


Abstract
Lymphoscintigraphy for sentinel node (SN) localization was performed on a 60-y-old man with a melanoma on his back. Skin contamination occurred as a result of the radiopharmaceutical dose administration. Skin contamination could result in a misinterpretation of the SN location. Careful observation of the procedure avoided a misinterpretation with this study.
A renewed interest in lymphoscintigraphy has occurred in recent years. This interest has been directed primarily at localization of the sentinel node (SN) draining a malignant tumor. The SN is the first node draining the tumor bed. Surgeons are interested in knowing if a malignancy has infected the SN. Lymphadenectomy can be avoided if the SN is not infected with tumor cells. The usefulness of lymphoscintigraphy for the identification of SNs in patients with melanoma is well documented (1–3). If the SN is not identified, the surgeon must remove and biopsy multiple lymph nodes.
In our institution lymphoscintigraphy is routinely performed on patients with melanoma and breast tumors. We have performed the procedure on patients with melanoma in many different locations on the body from head to foot. We do not routinely use lidocaine to help numb the skin. On the basis of our experience, we have not found that lidocaine significantly lessens the burn associated with intradermal injections. Our procedure is similar to that described in the Nuclear Medicine Procedure Manual (4). A small amount of contamination can result during the injection technique, which can cause a misinterpretation of the scan findings. We present this case study as an example of contamination by spray along the head and neck of the patient.
CASE REPORT
Lymphoscintigraphy for melanoma SN localization was performed on a 60-y-old man. The patient’s melanoma was located on his back between the shoulder blades, off center to the right. The melanoma was approximately 1 cm in diameter. Four intradermal (subcutaneous) injections of filtered 99mTc-labeled sulfur colloid (SC) were administered by a resident around the tumor site: 1 each above, below, and to the left and right of the tumor. Each of the 4 injections contained approximately 18.5 MBq (0.5 mCi) in 0.1 mL. The diameter of the injection site was approximately 1.5 cm. The patient was in the prone position for the injections.
One hour before receiving the injections of the 99mTc-SC, the patient was given 37 MBq (1 mCi) 99mTc-methylene diphosphonate (MDP) for anatomic referencing. The MDP injection was given in the anticubital region of the left arm. Care was taken to avoid any infiltration of the dose, which could be picked up subsequently by the lymphatic system draining that region.
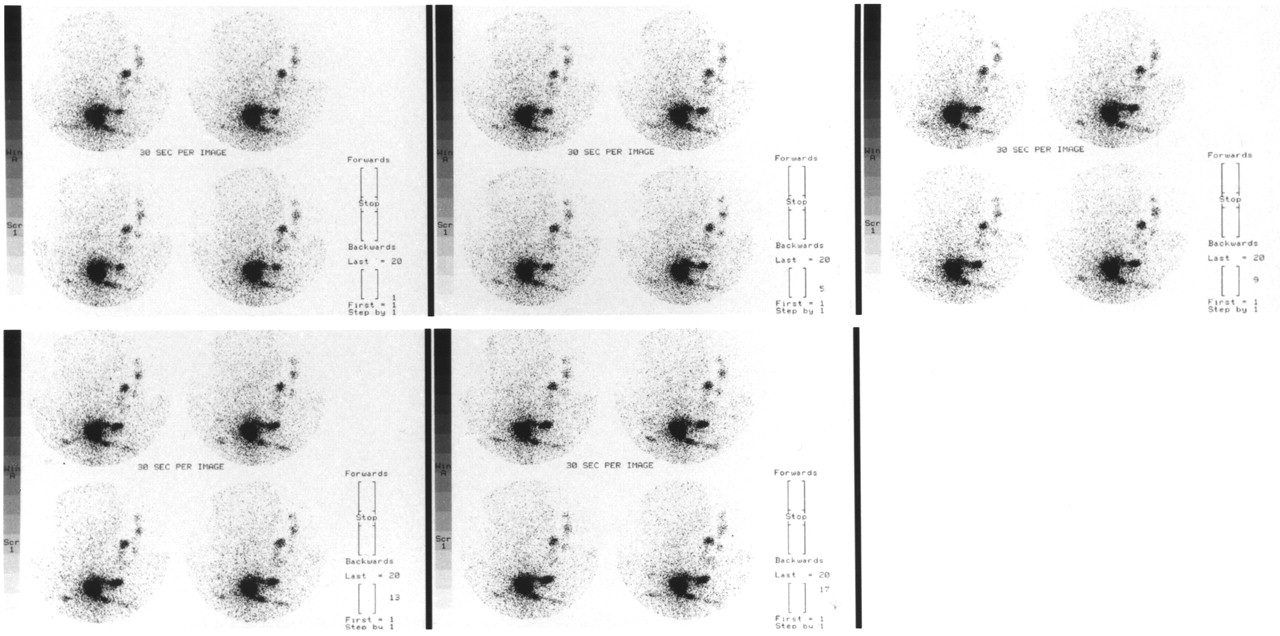
Immediately after the 99mTc-SC injections, the patient was put in the supine position for imaging. Posterior images of the head and upper back were taken with the camera beneath the patient. Twenty images, 30 s each (10 min total), were acquired followed by acquisition of five 5-min static images. The flow-study images are seen in Figure 1. Figure 2 shows the 5 static images.

