


Abstract
It is of vital importance to optimize the radiation dose to patients undergoing radionuclide bone scanning. This is one of the most common nuclear medicine procedures in many parts of the world, including Nigeria, and the current study was performed as part of a national survey to establish diagnostic reference levels (DRLs) for common nuclear medicine procedures in Nigeria in order to optimize their use. Nuclear medicine was only recently introduced to the health-care system in Nigeria, with only 2 centers presently conducting these procedures. Methods: A retrospective, cross-sectional study was performed in the nuclear medicine department of a tertiary hospital in southwest Nigeria to determine the preliminary local DRL for radionuclide bone scanning. One hundred and nine patients who met the study criteria were included. Data were obtained from June 2017 to March 2019 and were analyzed to obtain the third quartile of the distributed administered activity and achievable dose (anthropometric variables and radiation dose to bone surface). Results: The mean administered activity, achievable dose, and DRL were 833.98 ± 106.93, 832.5, and 895.4 MBq, respectively. The calculated preliminary local DRL was larger than values reported in studies done in Sudan, the United Kingdom, and Australia or by the International Commission on Radiological Protection. Conclusion: The preliminary DRL from this first-of-its-kind study in Nigeria was high because of practitioners’ lack of experience. However, the values were still within the international best-practice range, which when optimized will go a long way toward reducing medical exposure without compromising image quality.
In medical imaging, protecting patients from exposure to radiation is a major concern calling for intervention, prompting the International Commission on Radiological Protection (ICRP) to recommend principles to justify use, optimize protection, and limit doses. In medical exposure, however, dose limits are not applicable per se, as they would defeat the purpose of justifying the practice (1).
The significant increase in the use of radiation for medical purposes has led to a concomitant increase in the exposure of patients, relatives, and the environment to radiation (2). In the early 1990s, the ICRP introduced the concept of diagnostic reference levels (DRLs) to optimize doses (3,4) and minimize the amount of applied radiation. According to Council Directive 97/43/Euratom, DRLs are dose levels in medical radiodiagnostic practices for typical examinations of standard-sized patients or in standard phantoms for broadly defined types of equipment (4).
The establishment of DRLs and achievable doses has proven to be an effective tool in optimizing protection in medical imaging (5). DRLs and achievable doses are as defined in ICRP publication 135, the former being the level that protects patients from exposure during diagnostic and interventional procedures and the latter being the DRL achievable by standard, widespread techniques without compromising image quality (i.e., the value set at the median [50th percentile] DRL determined in a departmental survey). DRLs define the lower and upper limits of administered activities in nuclear medicine and radiology and can be applied to the most common nuclear medicine procedure in Nigeria, bone scintigraphy (a sensitive diagnostic imaging method that uses a radiopharmaceutical to evaluate the distribution of bone formation relating to physiologic processes, in addition to malignant and benign disease). The examinations chosen for the DRL process should be those performed most often in the region and for which dose assessment is practicable (6).
DRLs help avoid delivering, to a patient, excess radiation that does not contribute to the clinical purpose of the medical imaging task. This goal is met by comparing the DRL (derived from relevant regional, national, or local data) with the mean value observed in practice for a reference group of patients (e.g., similar in height, weight, and age) or a suitable reference phantom (6). When a procedure consistently exceeds the DRL, that procedure and its equipment should be locally reviewed for adequate optimization, and dose-reduction measures should be taken if necessary (7). DRLs are based on the activities that need to be administered to normal-sized patients (typically with a body weight of 70 ± 15 kg) to achieve good image quality during a standard procedure (8).
The role of nuclear medicine in patient management is as impactful in a developing nation as in other regions of the world. However, in developing nations the practice of nuclear medicine faces a myriad of challenges; these, though, can easily be avoided (9).
The “Bonn Call for Action” in 2012 (10) increased global awareness of the need to strengthen radiation protection in medicine. Despite the huge progress in protecting patients from radiation in most developed countries (10), the situation in most developing countries is still far from ideal. Nigeria does not have a local or national nuclear medicine dose registry, which is important for establishing dose reference levels, and a literature search could find no previous studies in Nigeria to establish DRLs for radionuclide bone scanning. Therefore, optimization of protection is doubtful, and establishing DRLs in Nigeria is vital (11).
