


Abstract
Objective:In the preparation of radiopharmaceuticals, staff receive considerable radiation exposure to the hands during withdrawal of activity from the elution vial, from a combination of the syringe and elution vial activities. In an attempt to reduce the radiation burden to the hands, a simple technique was developed that utilizes a modified lead pot lid and a syringe bearing a long needle with a sterile needle guide.
Methods:An elution vial in a lead pot with an attached syringe was secured at an angle of 45°, simulating the action of withdrawing 99mTc-pertechnetate from the elution vial. The 99mTc activity ratio of vial to syringe was 20:1. A gamma- camera detector without collimator was positioned at the syringe plunger and count profiles were obtained after 10 min of data acquisition. The experiment was repeated using the same set-up with (a) the modified lid on the lead pot and (b) a cold syringe to determine the contribution of the radioactive syringe to the count profile. Each experiment was repeated at the vertical position, simulating the normal action of redispensing 99mTc activity into the elution vial.
Results:The modified lid reduced exposure from the elution vial, with a count reduction of >98% for both orientations. The contributions of vial radioactivity to the total count profile were 76% and 84% for vertical and 45° orientations, respectively. The contributions of syringe activity were 24% and 16% for vertical and 45° orientations, respectively.
Conclusion:A reduction in the photon flux to the hands of up to 84% (with an associated reduction in hand dose) can be achieved by withdrawing activity through a modified lid on the lead pot housing the elution vial, without significantly altering normal work practices.
Nuclear medicine staff members typically receive a radiation burden to the whole body and hands resulting from the practices of eluting the 99mTc/99Mo generator and preparing radiopharmaceutical doses, as well as from administration of patient doses and patient contact. In our department, the normal work procedures of radiopharmacy staff require eluting the generator for a source of 99mTc-pertechnetate, reconstitution of cold kits with this isotope, and finally withdrawing multiple radiopharmaceutical patient doses from the kit vial. With these tasks, there is considerable radiation exposure to the hands when withdrawing 99mTc-pertechnetate activity from the elution vial. The hands receive a much higher radiation dose than other parts of the body (1,2). Attempts to reduce the hand dose have prompted the evaluation of radiation-attenuating surgical gloves (3,4), automated dose dispensing systems (5,6), and a prototype shielding syringe plunger (7). Recent studies have shown that the use of lead syringe shields during the dispensing of radiopharmaceutical patient doses results in a lower dose to the fingers, particularly the index finger (8), where the dose distribution is different (9). The radiation exposure to the hands, however, results not only from the syringe withdrawing 99mTc-pertechnetate activity but from the remaining, higher activity in the elution vial contained in the lead pot. The aim of this study was to find a practical way of reducing the hand radiation dose without significantly altering the routine functions needed for radiopharmaceuticals preparation. A new technique has been developed and involves withdrawing activity through a small hole in the lid of the lead pot that houses the elution vial. We have investigated the effect of using this modified lid on radiation exposure at the hand position.
MATERIALS AND METHODS
Experimental Set-Up
The new technique uses a modified lead lid to seal the pot containing the elution vial. This lid has a centrally located small hole (2.5-mm diameter) that permits a long syringe needle (21 gauge) to access the elution vial with the lid on. A sterile blunt plastic cannula (Becton Dickinson & Co; Singapore) is used as the needle guide and neatly fits in the small hole of the modified lid.
To evaluate the effectiveness of this lid, the following experiments were performed. Sodium 99mTc-pertechnetate solution (0.8 MBq) obtained from a dry bed 99Mo/99mTc generator (Gentech 120 GBq; Australian Radioisotopes, Sydney, New South Wales, Australia) was diluted in saline (0.9% to 10 mL) and then added to an evacuated elution vial (Gentech; 30 mL). After equilibrating the pressure with a breather needle, a small volume (0.56 mL) was then withdrawn from the elution vial and placed inside another syringe (5 mL) with an air space (1 mL). The ratio of elution vial activity to syringe activity was 20:1. This was to simulate a normal working day scenario in which 10 GBq 99mTc-pertechnetate is withdrawn from the elution vial containing 180 GBq 99mTc-pertechnetate to accommodate 8 patient doses of 800 MBq each over a 3-h period. The elution vial was secured inside the lead pot, and the radioactive syringe with needle was inserted through the modified lid via the cannula and into the vial.
