterns can be seen as a complete absence of the radiopharmaceutical, as in cases of infarction. There can also be areas of reduced perfusion, which may indicate ischemia, or areas of increased perfusion, which may indicate the origin of epileptic seizure foci. It is important to remember that these alterations in blood flow are nonspecific (3).

Comparison of SPECT brain scans showing normal findings (homogeneous distribution throughout cerebral cortex and good visualization of internal structures), stroke (findings typical of infarction), and epileptogenic focus (increase of radiopharmaceutical in temporal lobe).
The localization patterns of brain SPECT agents under normal and abnormal conditions are similar. The perfusion agent ECD produces a gray matter-to-white matter ratio slightly higher than that of HMPAO. In addition, ECD clears more quickly from the blood pool, with less scalp activity (soft-tissue uptake) present after 15–20 min.
IMAGE ACQUISITION
A primary source of poor image quality in SPECT is inadequate quality control. Significant image artifacts can occur during acquisition if either detector nonuniformity or center-of-rotation errors are present. As recommended by the manufacturer, quality control procedures should be carefully performed and analyzed before the camera is used to acquire SPECT images. Patient movement is another source of poor image quality, especially in brain imaging. A technologist can use several strategies to minimize patient movement. When patients arrive, time should be taken to explain the procedure and alleviate their concerns. Good communication between the technologist and the patient will help minimize the need to repeat the study. The comfort of the patient is the next concern of the technologist. Ensuring that the patient is positioned comfortably will reduce movement. The use of some type of immobilizing device is also recommended to help in maintaining head position and decreasing movement.
Proper positioning is also important for optimizing image quality. When a patient is improperly positioned, the results can be misinterpreted. An ideal approach is to position the patient’s head in the center of the field of view. The canthomeatal line, the line that extends from ear to eye, should be perpendicular to the face of the detector and the head held straight (not tilted left or right). All programs allow the flexibility of reorienting the data after acquisition to additionally correct for misaligned patients; however, manipulating the data can introduce errors, including image blurring. A typical SPECT acquisition is best acquired over a 360° rotation, with sufficient time per stop to obtain ample counts for good statistical data.
RECONSTRUCTION
A SPECT brain scan that has been acquired successfully must next be processed or reconstructed for visual or quantitative evaluation. The 2 commonly available reconstruction methods are filtered backprojection and iterative reconstruction. The more common of these, filtered backprojection, is relatively fast. The iterative method, in contrast, requires more processing steps but can potentially reduce some reconstruction artifacts.
To understand what occurs when data are reconstructed by filtered backprojection, one must understand the concept of simple backprojection. In simple backprojection, an assumption is made that the acquired photons occurred equally along a path from their point of detection backward. This assumption, although mathematically correct, creates artifacts. These artifacts, or false data, have to be eliminated by applying a ramp filter, hence the process of ramp-filtered backprojection. Image reconstruction is performed after the data are converted from a spatial domain into a frequency domain (Fourier transformation). The ramp filter then multiplies the low-frequency amplitudes of the data by small factors and the high-frequency amplitudes by large factors to represent the data. The image file created by this method is the closest representation of the acquired data but contains significant noise. The noise component of the data is a function of the statistical uncertainty in photon detection (due to the random nature of radiation emission and detection hardware).
APPLICATION OF SMOOTHING FILTERS
The next reconstruction step is the application of a smoothing filter to the data. Smoothing filters remove high-frequency noise from the data created by the ramp filter. By enhancing the low frequencies, filters, in effect, boost the image signal relative to the high-frequency noise and thus improve image quality. However, if the goal of the reconstruction and filtration is to provide quantitative information about a physiologic process of the brain (e.g., the density of a receptor target), this filtration strategy can corrupt the quantitative validity of the data by making the relationship nonlinear between the reconstructed counts and the amount of radioactivity distributed within that region of brain.
