


Abstract
The purpose of this study was to evaluate the effectiveness of activation versus baseline SPECT in detecting the regional cerebral blood flow (rCBF) changes in Alzheimer’s disease (AD) patients after milameline (CI979/RU35926) treatment.
Methods: Ten patients with AD who took part in a milameline drug trial were examined by 99mTc-hexamethylpropyleneamine oxime SPECT before and after the medication. A split-dose technique was used for the acquisition of baseline and activation images within a single session. Two patients were unable to complete the activation challenges. rCBF changes were assessed using the statistical parametric mapping program. Both increased and decreased contrasts were used to test rCBF changes on activation and baseline images, respectively. rCBF changes caused by activation were also examined before and after milameline treatment.
Results: Decreased rCBFs were observed at the temporal cortex on both sides of the brain and at the left parietal cortex on the activation SPECT images after milameline, whereas no statistically significant rCBF change was found on the baseline SPECT images. Memory stress caused not only increased rCBF in many areas of the brain, including the parietotemporal cortex, but also decreased rCBF at the splenium of the corpus callosum.
Conclusion: Cognitive activation scans are more effective than baseline scans in detecting rCBF changes in AD patients after milameline.
- regional cerebral blood flow
- SPECT
- statistical parametric mapping
- cognitive activation
- Alzheimer’s disease
Assessment of drug effects on patients with Alzheimer’s disease (AD) has been performed using SPECT (1–7) and PET (8–10). The symptoms of AD patients are believed to correlate with the patient’s regional cerebral blood flow (rCBF) or glucose metabolism (11,12), although the marker region using rCBF for the diagnosis of the AD remains questionable (13–15).
SPECT images are acquired, in many cases, before and after any drug administration or therapeutic treatment, and any change in rCBF is assessed in relation to the drug’s effect on the patients (1–7,11,12). Darcourt et al. (6) and Robert et al. (7) suggested that SPECT studies with cognitive stimulation would improve the sensitivity of detecting rCBF changes and would be better than that of baseline SPECT in evaluating the drug’s effect on AD patients. To my knowledge, assessment of the drug or therapeutic effect using activation SPECT images in detecting changes in rCBF in patients with AD has not been reported.
Brain activation studies are used mainly to identify specific anatomic regions and neural networks involved in particular cerebral functions (16–23). Activation studies using SPECT have the advantage of lower cost and wider availability than that of using PET and functional MRI (17). Moreover, using a split-dose technique (16,21–23) in the SPECT activation studies has another advantage in that no extra radiation dosage is required for both baseline and activation scan acquisitions. This is in contrast to that of a conventional single-dose rest scan. By combining the split-dose SPECT scan design with the conventional assessment of the drug or therapeutic effect using SPECT, not only can the rCBF changes in activation and baseline states be assessed separately but also the rCBF changes caused by the activation challenges can be examined before and after the medication.
The aim of this study was to examine the effectiveness of baseline verses activation SPECT scan images in detecting rCBF changes of a group of AD patients who participated in a milameline (CI979/RU35926) drug trial. Milameline is a muscarinic agonist and is a potential drug for the treatment of AD (24,25). Both preclinical and phase I clinical trials showed that milameline was safe (26,27) and possessed a pharmacologic profile of partial muscarinic agonist (28,29). The SPECT images were acquired before and after the patients received milameline using the split-dose technique. The patient images were analyzed using the statistical parametric mapping (SPM) program (30) taking the patients as a group. SPM is now a popular tool for analysis of SPECT images (31–34).
MATERIALS AND METHODS
Ten patients suffering from AD underwent a milameline drug trial followed by injection of 99mTc-hexamethylpropyleneamine oxime (HMPAO). The SPECT images were taken 1–4 wk before and 16–20 wk after milameline treatment.
A Picker Prism 3000XP (Phillips/Picker International, Cleveland, OH) triple-head gamma camera was used for the SPECT image acquisitions. Each patient was imaged supine with his or her head in a secured foam block. The chin and forehead were strapped to minimize movement. The intensity of light within the scan room was minimized. A split-dose scanning procedure, similar to that of Ebmeier et al. (19,21) and Panteno et al. (16), with injection of 370 MBq 99mTc-HMPAO, was used for each image acquisition. The number of projection images was set to 128 with data being acquired for 35 s at each projection. The images were reconstructed using filtered backprojection with a Butterworth filter (cutoff, 0.4; order, 3) and Chang’s attenuation correction.
