


Abstract
Objective:A trend in corporate healthcare is the merging of small community hospitals with larger regional hospitals to expand the patient base. The purpose of this article is to illustrate the benefits of operating several nuclear medicine departments under a centralized management system, rather than operating many decentralized departments. The issues discussed are the development, financial benefits, operations, and structure of a corporate nuclear medicine department. Methods: Seven nuclear medicine departments were integrated to form one corporate nuclear medicine department from a large hospital organization comprising seven different hospitals. The management team created the concept and advised administration. Training programs were designed and implemented, and committees were formed to ensure the efficient operation of the integrated department. All aspects of the department, such as scheduling and interpretation of studies, are managed at a central location. All technologists rotate to all hospitals. Success was measured by cost savings, study turn-around times, and evaluation of patient and employee satisfaction. Results: It was found that establishing a corporate nuclear medicine department created a greater patient base by servicing a larger geographic area, and resulted in savings of $870,000 annually. Standardizing procedures and protocols allowed for consistency in patient care, an inpatient turnaround time of 24 h, and a dictated report turnaround time of 30 min. Employee relations and satisfaction remained consistent with a 4.76 out of a 5.0 leadership index rating. Conclusion: A nuclear medicine department with a centralized management system is a viable option for corporate health care. It is recommended for operations endeavoring to expand the patient base and improve the financial picture.
The trend of large, regional health care systems merging with smaller local hospitals is spreading across the country. An effective way to integrate newly acquired satellite hospitals into a corporate system is to adopt a centralized management model. The development of one such corporate nuclear medicine department is presented in this article. This article discusses the integral developmental issues of organizational structure, personnel staffing and scheduling, and standardization of department protocols as they relate to this case study.
The hospital system described in this paper, Orlando Regional Healthcare (ORH), comprises 7 affiliated hospitals with approximately 1700 beds. The hospital system is a private, not-for-profit, community-owned hospital, the 10th largest hospital in the state of Florida. It serves 4 counties and approximately 575,000 people in health care, including a level-1 trauma center, a regional burn center, a cancer center, a sports medicine center, and an international business program serving 6000 international patients per year. The organization employs 12,000 team members, was recently recognized as one of the best hospitals in America by US News and World Report (1), and was named to Fortune’s (2) “Top 100 Companies to Work For”. The hospital system was formed as a corporate entity in the 1980s.
The 7 affiliates are described in Table 1. All of these hospitals operate as a single corporate entity with a centralized administration. Nuclear medicine is a centralized department with an administrative director and a manager—both board-certified nuclear medicine technologists. An organizational chart shown in Figure 1 clarifies the line of administration in the corporation. Five board-certified nuclear medicine physicians are staffed to read all nuclear medicine procedures. One physician acts as the designated radiation safety officer and approves all protocols. There are 24 full-time nuclear medicine technologists and 1 pool nuclear medicine technologist, all of whom are board-certified and Florida-licensed. Support staff includes 4 full-time and 2 pool registered nurses, 2 full-time ECG technologists and 1 pool ECG technologist, and 6 administrative assistants. The combined nuclear medicine department performs more than 50,000 clinical studies a year, including cardiac, oncology, MCD/PET, GI, and renal imaging.

Over the past 15 years, ORH Nuclear Medicine has shared its expertise in the field with other hospitals and hashelped advance the skill level of their technologists. For example, technologists have been trained on state-of-the-art techniques such as MCD/PET imaging and have hosted continuing education courses on current studies, such as lymphoscintigraphy mapping for surgery. ORH is often called upon to answer questions pertaining to the development, maintenance, and continual improvement of its unique operation to meet today’s market challenges. For example, the nuclear medicine department offers tours for hospital administrators and their staff to view equipment, network, and operations of the department. This case study shows that functioning as a corporation instead of as individual hospitals can expand the patient base, while still allowing departments to run efficiently and offer exceptional patient care.
DEVELOPMENT
The administrative director and department manager conceptualized a corporate nuclear medicine department at ORH in 1985. The various nuclear medicine departments at the outlying sites operated independently for 10 y, administratively separate from radiology at each site. This section discusses the factors necessary for development of an integration plan.