The current study addressed this challenge by establishing a preliminary DRL for bone scintigraphy, the most requested procedure in Nigeria, and by determining the role that achievable dose plays in reducing dose while maintaining diagnostic image quality.
MATERIALS AND METHODS
This was a retrospective and cross-sectional study performed in the nuclear medicine department of a tertiary hospital in southwest Nigeria. The data were collected from 2017 to 2019 and included 109 adults who were selected (using purposive sampling) (mean age, 57.9 ± 14 y [range, 34–87 y]; mean weight, 71.6 ± 6.7 kg; mean height, 1.63 ± 0.5 m; mean body mass index, 29.9 ± 3.0 kg/m2) (Table 1). The center was chosen because it had the imaging modality of choice and the facilities for the study.
Anthropometric Variables
Equipment Specifications
The radioisotope dose calibrator was a CRC-ISR (Capintec), with 100–240 V, 50/60 Hz, and 120 mA. The γ-camera was a model 4369372 SPECT device (Siemens) manufactured in November 2005, with 200 V, 50/60 Hz, 30 mA, and a line single phase.
Ethical Clearance
Ethical approval was obtained from the Research Ethics Committee of the Oyo State Ministry of Health. Also, data were anonymized and kept confidential in a personal computer, and the results did not contain any information that would allow the patients or center to be identified.
Procedure
Departmental documents and records were made available to the researcher, who was a former staff member of the center and one of the pioneer radiographers in its imaging unit. Data were generated and sorted to capture the needed details. The departmental protocol for bone scintigraphy included preparing the radiopharmaceutical (99mTc-methylene diphosphate), measuring it with a dose calibrator in the radiopharmacy hot lab, administering it intravenously to referred patients while they lay supine on the SPECT γ-camera, and acquiring planar images using the window and persistence routinely applied in the department. The activity administered and other anthropometric parameters were recorded for each patient.
Method of Measurement
DOSISRAD software was used to automatically calculate the absorbed dose to organs and the effective dose from the administered activity of the radiopharmaceutical (12). This software is based on the ICRP values, and the calculation was specific to the type of imaging study, clinical indication, patient’s weight, type of radiopharmaceutical, and administered activity (MBq).
Data Analysis
The data were saved in a Microsoft Excel spreadsheet and categorized for the examination parameters and anthropometric parameters. SPSS software (version 23.0; IBM) was used to analyze the mean and SD of the administered activity, anthropometric variables, and radiation dose to the critical organ (bone surface). The achievable dose and DRL were obtained from the distribution of the administered activity for radionuclide bone scanning. Parametric testing was suitable because there was a normal distribution at a 95% CI after using the Kolmogorov–Smirnov method to test for the normality of data distribution. Statistical significance was set at a P value of less than 0.05.
RESULTS
Table 2 shows mean, minimum, maximum, achievable dose (second quartile), and DRL (third quartile) data for administered activity and critical-organ dose.