Flow study images acquired 30 s apart. Images of flow study show area of contamination starting with earliest images (top left). Images were obtained from posterior projection.
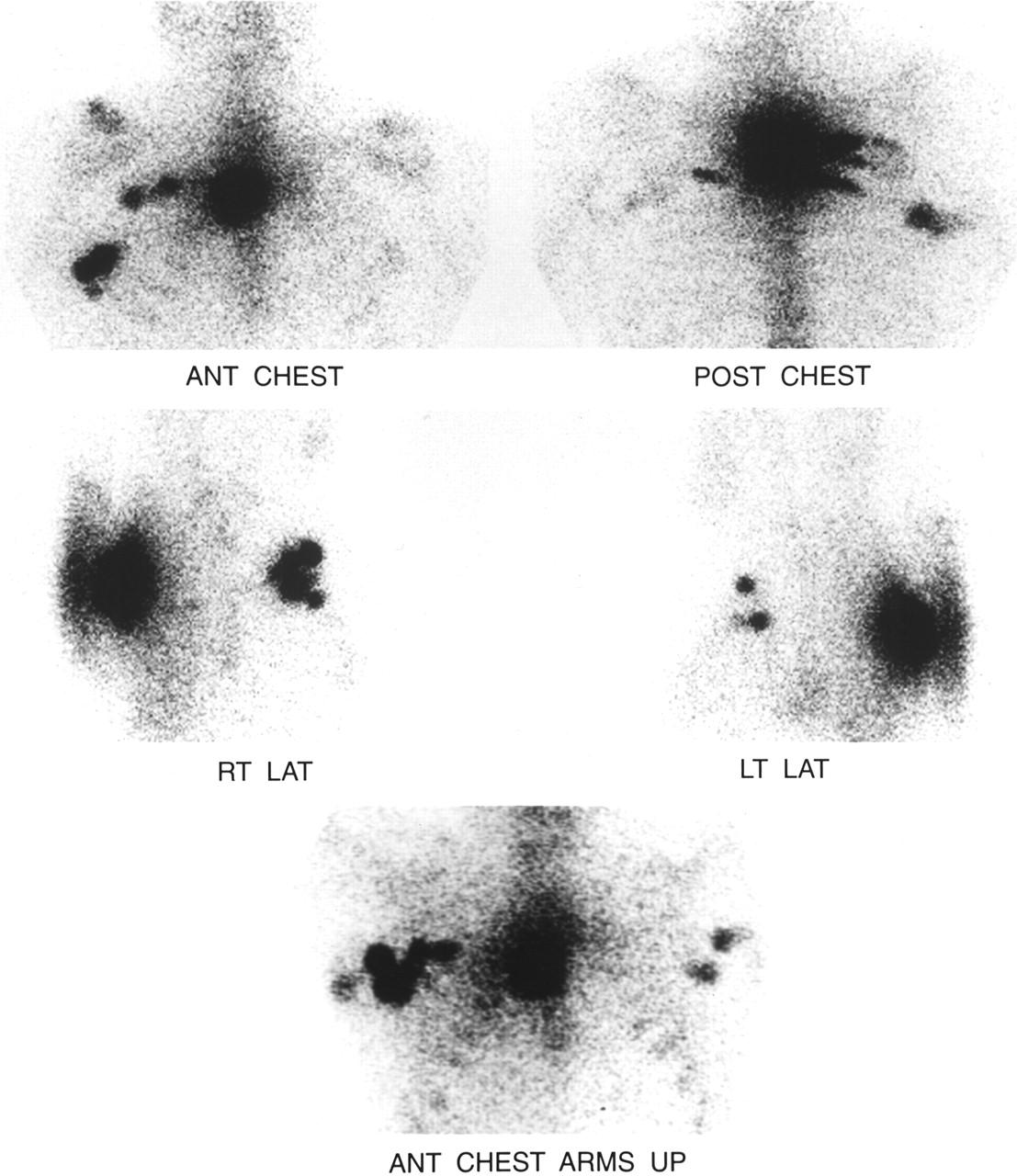
Static images obtained after cleaning patient to remove any suspected contamination. ANT = anterior; POST = posterior; RT = right; LAT = lateral; LT = left.