Management/Administrative Support
When developing a corporate department, it is critical that the effort garners the full support of the administration and department managers of each site; without this cooperation, failure is inevitable. However, achieving this support can be challenging; this is due, in part, to resistance to change (3). For example, the administration at one hospital did not want to relinquish control of the department. The administration was concerned that management would not be present at the individual hospital location, that staffing may not be sensitive to individual community needs, and that extra expenses would be incurred. These concerns were addressed through continual meetings, presentation of benefits, and support from the nuclear medicine physicians. In addition, management must empower the staff to problem-solve for a successful working relationship to flourish. Depending on the communication process, equipment needs, and department reorganization, the development process can take as little as 90 d or as long as 2 y.
Communication
Communication is another crucial factor in the development process. Discussion between administration and management must cover the topics outlined below.
Information relevant to the department integration process. This should include timelines of when the staff will be notified of any changes, notification of when and if the physicians will be in a centralized location, and information about whether the equipment will be network compatible.
Development, management, and oversight of a corporate budget.
Staff integration into the corporate nuclear medicine department.
Impact on patient care during and after the incorporation.
Of all these issues, the greatest challenge was helping the administration understand that one department could run all sites, because each site has unique characteristics with different demands. The nuclear medicine management understood this concern, and was willing to make adjustments to meet the needs of each site to help facilitate open communication. For example, one site may have a higher volume of pediatric patients than the other sites within the corporation. To accommodate that site’s needs, the staff would be trained in pediatric care; not only would this training benefit the site, it would also benefit the technologists by increasing their technical capabilities. In addition, physician concerns would have to be addressed. For example, a staff of 5 physicians would not be able to accommodate all locations; therefore, a centralized nuclear medicine reading area was established at the “main” area. Administration and management realized that staffing additional physicians was not fiscally beneficial, and establishing the centralizing reading area would still allow for excellent patient care.
Once the decision is made to integrate a facility, it is imperative to bring together staff technologists in focus groups to hear their concerns. (4) During the ORH experience, the following common staff concerns were expressed:
Shifts, call-back, holidays, seniority, salary
New corporate protocols and procedures
Staff rotation to the other corporation hospitals
How the change would benefit the individual employee.
All of these concerns were resolved easily. To determine the level of expertise of each technologist, ORH spoke with the administration of the facility about to be acquired and agreed to pay the salary of the technologist for 1 mo to have that technologist work at the “main” location. During this 1-mo period, the technologist was assigned a mentor, who was there to answer the new technologist’s questions and to teach the procedures and policies. The most commonly asked questions pertained to seniority, scheduling, and where the new technologist would be working. ORH maintained the current staff’s seniority. The newly acquired staff member started as if it were his or her first day, unless another arrangement was made for a technologist with 15+ y experience. The new technologist was shown how the schedule works and told that all technologists would rotate to all locations.
Having personal experience with the future employer put most new technologists at ease and allowed for a more comfortable transition. This arrangement also provided management with the chance to observe new employees first-hand and to determine if the working relationship would be mutually beneficial. The ORH nuclear medicine management has been successful in integrating the staff in this manner and has offered all acquired technologists a position. Out of the 6 sites acquired in the past 15 y, only 1 technologist decided to leave to explore new opportunities.
Equipment
Integration of equipment can be a challenge when implementing departmental changes. Because all of the locations are networked for physician viewing, and to ensure consistency of patient care and procedures, it is imperative that the equipment be compatible and networked properly. If the equipment is not compatible with the current network, management and administration should negotiate and create a timeline for integrating and networking equipment before taking on the new department. Although in most cases the equipment at the acquired site is compatible with that of the main division, it is important that the equipment be thoroughly evaluated.
Financial
Financial benefits to the hospital will be of greatest concern when negotiating and discussing a corporate department with administrators. The greatest advantage is the ability to purchase in bulk. The ORH transition resulted in $300,000 in savings on equipment and service contracts, $150,000 in savings on supplies, and an additional $150,000 in savings on radiopharmaceuticals. The total savings, $600,000 annually for approximately 7 y, was obtained by taking advantage of a corporate price reduction, rather than purchasing for each individual department.
