


Abstract
Objective:Over the past few years, we have performed several brain SPECT studies on patients who have had previous head trauma that required metallic cranioplasty. Transaxial images showed clearly defined photon-deficient areas extending from the brain tissue into the area of the scalp. To investigate the extent and pattern of this type of artifact, SPECT brain phantom studies were performed and compared with the patient studies.
Methods:SPECT brain phantom studies were performed using various metallic sheets to simulate metallic plates that were used for cranioplasty.
Results:Phantom studies using lead to represent tantalum plates were similar to our patient studies; that is, the photon-deficient area in normal brain tissue extended into the area where normal scalp activity would be. There was also increased tracer activity at the periphery of the photon-deficient area that extended to where normal scalp activity would be. This was similar to the patient studies and was not present on the phantom studies done without any metallic sheets present.
Conclusion:One would expect photon-deficient artifacts caused by radiopaque metallic plates in brain SPECT studies. The patient and phantom studies demonstrate that an increased tracer activity artifact is also present at the periphery of the photon-deficient area that extends into the area of the scalp. Knowing the appearance of this type of artifact caused by radiopaque metallic plates in brain SPECT studies could be beneficial, especially in cases with poor patient history and lacking radiographic correlation.
We have performed several brain SPECT studies in the past few years on patients that had previous head trauma that required metallic cranioplasty. The head trauma was not recent (>20 y prior to the study) and was not the indication for the study. To investigate the extent and pattern of the effect of metallic plates on brain SPECT studies, we performed several SPECT brain phantom studies using various metals to simulate metallic plates that had been used for cranioplasty.
MATERIALS AND METHODS
Three patient brain SPECT studies were evaluated. Patient 1 was a 76-y-old man with cerebrovascular accident (CVA) on the right with left hemiparalysis. His trauma occurred while in the military during World War II. Patient 2 was a 52-y-old man with a history of chronic alcohol and nicotine dependence who was referred for brain SPECT because of seizures. He had head trauma with a skull fracture 25 y before this study. Patient 3 was a 72-y-old man with head trauma in World War II who was referred for brain SPECT because of frontal lobe syndrome. After intravenous administration of 1,110–1,147 MBq (30–31 mCi) of 99mTc-ethylcysteinate dimer (ECD) and appropriate delay, brain SPECT imaging was performed with a triple-head SPECT camera equipped with low-energy, ultrahigh-resolution parallel hole collimators (patient 1) or low-energy, ultrahigh-resolution fan beam collimators (patients 2 and 3). An energy window of 20% centered at approximately 140 keV was used. The 128 × 128 study was acquired using a magnification of ×1.6 (patient 1) or ×1.0 (patients 2 and 3) for 7 consecutive acquisitions of 40 steps at 3° per step and 4 s per step. The multiacquisitions were summed if no patient movement was seen between acquisitions, converted to 64 × 64 to allow for 3-dimensional (3D) processing, and prefiltered using a ramp filter. SPECT reconstruction was processed using a Butterworth filter (order, 4.0; cutoff frequency, 0.30 cycles/pixel). The original 128 × 128 studies were archived for future reprocessing if needed.
A review of the surgical literature (1–4) indicated that aluminum, stainless steel, and tantalum with thicknesses of 0.064, 0.046, and 0.038–0.051 cm, respectively, have been commonly used for cranioplasty. Most of the metallic cranioplasties done during and following World War II used tantalum. We were unable to obtain any clinically used metallic plates; therefore, we used non–surgical-grade aluminum, stainless steel, and lead sheets (3.5 × 5.0 cm). Lead was used to simulate tantalum, which was unavailable. Table 1 summarizes metallic plate/sheet information.
Summary of Metallic Plates/Sheets Used for Cranioplasty and Phantom Study
Using a commercially available SPECT brain phantom filled with 99mTc, several SPECT studies were acquired on a triple-head SPECT camera equipped with low-energy, ultrahigh-resolution parallel hole collimators, with and without the various metallic sheets in place. The low-energy, ultrahigh-resolution fan beam collimators were not tested, given that they were no longer being used for clinical brain SPECT studies. An energy window of 20% centered at approximately 140 keV was used. Studies were acquired in 128 × 128 with a magnification of ×1.6 for 7 consecutive acquisitions of 40 steps at 3° per step and varying s per step, so the counts per step were comparable to clinical studies. The multiacquisitions were summed, converted to 64 × 64, and prefiltered using a ramp filter. SPECT reconstruction was processed using a Butterworth filter (order, 4.0; cutoff frequency, 0.30 cycles/pixel), similar to clinical studies.