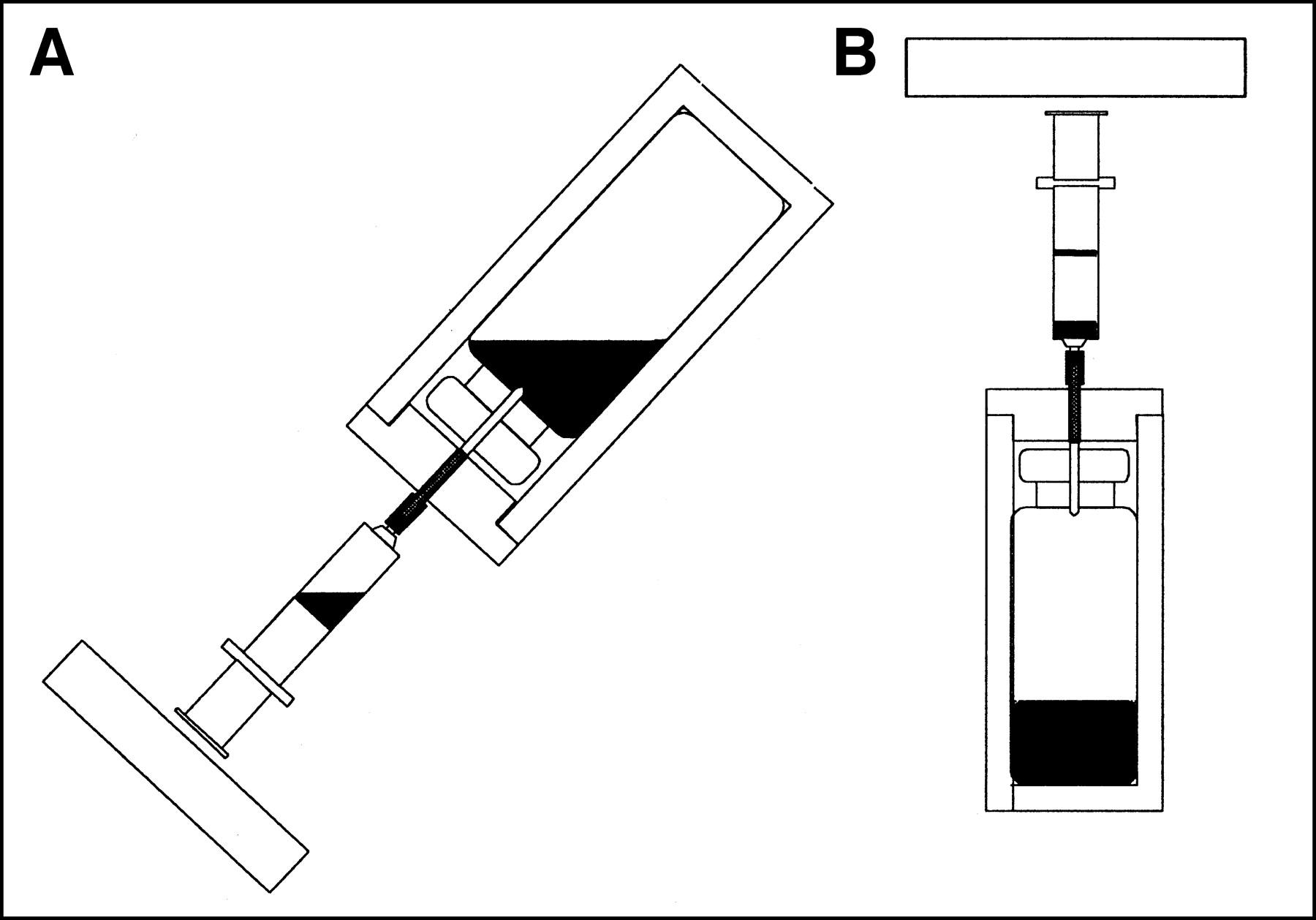
Two different orientations that are used when preparing radiopharmaceuticals were investigated: a 45° orientation representing the normal action of withdrawing radioactivity from the elution vial, and a vertical position representing the usual action for redispensing activity back into the elution vial (Fig. 1). At each orientation, 4 experiments were performed: with the syringe containing radioactivity or “hot” syringe (lid on, lid off) and with the syringe containing saline or “cold” syringe (lid on, lid off). The apparatus was fixed into position using a retort stand and clamps at both orientations.