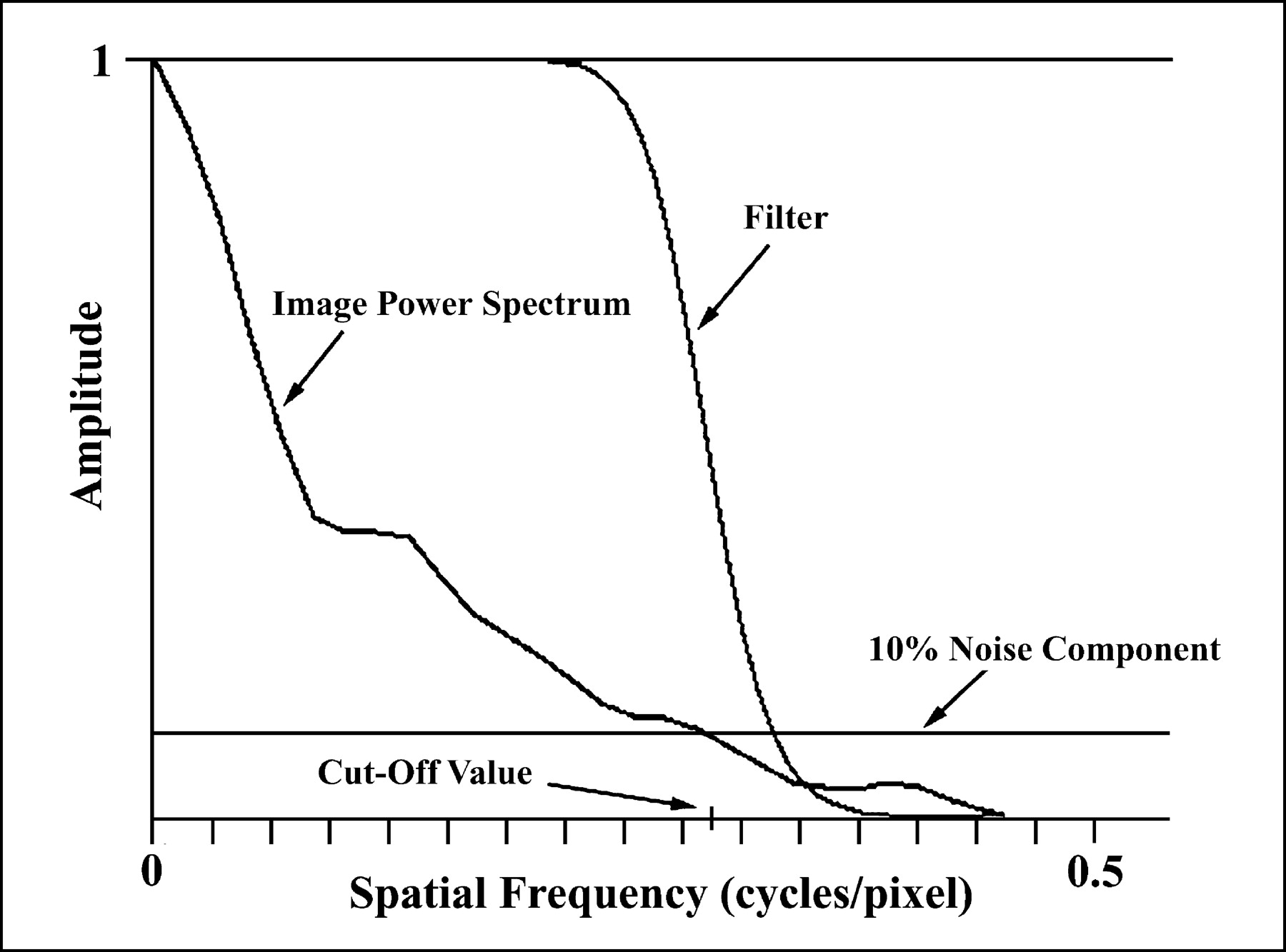
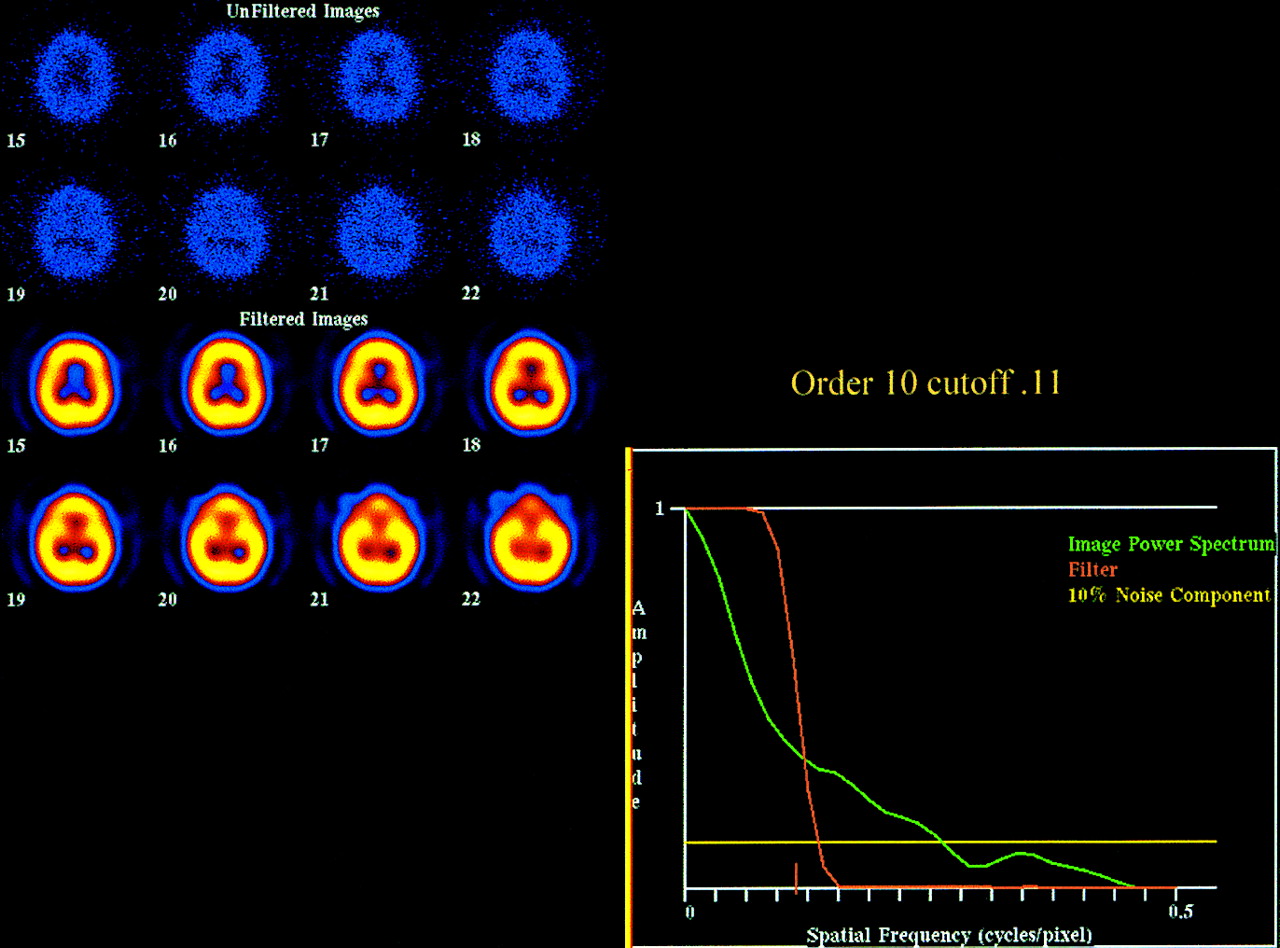
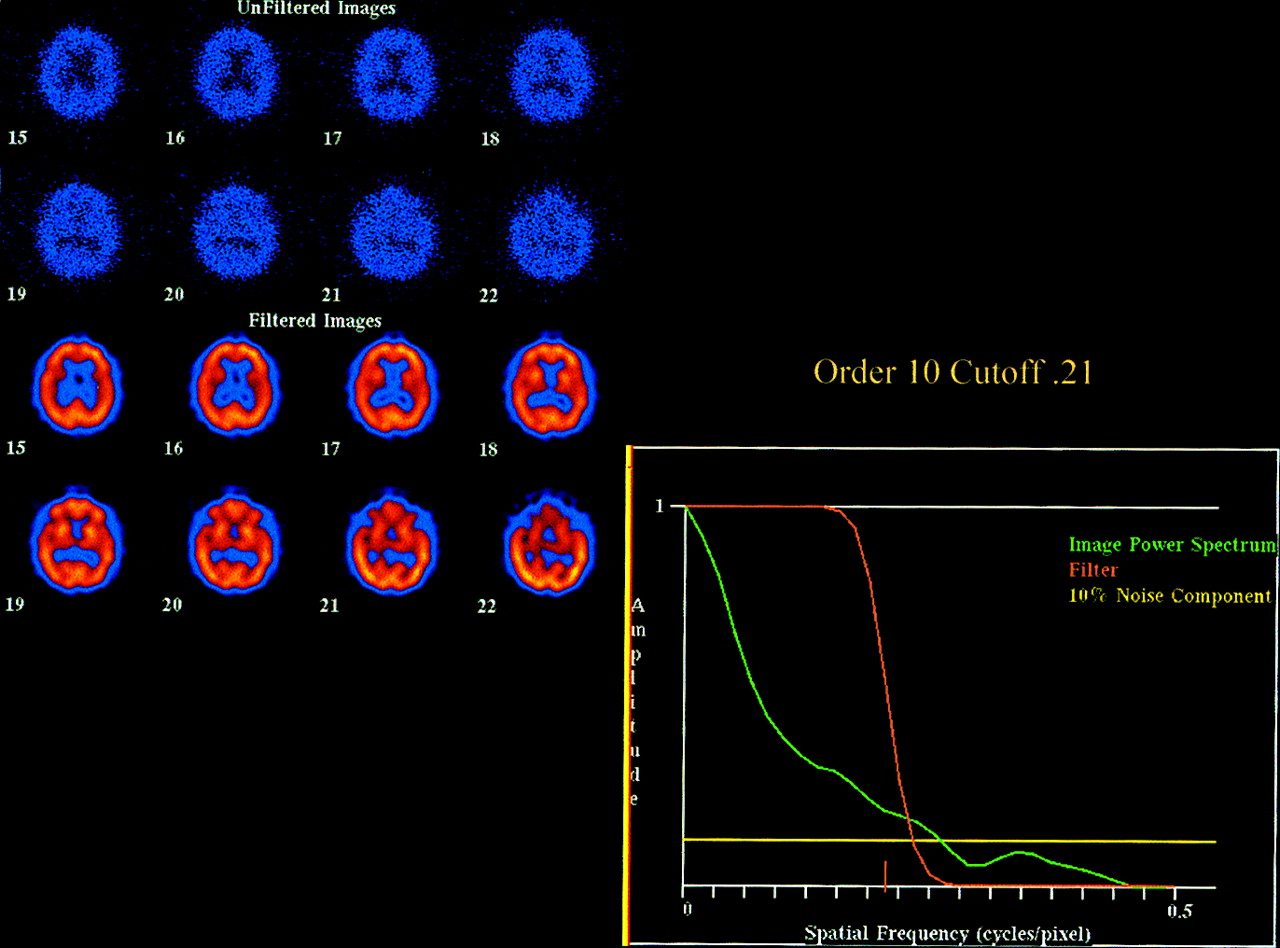
Filters are applied by manipulating the cutoff values for the data in the frequency space (Fig. 4). The cutoff value determines the amount of noise included or excluded from the data. When the cutoff value is increased, more noise is included, whereas the opposite is true for decreases in the cutoff value. These changes dramatically affect the visual presentation of the data. For example, when the cutoff is too high, the images are too grainy, and when the cutoff is too low, the images are too smooth (Fig. 5). For perfusion imaging, an overly smooth filter could eliminate the finding of a focal regional blood flow abnormality. A reasonable value to choose for the cutoff is the intersection of the