In addition to the SPECT studies, a planar image was acquired of a 99mTc-fillable flood source, with each type of metallic sheet placed between it and a single-head gamma camera equipped with a low-energy, all-purpose collimator. An energy window of 20% centered at approximately 140 keV was used. Counts from a region of interest (ROI) over each area attenuated by a metallic sheet were compared with counts from several ROIs throughout the uniform part of the image. From these ROI counts, the percentage attenuation was calculated for each metallic sheet tested.
RESULTS
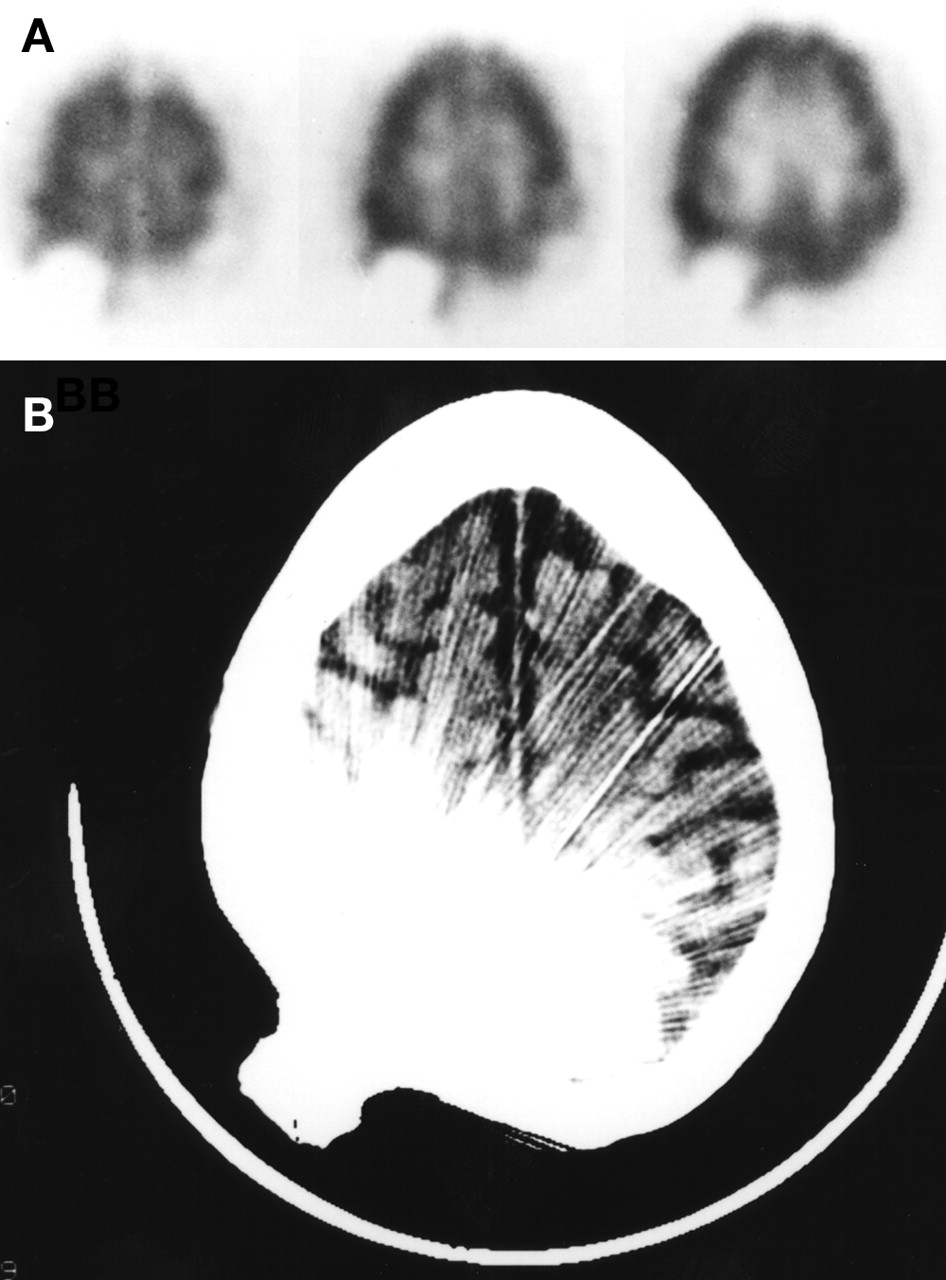
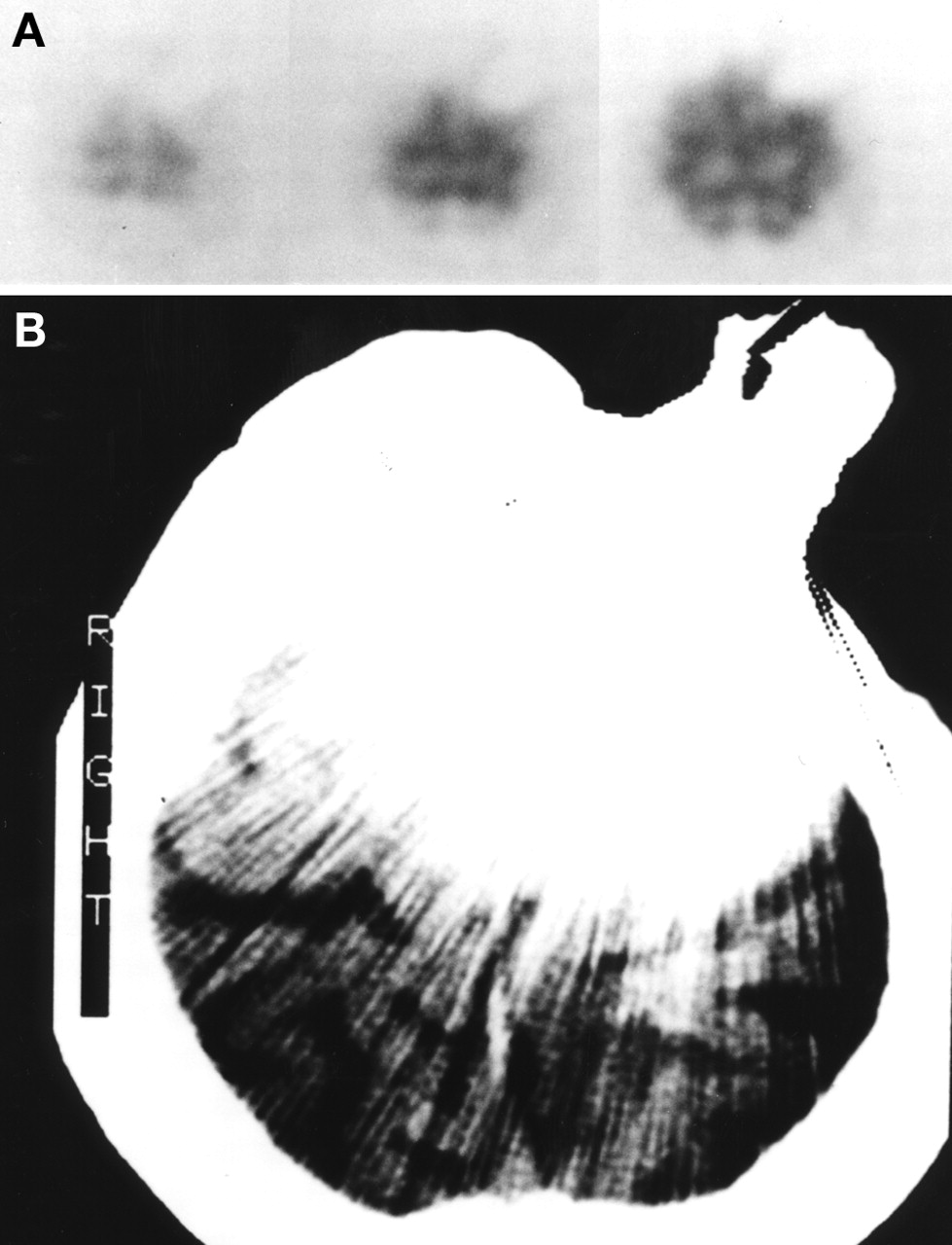
The patient brain SPECT transaxial images (Figs. 1A, 2A, 3A) showed a photon-deficient area underlying the metallic plate with increased tracer activity at its periphery that extended into the area of the scalp. Patient CT studies (Figs. 1B, 2B, 3B) showed significant streak artifact caused by the metallic plate.