The baseline SPECT images were acquired while patients were engaging in a simulated cognitive task. Each patient was asked to indicate (by pressing 1 of 2 buttons that were resting on his or her chest) when a word or repeated letters appeared on a computer screen. The screen was located 50 cm from the patient. The activation task involved patients memorizing a list of 10 words from the computer screen. The words were selected from the PALPA (psycholinguistic assessment of language processing in aphasia) instrument. The word list was presented as many times as necessary to achieve retention of 6 of 10 words. After a standard delay of 3 min, the patients began the recall task. This involved choosing between 2 words presented on the computer screen by pressing 1 of 2 buttons similar to that of the baseline task. One of the words was from the 10-item list, presented in random order, and the other word was selected as a semantic or phonemic distracter from PALPA. Both baseline and activation tasks were administered 30 s before the initial radiotracer injection and continued for 3 min after injection, during which time all radiotracer uptake occurred.
SPM was developed by Friston et al. (30) at the Wellcome Department of Cognitive Neurology, University College London (London, U.K.), and is now used worldwide (available at: http://www.fil.ion.ucl.ac.uk/spm; accessed May 11, 2002). Statistical parametric maps are spatially extended statistical processes that were used to characterize regionally specific effects in imaging data. SPM combines the general linear model and the theory of gaussian fields to make statistical inferences about regional effects. To examine images for specific regions of differences in perfusion between 2 groups, the 2 groups were compared using contrasts. The first contrast examined areas of increased perfusion in 1 group, compared with the other group, and the second contrast examined areas of decreased perfusion (30–34).
The SPM99 version of the SPM package was used for the image analysis. Native Picker SPECT images were transferred to an SGI Unix workstation (Silicon Graphics, Inc., Mountain View, CA), and an in-house C program was used to convert the Picker’s native image format into the Analyze format used by the SPM99 program. All images were coregistered with the PET template provided by the SPM99 package using the Automatic Multimodality Image Registration program (35). The images were globally scaled with a grand mean of 50 and smoothed with a 12-mm full width at half maximum kernel using SPM99. The experimental design “multisubjects, different conditions” was used for the statistical analysis. An