Staffing can also affect overall savings. In a corporate organization model, staff and support staff rotate between sites to cover workload needs and alleviate staff-to-patient fluctuation problems. Because management of the satellite departments is maintained under 1 administrator and 1 manager, separate leadership positions are unnecessary at each site. At ORH, this staffing method produced savings of $270,000 annually for 5 y. Together, bulk purchasing and rotating the staff resulted in a total cost savings of $870,000 annually, or $4,350,000 over 5 y. The financial benefits of a corporate integration are obvious.
Operations
ORH has a corporate central scheduling (CS) department that works closely with the department to ensure customer satisfaction. CS maintains information regarding scheduling and patient preparation for nuclear medicine procedures, and is often the first and only contact a patient has with the organization before arriving in the department. Considering that 70% of ORH nuclear medicine procedures are performed on an outpatient basis, the corporate model helps streamline registration, preapproval, and precertification, and channels patients to the appropriate site for their appointments. This has improved billing and reimbursement, and has reduced claim denials.
In addition to outpatient studies, ORH strives to maintain a demanding schedule for inpatient exams, which are expected to be completed within 24 h of receiving the order. Inpatient studies are expected to be completed the same day as ordered, whenever feasible. CS has access to all sites via GroupWise (Novell, Provo, UT) calendar software, enabling a more efficient workload distribution between sites and preventing one site from being overburdened while another sits idle. This also improves the quality of patient care and increases choices for patients, who can select from a wider variety of appointment times and choose the facility nearest to their home or work.
Patient access to the main nuclear medicine department has played a large role in the success of the corporate model. Optimal internal communication is critical to maintaining this success. Mandatory staff meetings are held monthly, a quarterly newsletter is distributed, and all staff members are assigned to committees. Studies are interpreted by the same group of board-certified nuclear medicine physicians at each site, improving consistency throughout the organization. The 5 board-certified nuclear medicine physicians are linked from the main location to the satellites via virtual network using synchronized optical network (SONET) ring technology, which allows communication between the outlying sites and the main location. Although this technology is crucial to the operations, there is a disadvantage to this configuration: If one site goes down, all sites go down. Therefore, ORH contracts with a network services company for 24/7 service to ensure continuous communication and to minimize interruption. The same network is then linked to the home of each nuclear medicine physician through the use of an integrated service digital network (ISDN). Seemor (ADAC Laboratories, Malpitas, CA) and Cemax-Icon (A Kodak Company, Freemont, CA) are used to transfer and view the images in the physicians’ homes. A unique password protection program provides security and maintains patient privacy.
Once the nuclear medicine physician receives images at the main location, communication between the outlying sites and the physician is essential. The following ORH protocol allows a 30-min turnaround time after completion of the study:
All face sheets with appropriate patient history, time of injection, technologist performing the procedure, and other relevant information are faxed to the physician reading room.
The nuclear medicine technologist at the site then alerts the physician that the information sheet has been faxed and answers any questions the physician may have regarding the patient’s condition or ability to comply with the demands of completing the exam.
The nuclear medicine physician must approve every study before releasing the patient from the department.
Stress gated thallium studies are reviewed upon completion of the stress processing. If the stress portion is normal, no additional imaging is done. The patient is released, and a report is given to the cardiologist. This process alone has saved many hours of valuable camera and imaging time.
Once the study is completed, the nuclear medicine physician dictates the official report by accessing the telephone dictation system. The ordering physician retrieves the report through a listen-access line before it is typed and distributed, if he or she chooses. Each site maintains a permanent administrative assistant, who files and transcribes completed patient charts. Individual chart numbers and folder colors are used for each site for ease of identification.
Structure
ORH’s corporate nuclear medicine department operates with 40 team members. Scheduling is based on the ability to offer excellent patient care, individual site needs, and budgeting concerns. Because the main facility has the largest volume of patients, the largest number of staff is assigned there on a daily basis. There are 10 nuclear medicine technologists scheduled each day for 8 different shifts, including the on-call technologist who does not report to work until 1500. In addition, two noninvasive RNs with advanced cardiac life support certification, 3 ECG technologists, and 4 administrative assistants are scheduled each day. The smaller sites are staffed according to trends in patient workload, practice patterns, the number of cameras operated, and on-call coverage. Each satellite has an RN and an administrative assistant.