image power spectrum with the noise component (Fig. 4). This cutoff choice prevents excess smoothness or graininess without distorting the data (Fig. 6). The cutoff value is important to the data because it helps determine the overall quality of the reconstructed image.
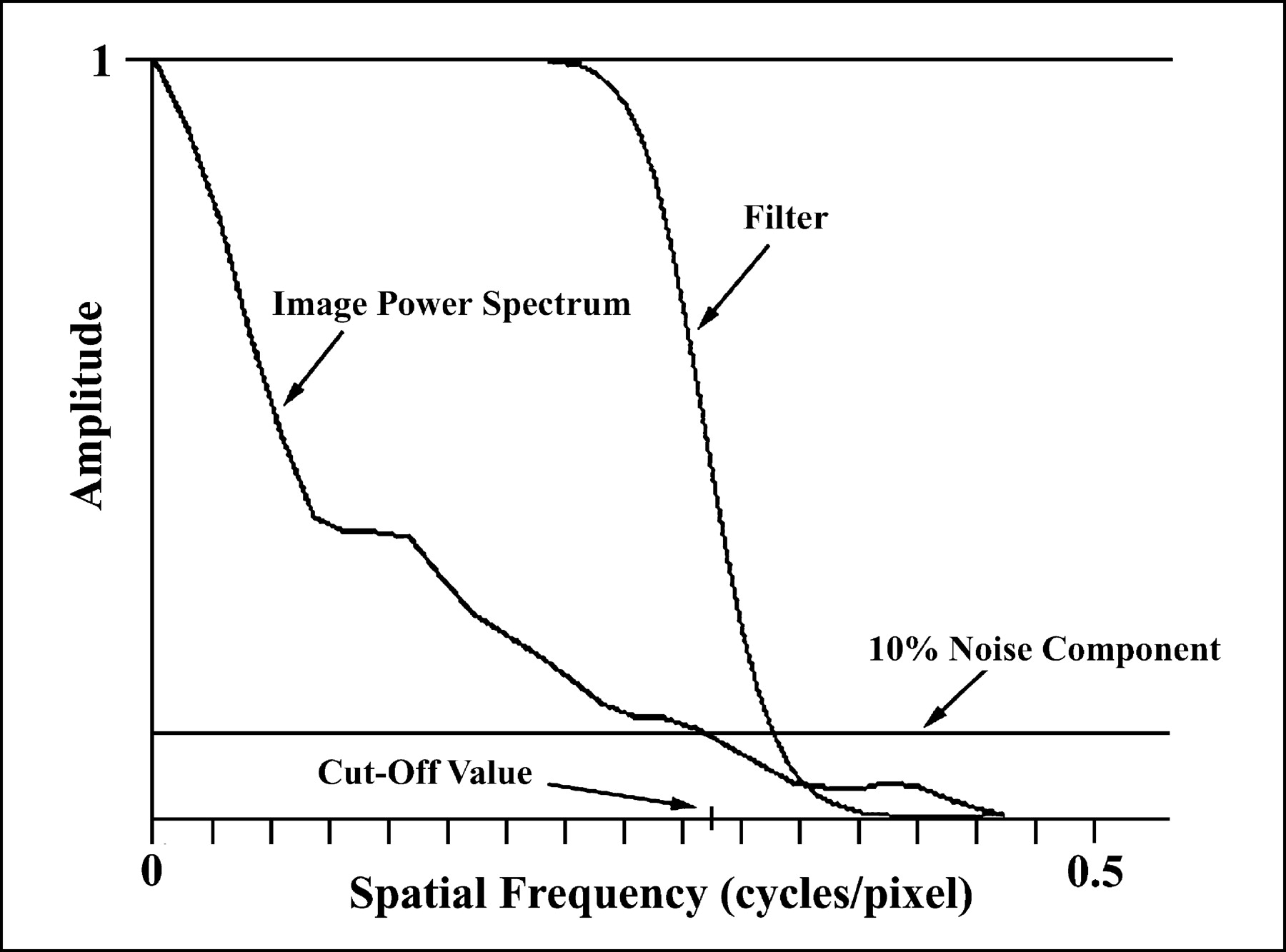
Example of frequency spectrum for brain perfusion dataset. Cutoff value can be set where image power spectrum intersects with noise component.
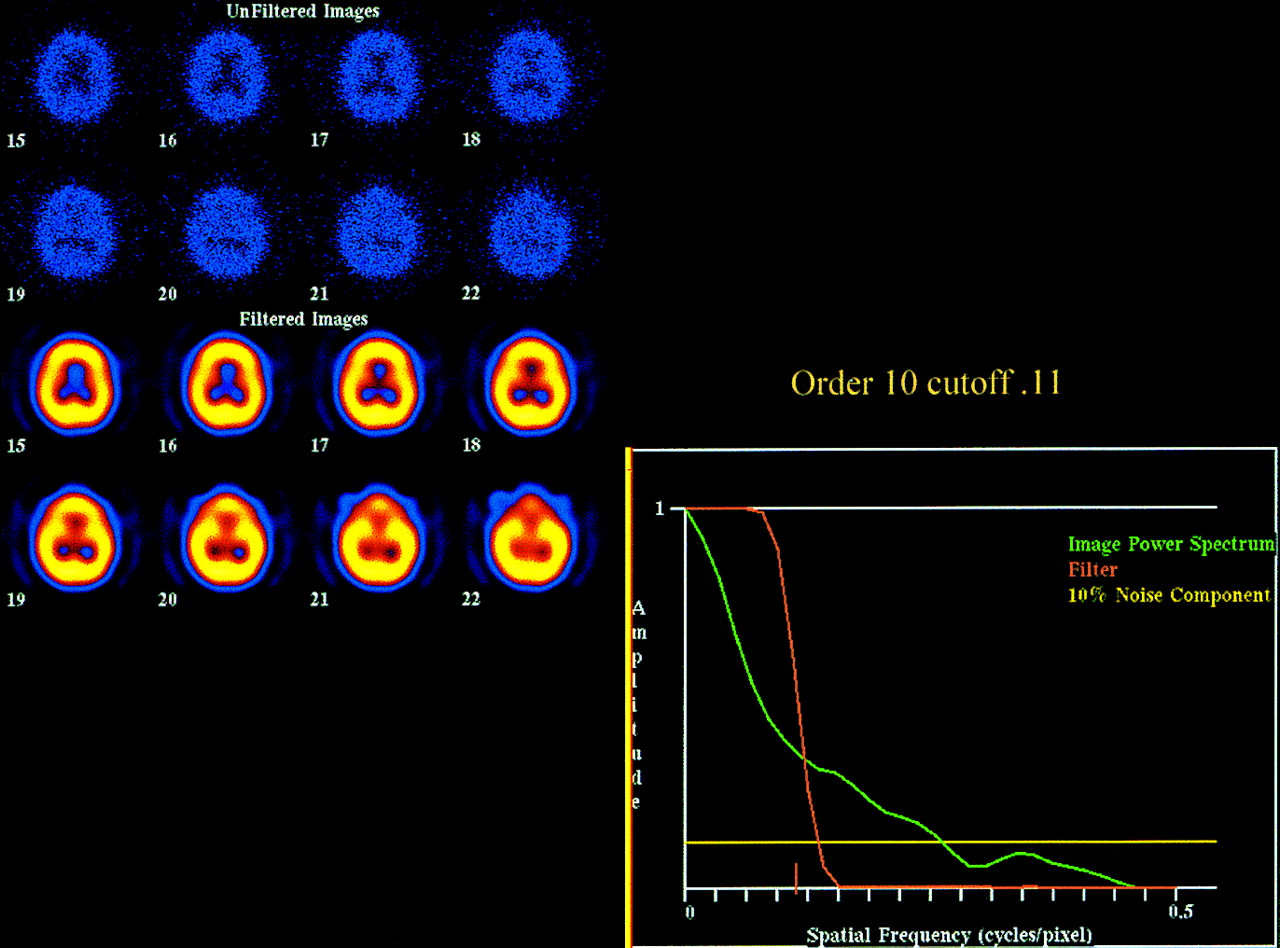
Example of data filtered using cutoff value of 0.11. Images become too smooth, and spatial resolution is lost.

Example of data filtered using cutoff value of 0.21. Images show good structural information within data and are not overfiltered.