Administered Activities and Critical-Organ Doses
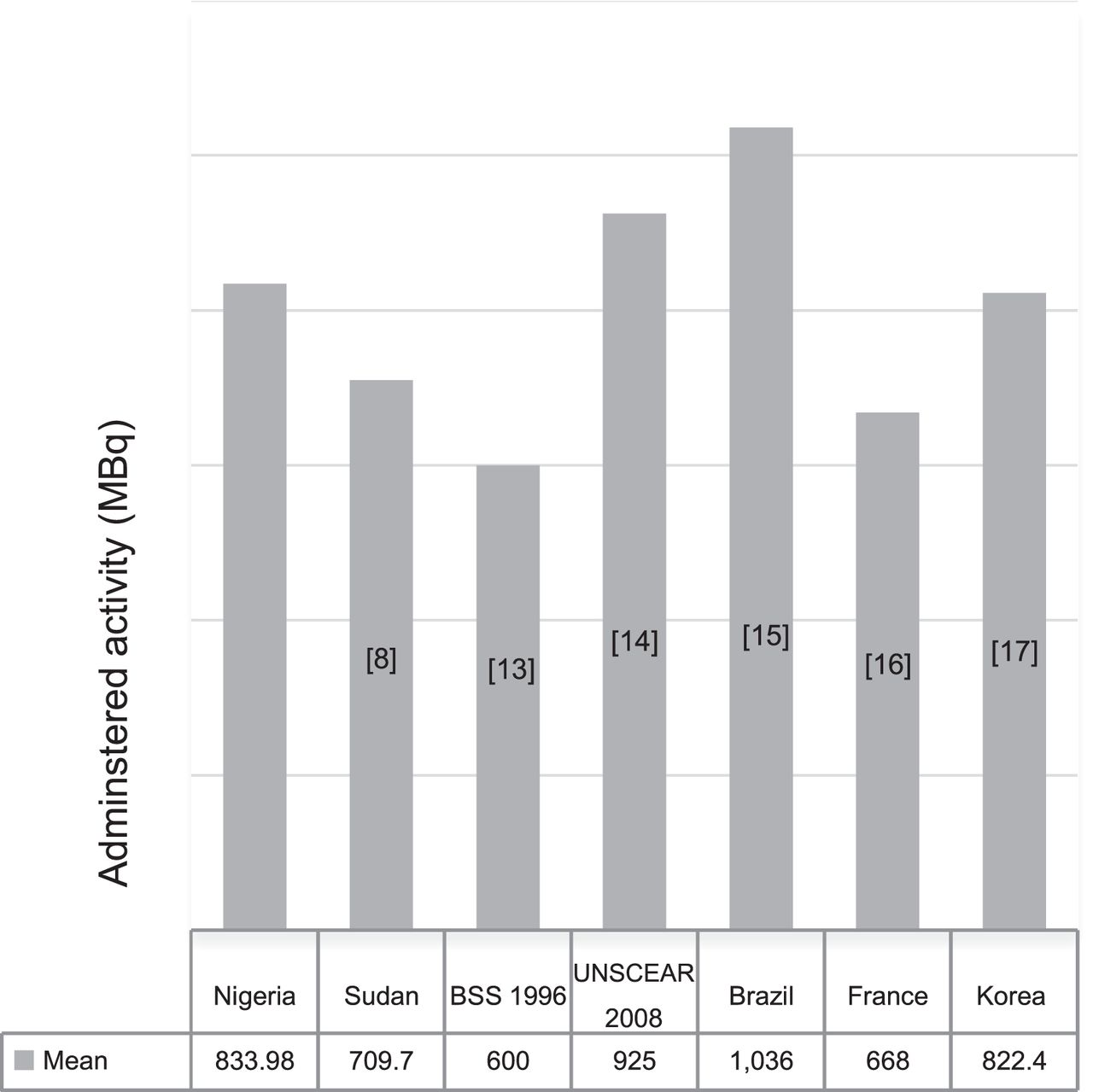
The mean administered activity, 833.98 ± 106.93 MBq, translated to a mean dose of 52.54 ± 6.31 mGy to the bone surface. Figure 1 compares this mean administered activity with the mean values in Sudan (8), Brazil (13), France (14), and Korea (15) and with the 1996 basic safety standard (16) and the 2008 standard of the United Nations Scientific Committee on the Effects of Atomic Radiation (17). The Nigerian mean value was lower than the United Nations standard and the Brazilian mean value but higher than the other mean values and standard.

Comparison of mean administered activity (MBq). BSS = basic safety standard; UNSCEAR = United Nations Scientific Committee on the Effects of Atomic Radiation.
The maximum activity administered was quite high, at 1,124.8 MBq; only Brazil had a higher value (1,480 MBq).
At 832.5 MBq, the achievable dose in this study was lower than the mean administered activity of 833.98 MBq (Table 2). However, the difference was not significant.
The DRL (895 MBq) was within the European Union range of 500--1,110 MBq (Table 3) but below the Brazilian DRL (1,110 MBq (13)) and the Australian DRL of 920 MBq (18) and above the Sudanese of 777 MBq and U.K. of 600 MBq DRLs (19).