Schematic diagram of apparatus used in new elution technique for 45° (A) and vertical (B) orientations. Rectangle at proximal end of syringe represents gamma-camera detector.
Quantitative Measurements
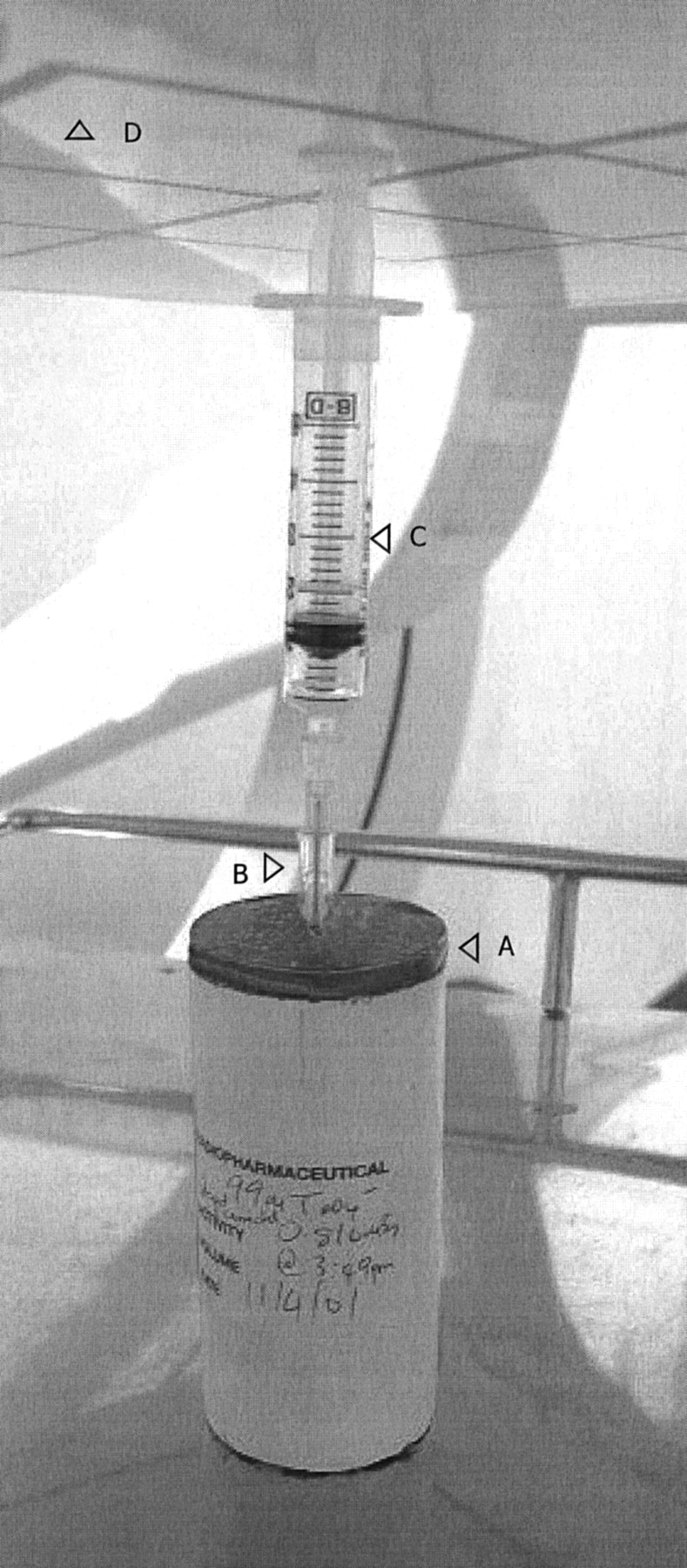
A scintillation camera (Millennium MPR; General Electric Medical Systems, Milwaukee, WI) detector without collimator was positioned as close as possible to the syringe plunger for the vertical orientation (Fig. 2). The shortest distance from the camera detector crystal to the center of the radioactive solution was 21.5 cm. Static acquisitions were obtained with a 99mTc window (140 keV ± 20%) for 10 min to generate images and count profiles (an approximation of radiation dose). Vertical count profiles were obtained from the images with a slice thickness of 4 pixels and expressed as counts/min/MBq versus distance (cm) along the camera face perpendicular to the axis of vial and syringe. The same procedure was followed with the 45° orientation experiments. The distance along the camera face was calibrated against image pixels using 2 99mTc sources separated by a known length. Low 99mTc activities (<1 MBq) were used for all experiments to avoid dead-time errors. The percentage dose reduction in using the modified lid was obtained from the count profile data at the peak values using the formula: 100 × (1 − counts lid on/counts lid off). To assess reproducibility, experiments were repeated for the vertical orientation (n = 5) and the values for full width at half maximum (FWHM), contribution from syringe activity, and attenuation by syringe are reported as mean ± SD. Reproducibility was determined using the formula: coefficient of variation = 100 × SD/mean.

Layout for vertical orientation experiments with scintillation camera. (A) Modified lid. (B) Needle guide. (C) “Hot” syringe. (D) Gamma-camera detector (without collimator).
RESULTS
The modified lid reduced exposure from the elution vial, with a count reduction of >98% in the high-dose region (cold syringe, lid on) at both 45° and vertical orientations (Fig. 3). The count profile resulting from activity in the elution vial was altered by the collimating effect of the lead pot and had a FWHM value of 16.3 cm and 9.8 ± 0.3 cm for the 45° and vertical orientations, respectively. Counts fell to background levels (<5% of peak value) at distances (perpendicular to the axis and from the center line) >16.3 or 15.5 cm for the 45° orientation, which had an asymmetic distribution, and 8.2 cm for the vertical orientation. There was a significant drop for 45° (23%) and vertical (35% ± 2%) orientations at the center line of the count profile as a result of attenuation by the syringe and, specifically, the metal needle.