Another variable of a smoothing filter is the order of a Butterworth filter. The order sets the rate of transition from signal (data) to noise and determines the slope of the filter. An increase in the order will produce a steeper slope and, therefore, a faster change from signal to noise. A decrease in the order slows the change and produces a more gradual slope. Unlike changes in the cutoff value, changes in the order do not dramatically alter the visual presentation of the data (4). Although there are many smoothing filters available from different vendors (e.g., Hanning, Hamming, and Shepp-Logan), our physicians have found that the described reconstruction and filtering parameters provide the most acceptable images for clinical reading.
ATTENUATION CORRECTION
The last reconstruction step for SPECT data is attenuation correction. Attenuation correction increases the counts at the center of an image proportionately to the distance from the edge of the image and can be either uniform or nonuniform. Uniform correction (the Chang 0 method) uses an ellipse (constant μ, in cm−1) to compensate for absorbed γ-rays. The attenuating properties of the object being imaged are assumed to be uniform, and the counts in the image simply are boosted as a function of distance from the edge of the ellipse and the assumed density of the object. The density of the brain is similar to that of water, and the thickness of the skull is uniform around the brain. The assumption of uniform attenuation conditions is therefore adequate for most brain applications. Nonuniform attenuation correction, in contrast, is well suited to whole-body imaging, in which tissue and bone densities vary greatly.
CONCLUSION
Brain SPECT is a powerful clinical and research tool in the management and diagnosis of neurologic and psychiatric diseases. With careful acquisition and processing to achieve optimal images, the highest-quality data can be obtained and used in various applications to further our knowledge of the functional and structural areas of the brain.
Acknowledgments
The authors thank Eileen O. Smith, Jeremy Virgil, Gary Wisniewski, and Brenda Jacobson for information provided and their support in the preparation of this article.
Footnotes
For correspondence or reprints contact: Gina N. Morano, CNMT, RT(N), Molecular NeuroImaging, LLC, 60 Temple St., Suite 8A, New Haven, CT 06510.
E-mail: gmorano@mnimaging.com
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/education/ce_online.html) THROUGH DECEMBER 2004.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}