arbitrary value of 30 voxels was set for the cluster threshold (P < 0.01 for all clusters), and the other parameters were used as set by the SPM99 default. Both increased and decreased rCBF contrasts were used to test the rCBF changes on the activation SPECT images before and after milameline in parallel with that on the baseline SPECT images. Similar tests were also used for the activation-caused rCBF changes before and after milameline.
RESULTS
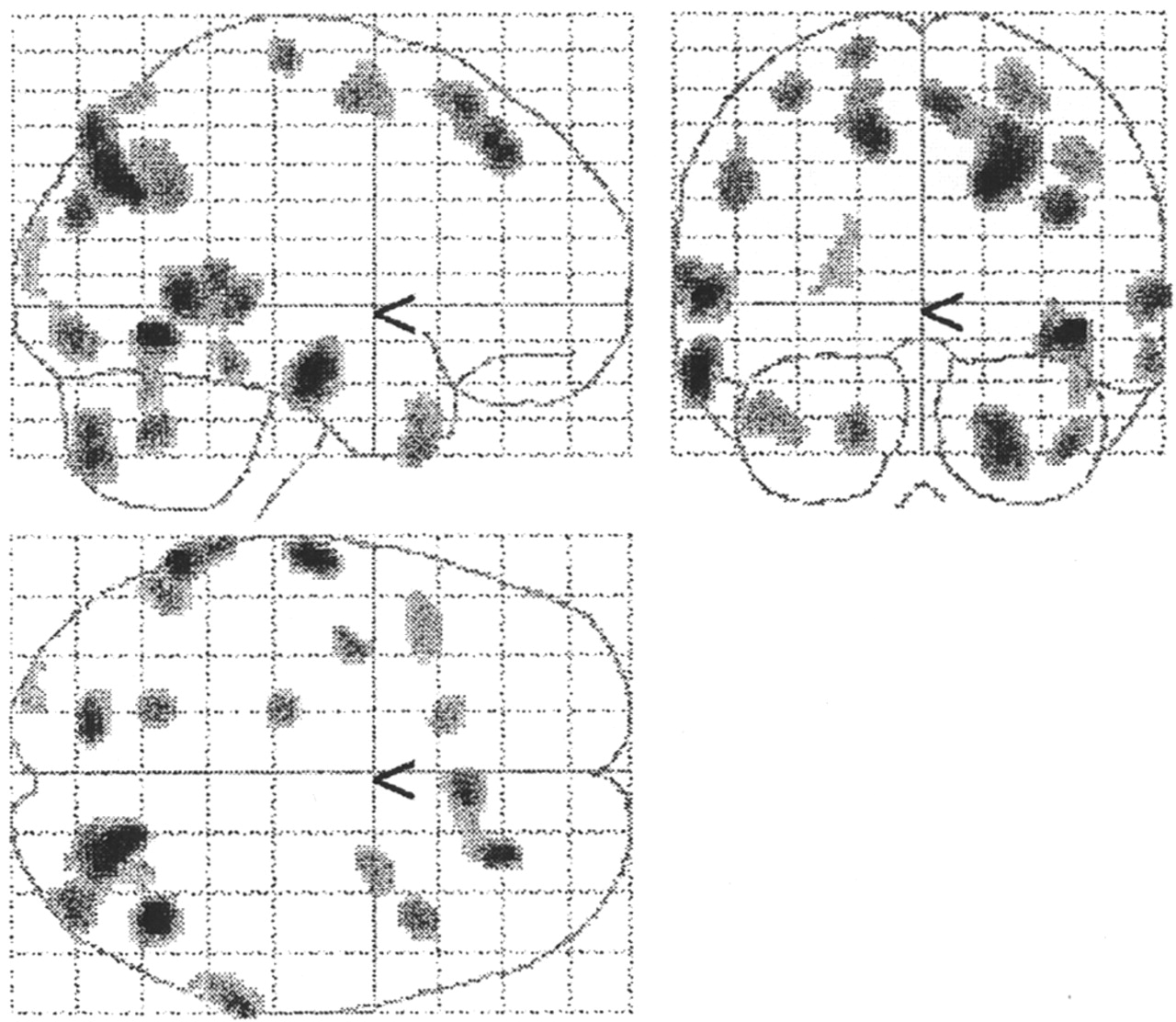
Comparison of the activation images and the baseline scans before milameline treatment (using increased contrast) demonstrated increased rCBFs in many areas of the brain as shown in Figure 1. The Talairach and Tournoux coordinates (Talairach coordinates) (36) of these increased rCBF regions within Figure 1 are listed in Table 1. A similar pattern of increased rCBFs was observed in the activation after milameline (not shown). These results indicate that the memory stress induced an increased cerebral blood flow in many areas of the brain, predominantly in parietotemporal cortex regions.
Talairach Coordinates for Increased rCBFs Caused by Memory Stress Activation Before Milameline Treatment
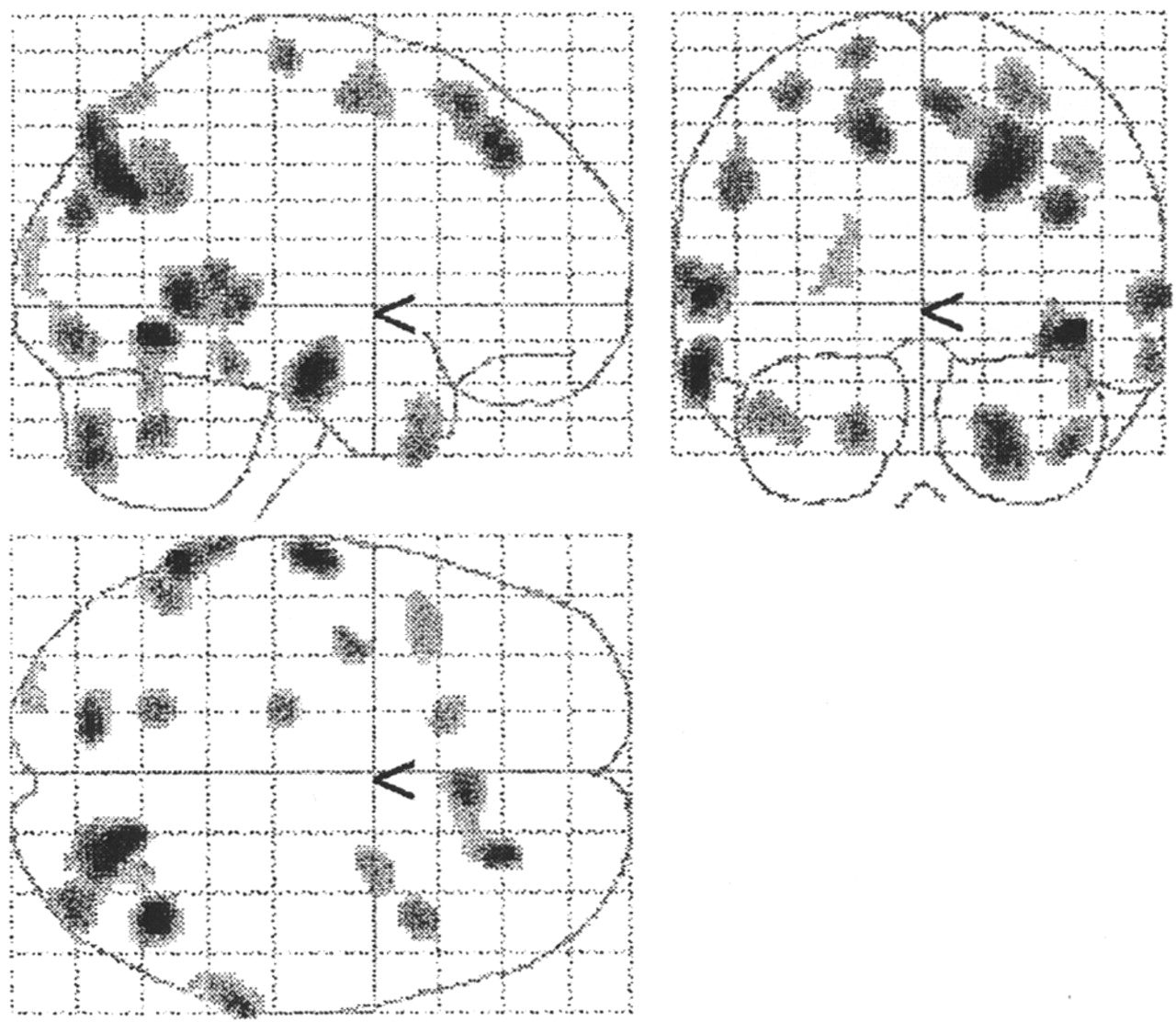