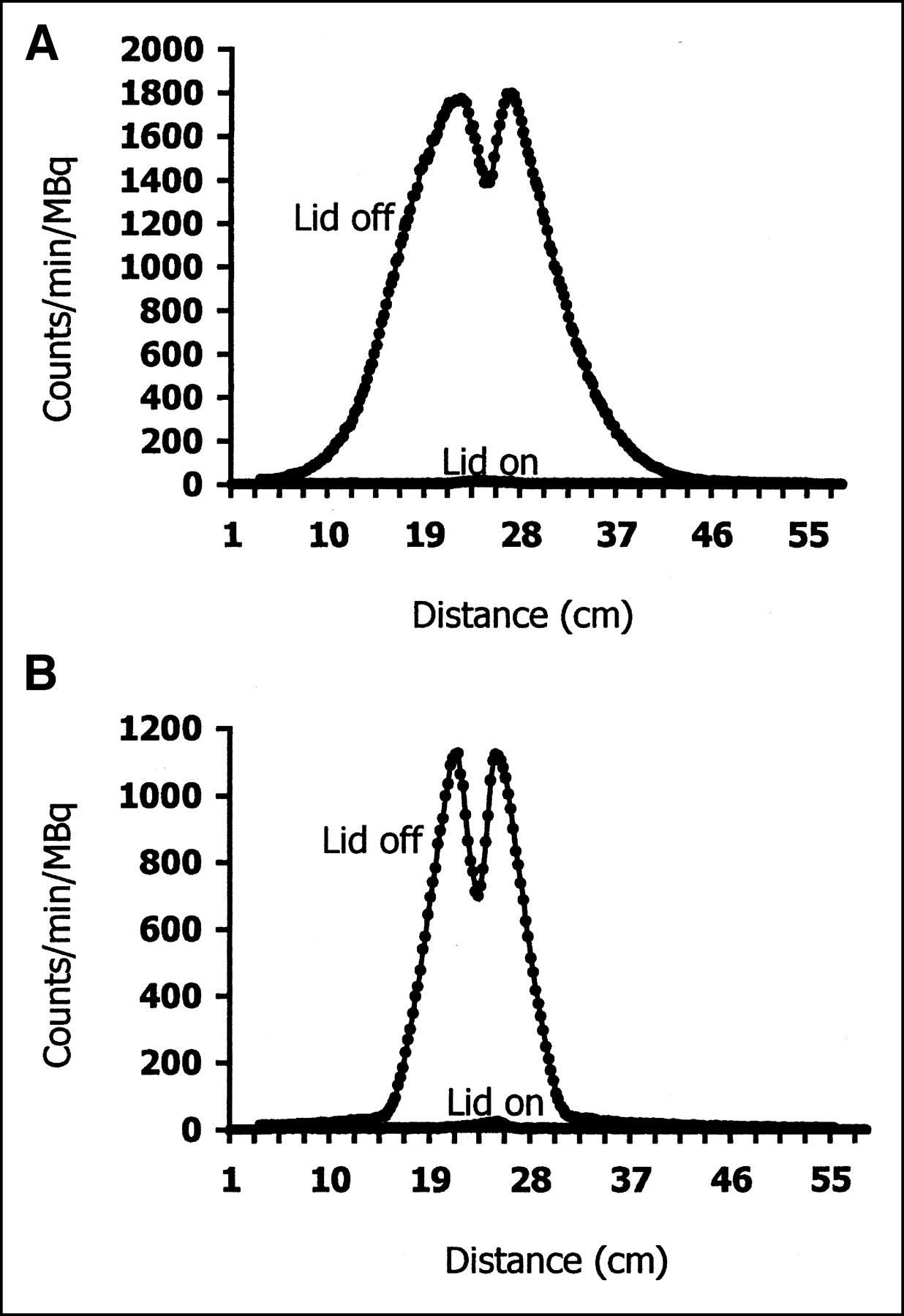
Count profiles for “cold” syringe in 45° (A) and vertical (B) orientations, illustrating reduction in radiation exposure from elution vial when modified lid is used.
In Figure 4, the lid-on profiles for both orientations represents counts from the syringe only. In the 45° position the elution vial contributes 84% to the total count profile (hot syringe, lid off). The remaining contribution from the syringe activity is 16%. At the vertical orientation, the elution vial contributes 76% and the hot syringe 24% ± 1% to the total count profile (Fig. 4). Repeat experiments performed in the vertical orientation were highly reproducible, with coefficients of variation of 3.4%, 3.4%, and 5.3% for FWHM, contribution from syringe activity, and attenuation by syringe, respectively.