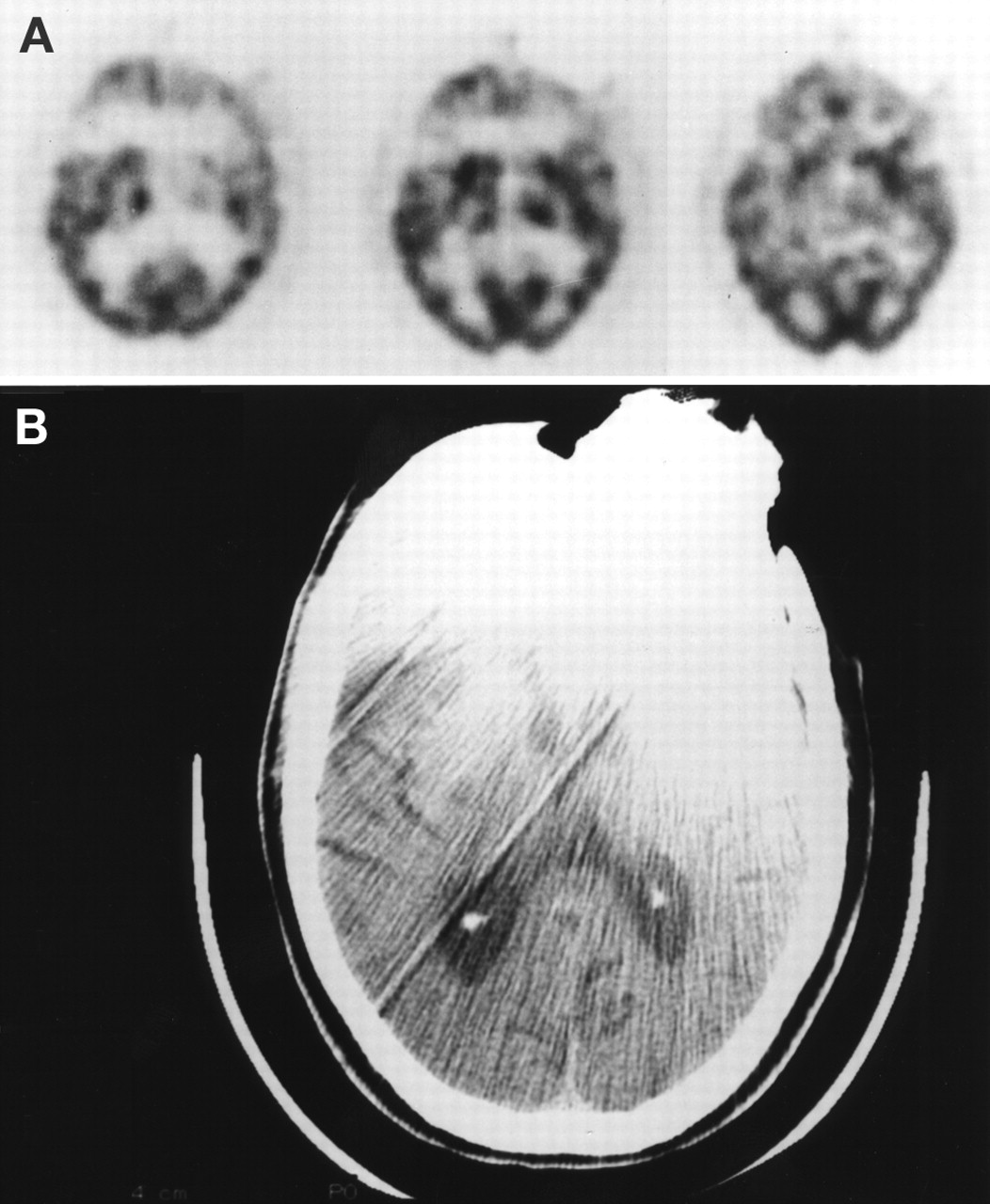
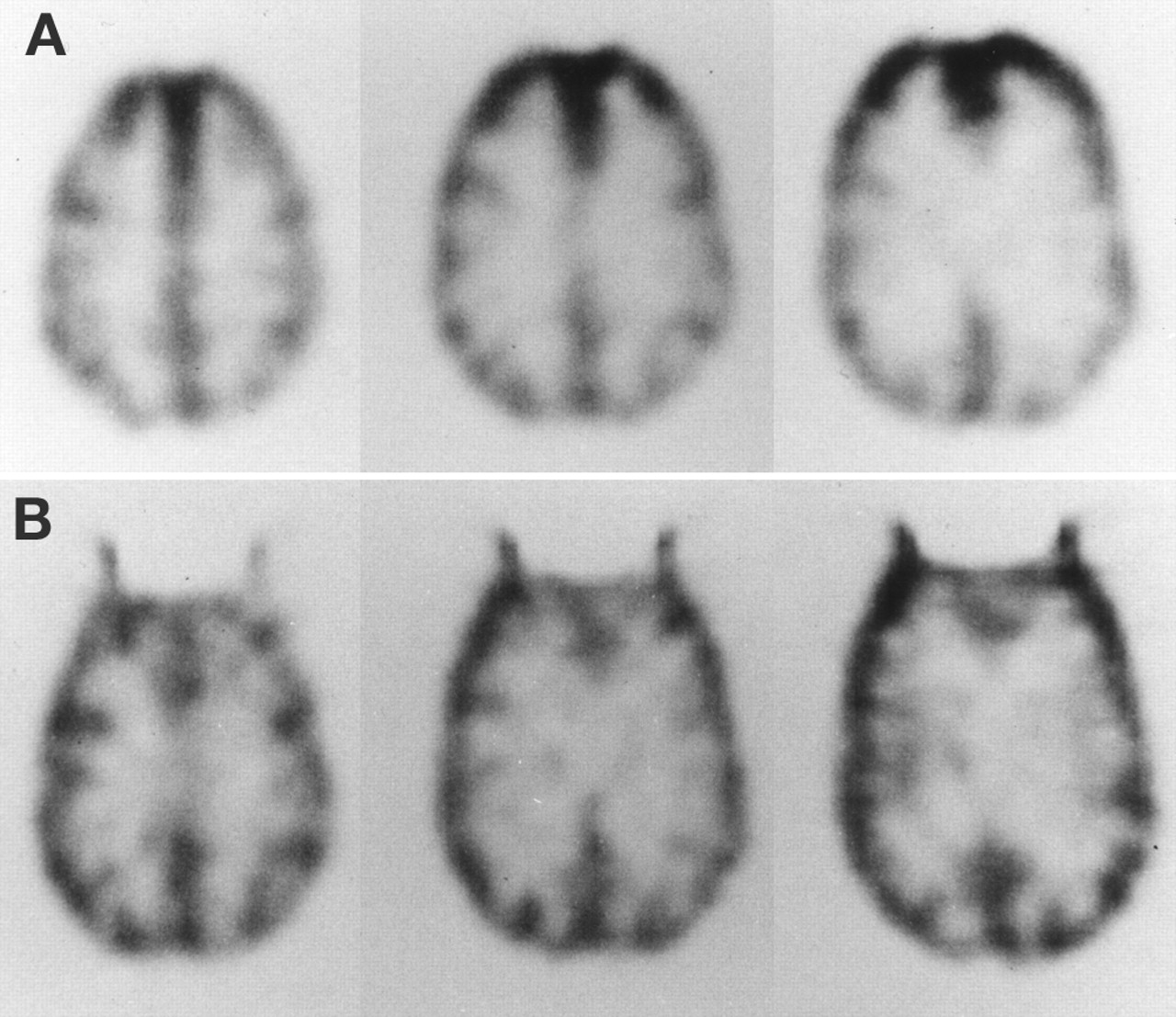
Transaxial images were visually compared for each SPECT brain phantom study. The studies that had either the aluminum or stainless steel sheets demonstrated no discernible photon-deficient areas and were comparable to the phantom study without any metallic sheets (Fig. 4A). The phantom studies with the lead sheet in place (Fig. 4B) demonstrated a photon-deficient area in the phantom underlying the area where the lead sheet was placed. There was also an increased tracer activity artifact at the periphery of the photon-deficient area that extended into the area where the scalp would be.
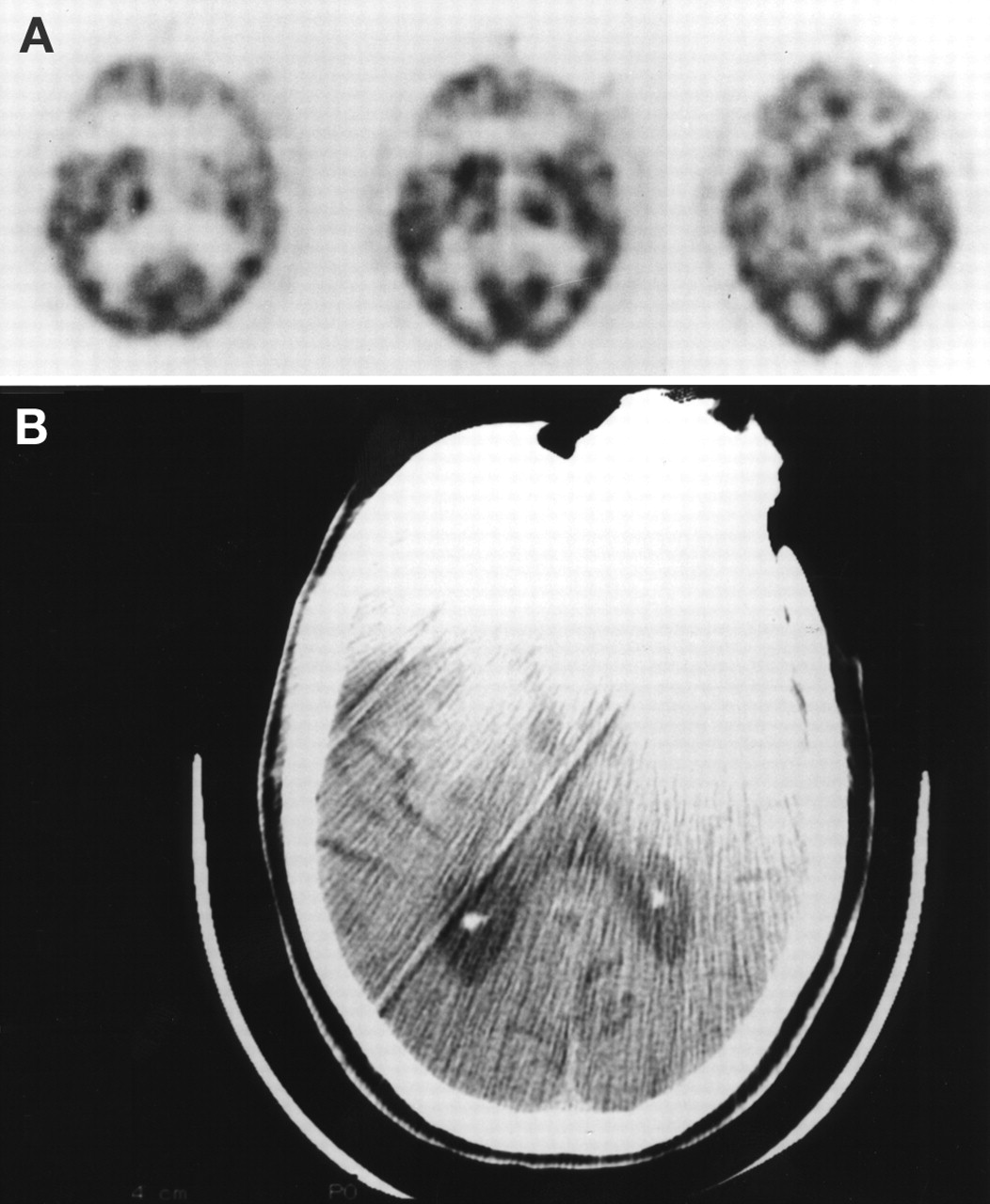
Patient 1, with head trauma in the 1940s that required a metallic plate in the left frontal area. (A) Transaxial images from brain SPECT study show photon-deficient area in the left frontal region with faint increased tracer activity extending into scalp area at periphery. (B) CT shows significant streak artifact caused by the metallic plate.
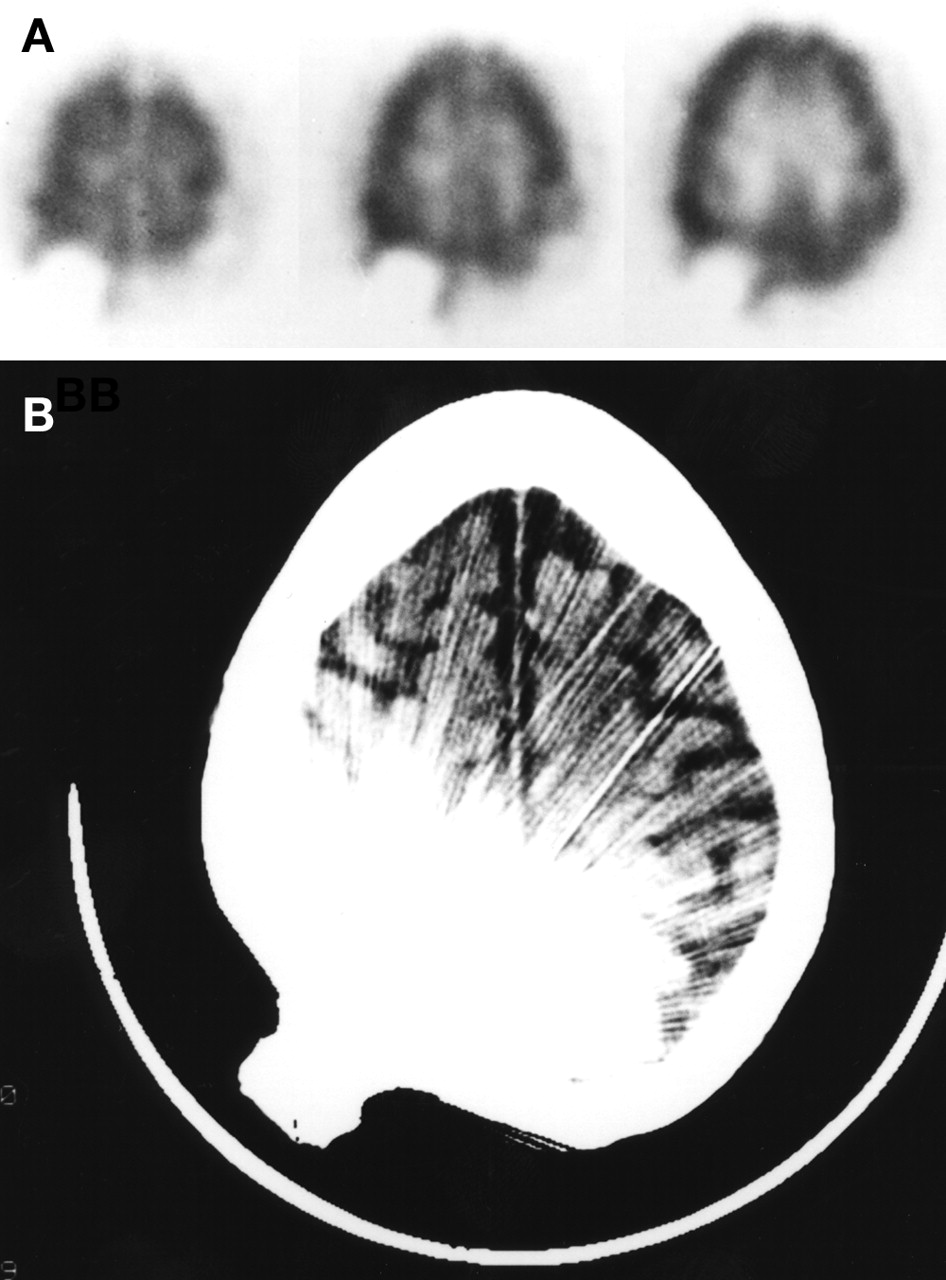