The distance between hospitals and the need to maintain a 1-h response time to a call requires that 3 call teams rotate the on-call schedule: a south team (St. Cloud, Sand Lake and South Lake), a north team (South Seminole), and a “main” location team (Orlando Regional Medical Center, Lucerne, and Arnold Palmer Hospital). Each team is responsible for calls at the locations in its area, which means that technologists are not responsible for taking calls at all locations. The call period is for 7 d, Friday through Thursday. The call technologist’s arrival time Monday through Friday is later in the afternoon, to accommodate the probability that they were at the hospital performing procedures during the evening or early morning.
Recent increased patient census trends are a challenge for weekend coverage. The technologist staff at ORH was empowered to devise a plan to cover the increasing weekend volumes. Weekends are staffed with a rotating staff of 4 technologists, who do not take traditional calls but who cover all weekends for the year. Because each technologist is familiar with all sites and the procedures and protocols are standardized, all technologists know the idiosyncratic expectations of the satellites.
There are 33 different shifts to be scheduled corporate-wide. A senior technologist is assigned to create the staff schedule and submit it for approval by the manager. Everyone is expected to be multitask-oriented and to rotate to all sites and all assignments, which helps to maintain consistency of technical expertise among the sites. Quality control is performed every morning and assigned to the technologists with the first shift of the day. Specific studies are scheduled in specific rooms. Because all technologists rotate to all facilities, ORH can eliminate a lead technologist at each location and instead assign a technologist to make final decisions at each site.
The staff hierarchy is based on seniority and ability. The senior staff members are the decision-makers and work with the management team. Each senior staff member is assigned to chair a department committee. These committees are Core Group, Orientation Group, Procedural Group, Quality Assurance Group, Supply Committee, and Social Committee. Each group has a lead technologist that organizes regular meetings, keeps the group focused on the corporate mission statements, and informs management of the changing needs of the department. The responsibilities of each group follow.
Core Group comprises 7 senior technologists, who act as the voice of the staff. They have monthly meetings with management and discuss all questions and concerns from the staff members, who are aware they can bring questions to any of the Core Group technologists or management. Members of this group are also chosen to represent or chair the other committees, and must submit minutes from each committee meeting to management on a quarterly basis.
Orientation Group is responsible for mentoring newly hired technologists. Each new hire is paired with an experienced team member, who acts as a mentor (5). Mentors are responsible for familiarizing new hires with all facilities, encouraging efficient and accurate study performance, and introducing them to other team members. Mentors also supply new hires with weekly updates on their progress. Because of the rotation schedule, mentoring responsibilities may be delegated to other technologists, but the assigned mentors are ultimately responsible for the new hires’ readiness. The training is clearly documented by using a rubric to minimize miscommunication of expectations. When new procedures are introduced, this committee trains department team members on the acquisition parameters and data processing. They also are responsible for continuing education endeavors, to keep technical skills at an exceptional level.
Procedural Group maintains and updates the department’s procedure and policy manual. A copy is placed at each site. When new procedures are introduced, this committee creates the acquisition protocol and procedure with the approval of management and physicians. This group also generates a technical newsletter to update the team on the changes in the department, as well as trends in the industry.
Quality Assurance is the “checks and balance” committee. Accurate paperwork and daily quality control are extremely important and must be monitored. A quarterly individual update is given to each team member. A form generated by the committee provides a peer review of areas for improvement in charting and documenting.
In addition, 25 random charts are reviewed each month from all sites. The patient’s history, dose slip, films, patient education form, and acquisition parameters are reviewed. The technologist performing the study is responsible for these items, and must initial the paperwork. Missing items are reported in a quarterly report, which is given to each technologist to review, follow-up, and improve upon as needed.