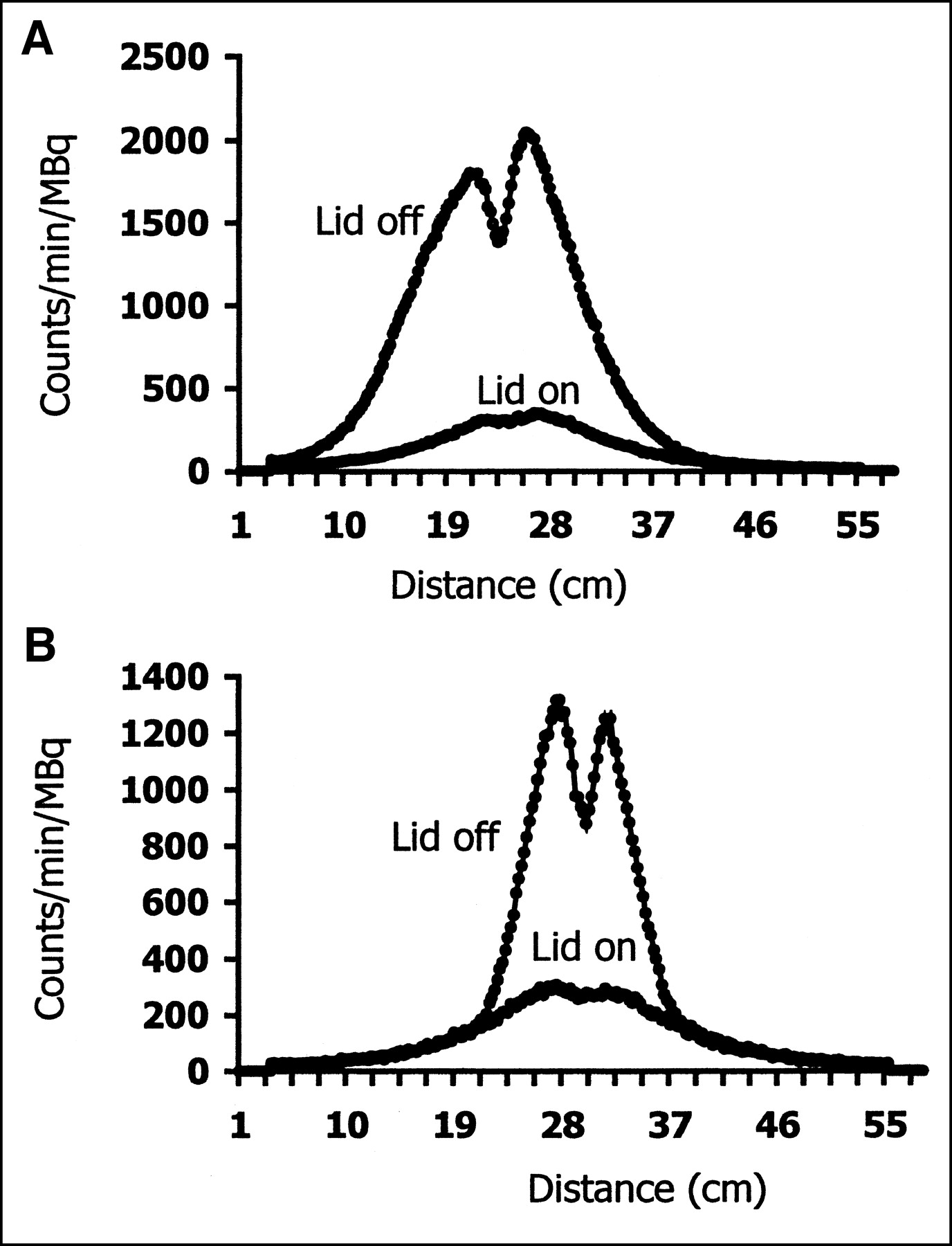
Count profiles for “hot” syringe in 45° (A) and vertical (B) orientations, illustrating contribution of syringe activity (lid on) to total count profile.