From the injection site the images are observed for movement of the tracer or tails leading to focal areas of tracer uptake, which represent a node. The flow study showed movement of the tracer superiorly to the right of the tumor site. The superior movement appeared to have nodal progression in the neck, which was visible on the first flow image. The fact that nodal progression showed up so quickly was suspicious. Although nodes can be visualized shortly after the injection, they do not usually appear from the onset or the first image of a flow study. Also, the hot spots seen on the flow-study images appeared to be outside the body contour outlined by the distribution of 99mTc-MDP. This could only mean contamination.
A technologist cleaned the patient’s neck, back, and shoulders with a washcloth. The images of the chest were taken after cleaning the area of suspected contamination on the patient. The static images were acquired using a different camera. Before taking the static images, the bed sheets were scanned to verify that they were not contaminated. The static images were acquired in the following order: anterior, arms down; posterior, arms down; right lateral, arms up; left lateral, arms up; and anterior, arms up. After all images were obtained, the doctor used a cobalt marker and an ink marker to locate and indicate the locations of the hot spots on the skin using the persistence scope. The static images did not show any superior movement toward the neck and upper back. They did display multiple nodes in the left and right axillary regions. The anterior image with the arms down masked the hot nodes on the left side, which were clearly visible on the anterior and left lateral images with the arms up.
DISCUSSION
Contamination by spraying of the radiopharmaceutical is uncommon but does occur occasionally. The direction and distance of spray vary. Draping the area around an injection site and the use of gauze are useful but may not be adequate to avoid contamination by spraying.
Spraying of the radiopharmaceutical has several causes. The location of the tumor has an effect. Some areas of the body have tough skin that is tightly stretched, whereas it is looser in other areas. The back, in particular, can be taut and firm on some individuals. If the skin is not pliable and does not accommodate the dose volume, spraying will occur. Spraying often results from excess pressure, which causes some of the radiopharmaceutical to shoot back toward the physician who is administering the dose. This is especially true if the patient is sitting upright when the injection is given. In this case, the direction of the spray was not toward the physician.
The larger the volume administered, the greater the chance of contamination by spraying. To avoid this problem, each dose should be preferably 0.05 mL. In this case, the volumes administered were closer to 0.1 mL. Also, the physician who is administering the dose needs to judge the resistance he or she feels as the dose is injected. In some cases, slightly less than the entire volume should be administered to avoid spraying.
Certain areas of the body are more sensitive than others. The patient is more likely to move in sensitive areas, which could result in contamination. For very sensitive areas of the body, we have had an anesthesiologist administer anesthetic before giving injections.
CONCLUSION
In this study, some of the volume from the superior injection was lost because of spraying. Enough activity was administered to give flow information, though perhaps with less sensitivity.
Physicians and technologists performing this procedure need to be alert to the possibility of skin contamination caused by spraying of the radiopharmaceutical. Contamination may cause a hot spot that could be misinterpreted as a node.
Acknowledgments
The authors acknowledge Cleolius Calloway, who assisted with decontamination and took the static images.
Footnotes
For correspondence or reprints contact: John Warner, CNMT, 5889 Dover Rd., Lake View, NY 14085.
E-mail: jwarner{at}roswellpark.org





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.