Increased rCBFs caused by cognitive activation before milameline. Talairach coordinates of these activation regions are listed in Table 1. Similar pattern of increased rCBFs was observed in activation after medication (not shown).
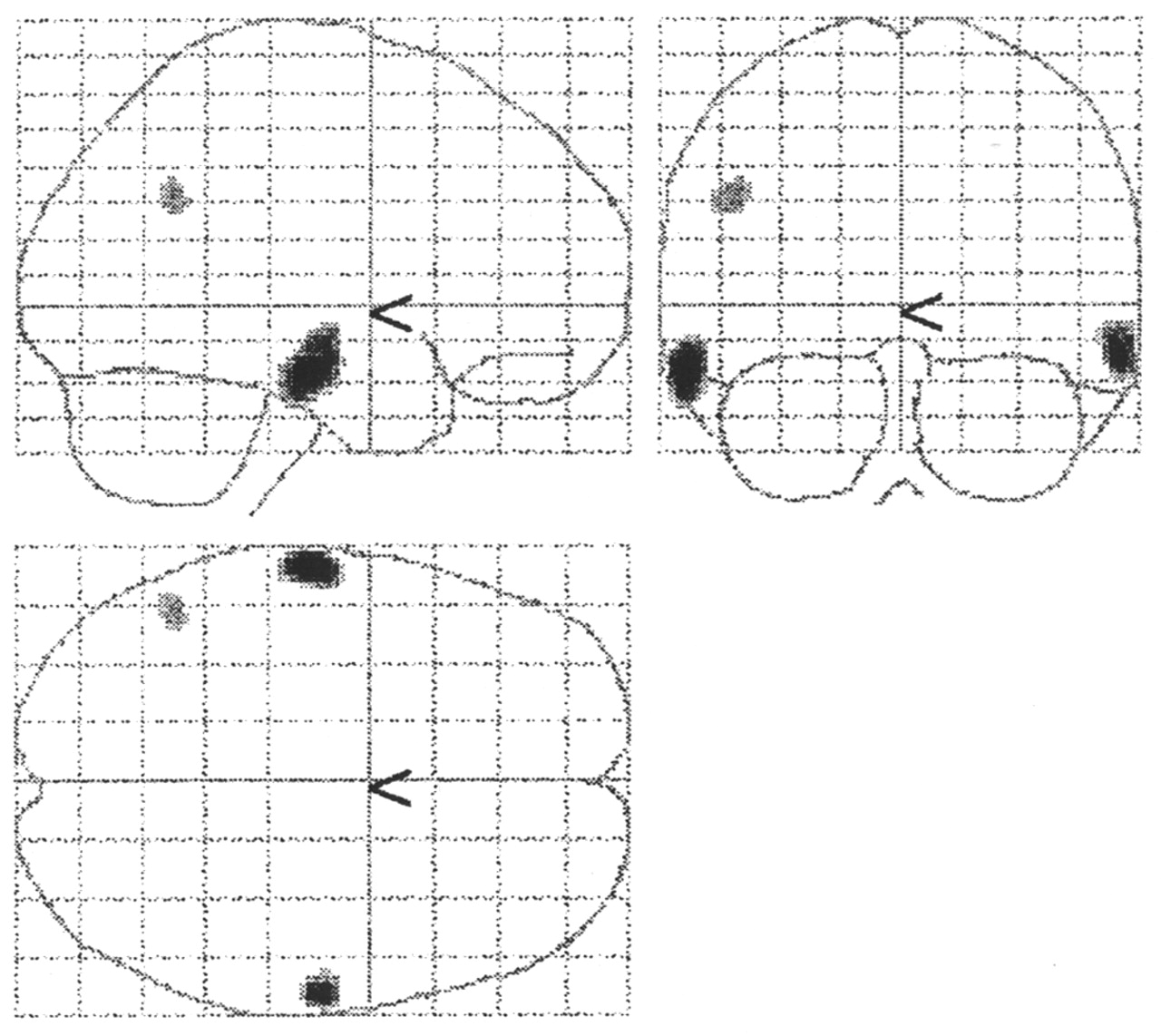
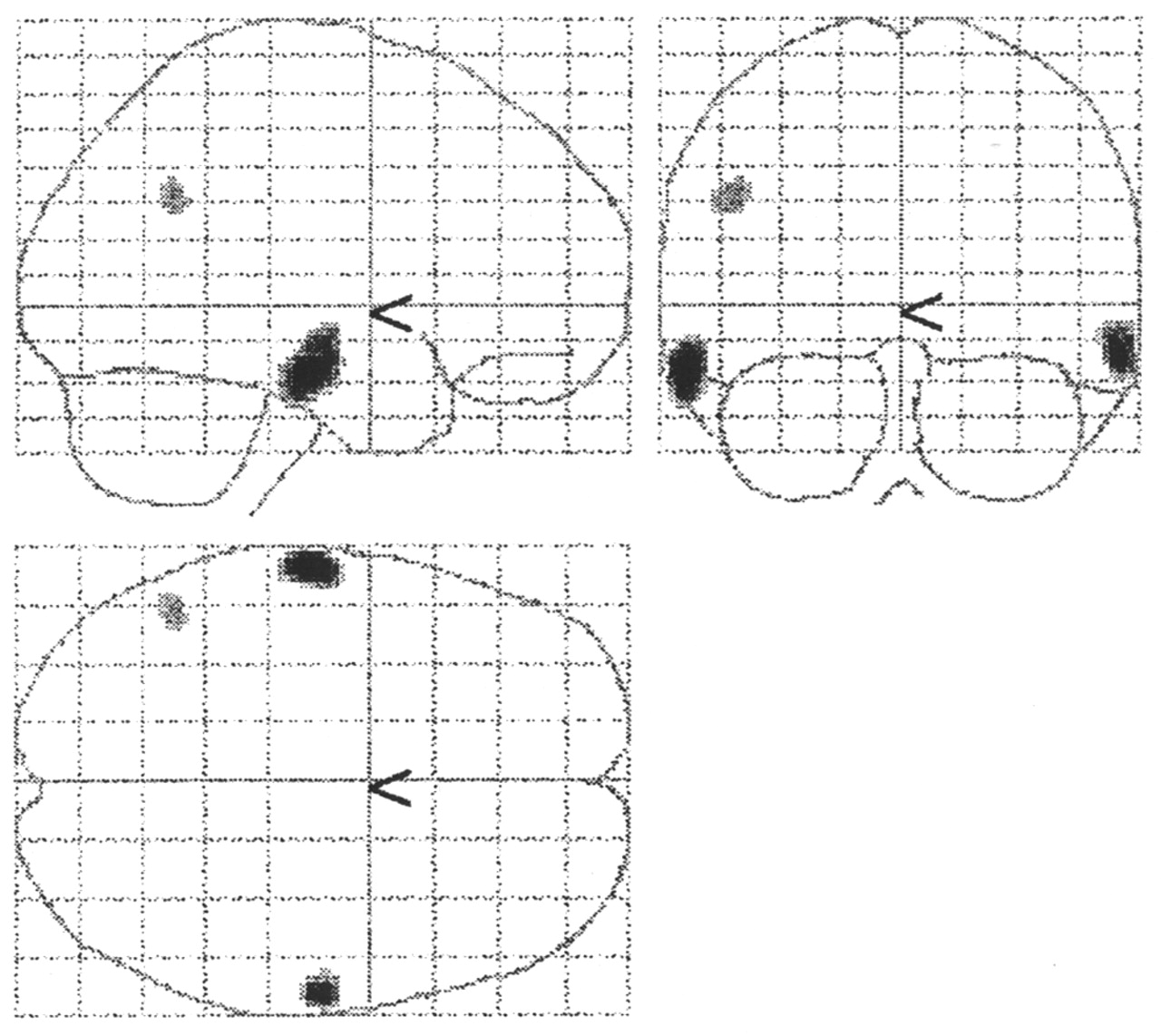
On the other hand, using decreased contrast for comparison of the activation images and the baseline scans both before and after milameline showed decreased rCBFs in the areas of the splenium of the corpus callosum. These are shown in Figures 2A and 2B, before and after medication, respectively. The Talairach coordinates of these regions are (4, −30, 12) and (4, −42, 12) before medication (Fig. 2A) and (−16, −36, 12) after medication (Fig. 2B) with T scores of 4.60, 4.26, and 5.93, respectively (P < 0.001). These results show that memory stress also caused rCBF reductions in deeper structures within the brain. There is a small difference between before and after milameline in that the decreased rCBFs are located at the center right before the medication (Fig. 2A), whereas the decreased rCBF appeared at the center left after the medication (Fig. 2B).

Decreased rCBFs caused by cognitive activation before (A) and after (B) milameline. Talairach coordinates are (4, −30, 12) and (4, −42, 12) before and (−16, −36, 12) after medication. T scores are 4.60, 4.26, and 5.93, respectively (P < 0.001).
Comparison of the activation scans (using decreased contrast), before and after milameline, resulted in decreased rCBFs as shown in Figure 3. Their Talairach coordinates are (−62, −18, −18), (62, −14, −16) at both sides of the temporal cortex and (−46, −54, 32) at the left parietal cortex. Their T scores are 5.51, 5.21, and 3.99, respectively (P < 0.001). No statistically significant increase in rCBF was evident after milameline (using increased contrast).
Decreased rCBFs obtained from contrast of activation images after milameline. Talairach coordinates are (−62, −18, −18), (62, −14, −16), and (−46, −54, 32) with T scores of 5.51, 5.26, and 3.99, respectively (P < 0.001). No statistically significant increase in rCBF was evident after medication.
Comparison of the baseline images, before and after milameline, failed to show any difference with statistical significance (using both increased and decreased contrasts). This is in contrast to the decreased rCBFs found on the activation images. However, image subtractions on individual baseline images, before and after milameline using our in-house program, did show rCBF changes (not shown), with different patients having rCBF changes (increase or decrease) at different locations. These changes were not significant on the statistical tests in the group analysis using SPM99.