Because 40 different people travel to 7 different sites, supplies and storage must remain consistent. The Supply Committee is responsible for this. Each supply cabinet throughout the department is assigned an individual number and labeled boldly on the outside of the door or drawer. For example, a number 1 on a master supply list also identifies the supplies that go into cabinet number 1. This supply list is posted throughout the department, which improves technologist efficiency and eliminates ordering errors.
Social Committee is responsible for team gatherings, collecting funds for social events, and sending flowers for special occasions to team members.
New committees can be implemented depending on the needs of the department. To overcome the challenges a corporate nuclear medicine department faces in fostering communication between hospitals, a Communications Committee can be developed. This committee would ensure that changes in procedures, written materials, and day-to-day activities are communicated to all team members via memo, fax, and telephone conversations. A checklist of the communication process would be used so that each team member could be held accountable for the information he or she received.
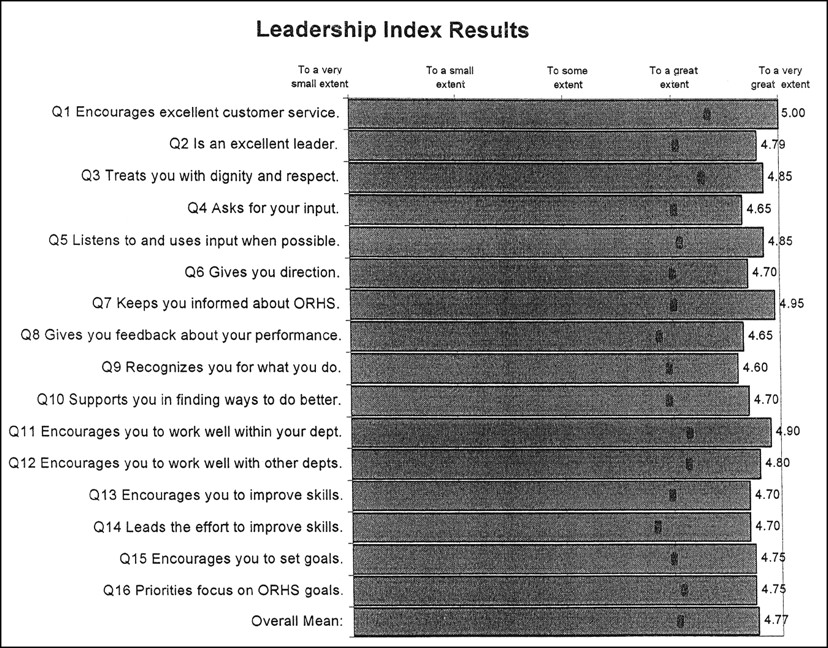
These committees underscore the corporate nuclear medicine department’s philosophy: teamwork. All team members know that they are part of the decision-making process for the department, which increases pride and participation in the daily work routine. This maintains a high morale in the department and can be documented through a leadership index. Each year, ORH employees rate their departments’ management and working environment. The nuclear medicine administrative staff has consistently received an average rating of 4.76 out of a 5.0; Figure 2 outlines the leadership index and the categories associated with the rating system.
CONCLUSION
This article discussed the concept of operating a multisite nuclear medicine department as a corporate entity, and described the development, operation, structure, and issues of creating such a department. The ORH experience has shown that corporate integration is a financially sound decision that supports commitment to excellence at all levels. Patients continue to express satisfaction with services received, and physicians are extremely happy with the patient care and timeliness in receiving reports. Staff morale is at a peak when the working environment offers decision-making opportunities and responsibilities; this, in turn, positively affects the quality of work performed.
This model successfully facilitated the integration of 7 different sites into a corporate department. The experiences reported in this article may offer substantive ideas for other departments with similar aspirations.
Acknowledgments
The authors would like to thank Rick Golab, Karen Blondeau, and Madeline Santana for their support and guidance with this paper.
Footnotes
For correspondence or reprints contact: Terry Worsley, CNMT, Manager, Orlando Regional Healthcare, Department of Nuclear Medicine, South Orange Avenue, Orlando, FL 32806; Phone: 407-841–5159; E-mail: TerryW{at}orhs.org.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.