DISCUSSION
Previous workers have studied the radiation burden to the hands during the preparation of radiopharmaceutical doses, offering practical solutions such as syringe shields (9), radiation-attenuating gloves (3), and syringe plungers (7). However, this report considers the contribution to the total radiation exposure made by high levels of radioactivity in the elution vial, a scenario that is common in reconstituting cold kits and preparing patient doses. The daily workload in a department dictates how much activity is necessary to reconstitute each cold kit planned for use on that day. In this department, for example, 10 GBq would be required to reconstitute a methylene diphosphonic (MDP) acid kit in the morning to yield 8 patient bone doses over the next 3-h period. This activity is removed from the elution vial, where the amount of 99mTc-pertechnetate is usually considerably larger than that withdrawn by syringe. With 120-GBq generator-delivered precalibration (equivalent to 180 GBq), the eluted 99mTc-pertechnetate activity on the first few days can exceed the syringe activity by up to a factor of 20 (the worst-case scenario), the ratio decreasing with every new elution over the following days. Our results indicate that 99mTc-pertechnetate in the elution vial accounts for a large portion (up to 84%) of the photon flux to the hands. When the modified lid was used, it effectively eliminated this contribution. The success of this technique is dependent on the small size of the hole in the lid, where most of the radioactivity is shielded from the elution vial and low radiation emission is “collimated” in a thin beam toward the hand. The radiation dose was not directly measured in these experiments. However, the count profiles are a reasonable approximation to dose.
A significant part of the hand/arm will be exposed to vial activity, particularly when withdrawing activity at 45°. This is the orientation that most appropriately represents the posture of the hands of radiopharmacy personnel when 99mTc-pertechnetate activity is withdrawn from the elution vial. In this position, the count profile was considerably broader than at the vertical orientation (FWHM 16.3 cm vs. 9.8 cm) because the vial activity was nearer to the opening, thus reducing the collimating effect of the pot. The count profile was also skewed because the 99mTc-pertechnetate volume was asymmetric or tilted. In practice, the elution vial is not fixed inside the lead pot, allowing staff to slide it out from the pot during withdrawal of radioactivity, which would result in an even broader profile and consequently a larger area of the hands and arms irradiated. With the modified lid left on the pot during the withdrawal procedure, this radiation burden is removed.
Use of the plastic cannula in the technique overcomes any compromise in sterility when withdrawing radioactivity through the narrow opening. This cannula ideally fits through the lid hole and acts as a guide for the syringe needle to pierce the bung. Conveniently, the needle and needle guide dimensions are such that the needle protrudes only a few millimeters inside the vial, thereby alleviating any problems in extracting “blindly” (i.e., at a 45° angle) from vials containing low volumes. The routine practice of wiping the elution vial bung with a sterilizing agent, such as 70% alcohol, is unaffected. When withdrawal of 99mTc-pertechnetate from the elution vial is complete, the modified lid is either left on, replaced with a standard lid, or another lid can simply be placed on top of the modified lid. Although the needle dimensions and fixed construction of an insulin syringe would preclude its use with the modified lid, all other common syringes (1, 2, 5 mL, etc.) containing a provision for needle attachment can be used. The needle should be 38 mm long, a standard length for this common hospital item and an optimal size to reach just beyond the elution vial bung. Apart from the MDP reconstituted kit situation, the modified lid would also be an advantage when single-patient doses of 99mTc-pertechnetate are withdrawn directly from the elution vial (such as for gated blood pool, Meckels, lacrimal, shunts, thyroid studies, etc.), and contribution to radiation exposure from the syringe activity is very small. It would also have an advantage when single 99mTc doses are withdrawn from reconstituted cold kits of much higher activity. The modified lid has been successfully used in our radiopharmacy for routine preparation of radiopharmaceutical patient doses.
CONCLUSION
Depending on the procedure undertaken, a large component of the radiation exposure to the hands is from activity in the unshielded vial. By withdrawing activity through a modified lid on the lead pot housing the elution vial, a reduction in the photon flux to the fingers/hands of up to 84% can be achieved. The use of this simple and effective technique does not significantly alter normal work practices.
Footnotes
For correspondence or reprints contact: Chris Tsopelas, PhD, Nuclear Medicine Department, Royal Adelaide Hospital, North Terrace, Adelaide 5000, South Australia, Australia.
E-mail: ctsopela{at}mail.rah.sa.gov.au





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.