Patient 2, with head trauma in the 1970s that required a metallic plate in the right occipital area. (A) Transaxial images from brain SPECT study show photon-deficient area in the right occipital region with prominent increased tracer activity extending into scalp area at periphery. (B) CT shows significant streak artifact caused by the metallic plate.
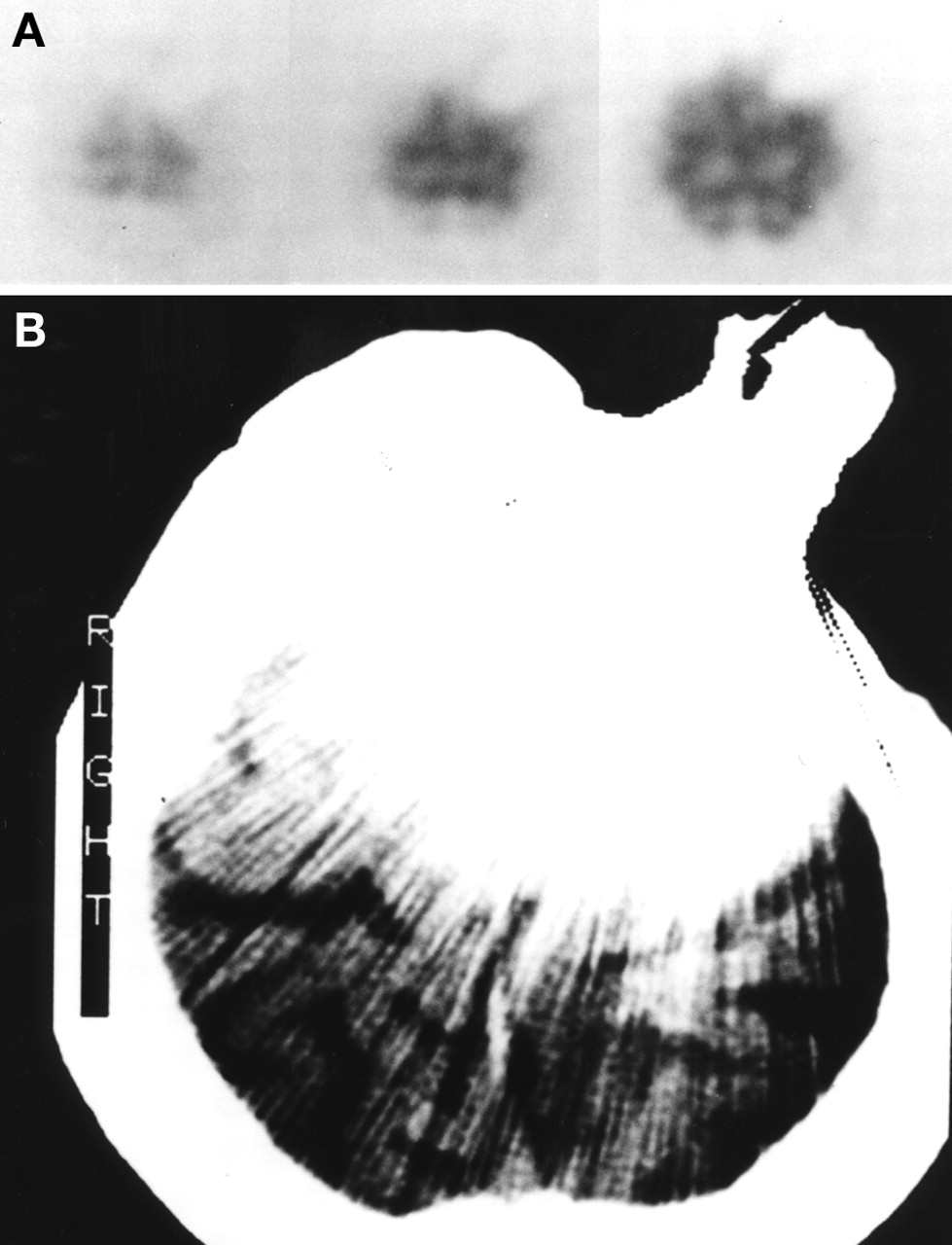
Patient 3, with head trauma in the 1940s that required a metallic plate in the left frontal area. (A) Transaxial images from brain SPECT study show photon-deficient area in the left frontal region with very faint increased tracer activity extending into scalp area at periphery. (B) CT shows significant streak artifact caused by the metallic plate.

Transaxial images of SPECT brain phantom with no metallic sheets in place (A) and with 0.076-cm lead sheet placed over midline of the frontal region (B). The 0.038-cm lead sheet produced a similar artifact, though not as prominent.
Table 1 summarizes the calculated attenuation caused by the metallic sheets in the planar image.
DISCUSSION