Comparison Between Local DRL and International Standard Values
DISCUSSION
This study established preliminary DRLs for bone scintigraphy in a tertiary hospital in southwest Nigeria, the only teaching hospital that offered nuclear medicine services at that time.
Anthropometric Variables
The high mean body mass index indicates that many of the patients being scanned for the various indications were overweight. The maximum body mass index fell within the severely obese class, at 37.99 kg/m2 (reference range for severe obesity, 35–40 kg/m2), a value that increases the risk of many types of cancer, such as cancers of the breast, colon, and endometrium.
Maximum Administered Activity
The high maximum administered activity may stem from a lack of standardized protocols and may indicate use of an unnecessarily high radiation dose. Hence, there is a need to audit, regulate, and optimize doses. The minimum and maximum administered activities for the same type of procedure have been observed to range widely, by 44% (20). Nonstandardization of activities administered for the same type of procedure can denote a deficiency in controlling for radiation exposure.
Mean Administered Activity
The mean administered activity in Nigeria, though within the international range, clearly points toward use of an unnecessarily high activity, which in turn increases the radiation dose to the patient. This finding indicates that neither a guideline nor a reference value is in place to guide personnel in optimizing medical exposure while retaining diagnostic image quality.
Achievable Dose
Achievable dose represents the 50th percentile (median) (21) of the dose distribution, as defined by the ICRP and the International Atomic Energy Agency, and is recommended as a reference to prevent excessive ionizing radiation. Figure 2 shows that our calculated value was within the range reported by the Society of Nuclear Medicine and Molecular Imaging, the American Society of Neuroradiology, and the European Association of Nuclear Medicine but fell below the ranges reported by the American College of Radiology and the National Council on Radiological Protection. Achievable dose has an additional role in optimization, as some degree of patient dose reduction can be attained without affecting image quality. Extrapolation of this value into current practice for radionuclide bone scintigraphy could reduce the dose by approximately 26%, a highly significant degree of optimization.
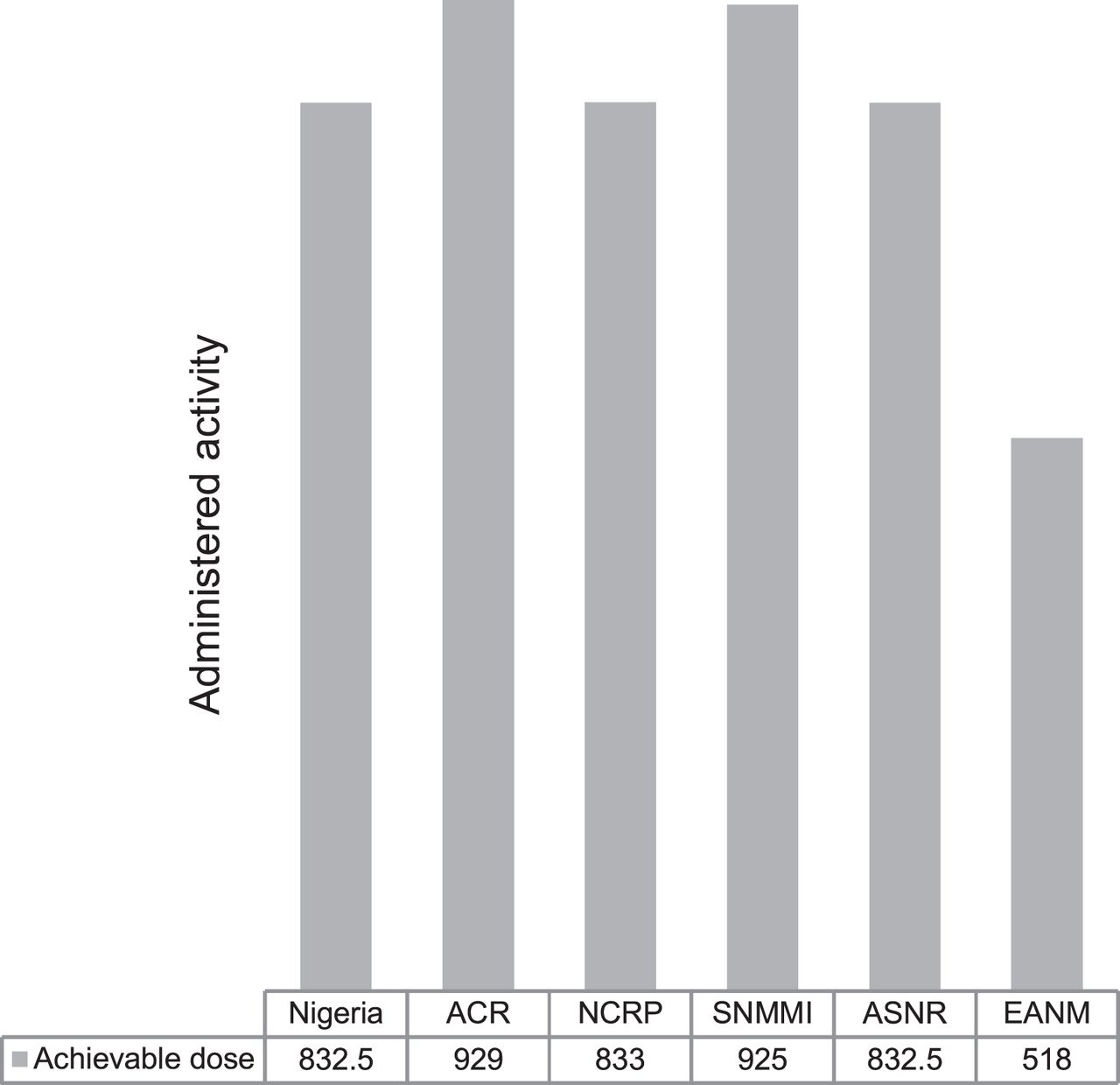
Comparison of achievable dose (19) with others indicated in literature. ACR = American College of Radiology; ASNR = American Society of Neuroradiology; EANM = European Association of Nuclear Medicine; NCRP = National Council on Radiological Protection; SNMMI = Society of Nuclear Medicine and Molecular Imaging.