DISCUSSION
Memory stress challenge caused an increase in rCBF in many areas of the brain as shown in Figure 1. This is consistent with the belief that memory is linked with the association cortex (11,12). Memory impairment is the hallmark of AD (37), and it is not surprising that reduced rCBF has been found in parietal, parietotemporal, temporal, and frontal regions of AD patients (11,12). The increased rCBFs in many regions from memory stress support the view that AD is linked with several regions of the brain (11,12).
More interesting results are those of decreased rCBFs at the splenium of the corpus callosum after the activation challenges as shown in Figures 2A and 2B. There is increasing evidence that AD is linked with rCBF reduction in deeper brain structures (6,15,34,37), such as the posterior cortex of the cingulate gyrus (34) and hippocampal regions (15,37). Rodriguez et al. (15) suggested that the reduction in rCBF in the hippocampal region could be a marker of the severity of AD, whereas no difference in rCBF has been demonstrated in this region between AD patients and normal control subjects (38). The rCBF reduction at the splenium of the corpus callosum is in the vicinity of the posterior cingulate gyrus. This area is believed to be part of the limbic circuitry and the association cortex (34). Reduced rCBF in the splenium of the corpus callosum has been demonstrated as caused by memory stress. These results suggest that memory stress activation results in rCBF increases in many cortical regions, at the expense of the reduced rCBF deeper within the brain, in those individuals with AD. Darcourt et al. (6) suggested that territories in jeopardy have a preserved rCBF at rest and can only be detected in stress conditions. The present results seem to suggest that the rCBF reserve at the splenium of the corpus callosum was exhausted by stress activation on patients with AD.
Further interesting results were obtained, including the fact that decreased rCBF was observed in the temporal and parietal cortex (Fig. 3), on activation images, whereas there was no statistically significant change in rCBF when baseline images were compared. This finding indicates that the activation SPECT images are more effective in detecting the rCBF changes in AD patients than are the baseline SPECT images (6,7). Moreover, decreased rCBF was observed after milameline treatment. This is consistent with the report of a negative effect of milameline on AD patients (39). Theoretically, any improvement in those with AD after drug treatment is generally linked to increased rCBF (1–10). However, milameline has partial muscarine agonist properties and has been reported to be safe for the treatment of AD (24–29). Hartvig et al. (40) reported that no change in rCBF after milameline infusion was detected using PET on 2 monkeys. The decreased rCBF at temporal and parietal regions from the present analysis could also be the progression of AD rather than the effects of milameline on the patients because the SPECT scans were acquired some 20–24 wk apart between medication. In fact, the rCBF reduction at the temporal and parietal cortex has long been regarded as the marker of AD (1–15).
CONCLUSION
Cognitive activation and SPECT imaging are more effective than that of baseline scans in detecting changes in rCBF in patients with AD after milameline. No statistically significant difference in rCBF has been demonstrated on baseline scan images. Memory stress activation on AD patients caused rCBF increases in many regions of the brain, including the parietal, parietotemporal, temporal, and frontal cortex, but also decreased rCBF at the splenium of the corpus callosum located deep within the brain. Reduction in rCBF at the temporal and parietal cortices after milameline supports the theory that milameline has a negative effect on the rCBF in those with AD-type dementia.
Acknowledgments
The author thanks Dr. Maurice Goodear (Albury Nuclear Medicine, Albury, New South Wales, Australia) and Dr. Bill Muratidis (Canberra Hospital, Canberra, Australian Capital Territory, Australia) for critical review of this manuscript. The author also thanks Dr. Julian Trollor (Neuropsychiatry Institute, Prince of Wales Hospital, Sydney, New South Wales, Australia) and Dr. Walter Haindl (Nuclear Medicine Department, Prince of Wales Hospital) for discussion at an earlier stage of this work. The AD patients and the milameline drug trial were part of a research project led by Dr. Julian Trollor. This image analysis work was initiated while the author was working in the Nuclear Medicine Department, Prince of Wales Hospital. This work was supported by a Charles Sturt University Research Grant (A514.171.xxx.9492).
Footnotes
For correspondence or reprints contact: Xiao Ming Zheng, PhD, School of Clinical Sciences, Faculty of Health Studies, Charles Sturt University, Wagga Wagga, New South Wales 2678, Australia.
E-mail: xzheng{at}csu.edu.au
REFERENCES





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.