The SPECT brain phantom studies with the lead sheets clearly showed a defined photon-deficient artifact. An area of increased tracer activity was also evident at the periphery of this photon-deficient artifact. This increased tracer activity is also an artifact because it extends beyond where any activity should be found. These artifacts are caused by photon attenuation by the metallic plate, which results in SPECT reconstruction errors. These artifact presentations are similar to our patient studies, though one cannot assume that the photon-deficient areas in the patients were solely a result of attenuation from the metallic plates because they have had head trauma to these areas. These studies still yielded clinical information of perfusion in other regions of the brain unaffected by the artifacts. A similar brain SPECT artifact caused by a metallic plate can be seen in the case presentation by Boren et al. (5,6). Although we cannot confirm that the patients we studied had tantalum plates, the surgical literature states that tantalum (1) plates are radiopaque, and contains reports of CT studies that are similar to our patients’ CT studies (Figs. 1B, 2B, 3B). The literature (1–3) also states that both aluminum and stainless steel plates are radiolucent, which was clearly evident in our phantom studies.
Common SPECT artifacts caused by camera problems (e.g., uniformity, center of rotation) and patient motion can be easily detected and avoided (7,8). Sometimes SPECT errors can be caused by a simple mistake by the technologist (i.e., multihead camera with a different type of collimator on one of the three heads) (9). Attenuation caused by body tissues or by external materials will cause SPECT artifacts (7,8,10–12). The degree of attenuation caused by a metallic plate will be directly related to the magnitude of the artifact it produces, which then can affect the quality of the SPECT study. A brain SPECT study performed on a patient with a radiopaque metallic plate will yield a clearly defined photon-deficient area extending from the brain tissue into soft tissue (scalp), with increased tracer activity at the periphery of the photon-deficient area. This increased tracer presentation in the area of the scalp that is limited to the periphery of the photon- deficient area can easily be distinguished from other soft-tissue tracer presentations that are more diffuse (i.e., poor radiopharmaceutical tagging, recent surgery).
CONCLUSION
As one would expect, certain metallic plates cause photon-deficient artifacts on brain SPECT studies. They also cause another artifact of increased tracer activity seen at the periphery of the photon-deficient area. Knowing the appearance of this type of artifact caused by radiopaque metallic plates in brain SPECT studies could be beneficial, especially in cases with poor patient history and lacking radiographic correlation.
Acknowledgments
This study was presented at the 44th Annual Meeting of the Society of Nuclear Medicine in San Antonio, Texas, in June 1997.
Footnotes
For correspondence contact: Michael T. Hackett, M.S., Radiation Safety Officer, Radiation Safety Office/Nuclear Medicine Service (115-CDD), Department of Veterans Affairs Medical Center, 2250 Leestown Road, Lexington, KY 40511-1093; Phone: 859-381-5929; Fax: 859-381-5934; E-mail: michael.hackett{at}med.va.gov.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.