Preliminary DRL
If the DRL is consistently being exceeded, the procedures and equipment should be reviewed to determine whether further optimization is needed to protect patients and, if so, dose-reduction measures taken (7). Our findings during this developmental phase in Nigeria showed a moderate level of safety, even though doses were sometimes administered without considering whether both patient protection and image quality had been optimized. Application of DRLs will help avoid administering an unwarranted radiation dose that does not add clinical information to the images. Establishing a national DRL will provide a dose-optimization tool to guide other nuclear medicine centers in Nigeria.
Limitations
The study, being retrospective, had some outliers too small or large for the age and weight ranges. Caution is therefore advised in applying the values.
CONCLUSION
Optimization of protection in Nigeria is doubtful, as no reference records are kept in daily practice, and a literature search could find no previous studies to establish DRLs for radionuclide bone scanning, the most common nuclear medicine procedure in southwest Nigeria. This first study to determine local DRLs and achievable doses for bone scintigraphy found values higher than those in some other countries and international bodies. Application of these DRLs in subsequent studies will significantly reduce unnecessary exposure of patients to medical radiation. In determining the minimum practicable radiation dose, one should use sound judgment and have a clear reason to administer the radiation. Inconsistency in the activity administered for the same procedure calls for concern, as wide differences in administered dose were noted without additional image quality, signifying a lack of local regulations, evidence-based protocols, and standard operating procedures.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
For their support, we thank Muideen Isa; Wasiu Lamidi; Ezinma Micheal (Deputy Director of Radiography and Nuclear Medicine Radiographer, University College Hospital, Ibadan); Idris Garba (HOD, Radiography, Bayero University, Kano); Prof. Tijjani H. Darma (Department of Physics, Bayero University, Kano); the Radiation Protection Research Group, University of Nigeria, Nsukka, headed by Prof. Kenneth K. Agwu; and HOD, Nuclear Medicine Centre, University College Hospital, Ibadan.
Footnotes
Published online July 30, 2021.
REFERENCES
- Received for publication February 16, 2021.
- Revision received May 21, 2021.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.