


Abstract
Our rationale was to evaluate the role of 99mTc-methylene diphosphonate (99mTc-MDP) SPECT/CT for the detection of sacroiliitis in spondyloarthropathies by comparing it with clinical markers and MRI findings. Methods: We prospectively included 155 patients (83 men and 72 women; mean age, 35.80 ± 12.40 y; range, 18–60 y) diagnosed with spondyloarthropathies as per the criteria of the European Spondyloarthropathy Study Group. All patients underwent clinical evaluation (using the Bath ankylosing spondylitis disease activity index [BASDAI]), measurement of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level, planar 99mTc-MDP bone scintigraphy, SPECT/CT, and MRI of the pelvic region. Using MRI as the reference criterion, the diagnostic accuracy of the clinical and scintigraphic parameters was assessed. On planar bone scintigraphy and SPECT, a score of 0, 1, or 2 was assigned when tracer uptake in the sacroiliac joint was less than, equal to, or more than that in the sacrum. A score of 2 was considered positive for the diagnosis of sacroiliitis. Results: The sensitivity, specificity, accuracy, and positive and negative predictive values of 99mTc-MDP SPECT/CT were 90.0%, 80.0%, 87.0%, 92.0%, and 75.0%, respectively. The accuracy of SPECT/CT (87%) was better than that of ESR (58.1%), CRP (32.9%), BASDAI scoring (77%), and planar bone scintigraphy (53%). Similar results were found for sensitivity and negative predictive value. Regarding specificity, SPECT/CT (80%) was lower than BASDAI scoring (88.6%) and equal to planar bone scintigraphy (80%). Regarding positive predictive value, SPECT/CT (92%) was a bit lower than BASDAI scoring (93.6%). κ-values for planar 99mTc-MDP bone scanning and SPECT/CT were 0.167 and 0.673, respectively, indicating poor agreement for planar bone scanning and good agreement for SPECT/CT. A significant (P < 0.001) correlation (r = 0.659) was observed between SPECT/CT and MRI findings. Conclusion: 99mTc-MDP SPECT/CT has diagnostic accuracy comparable to that of MRI for the evaluation of sacroiliitis in spondyloarthropathies and can thus be used as an alternative when MRI is contraindicated. SPECT/CT shows better accuracy than planar bone scintigraphy, ESR, CRP, and BASDAI scoring in the diagnosis of sacroiliitis.
Spondyloarthropathies are characterized by seronegative and inflammatory arthritis generally involving the spine and presenting clinically as peripheral arthritis and enthesitis. The spectrum of spondyloarthropathies includes ankylosing spondylitis (AS), psoriatic arthritis, enteropathic spondyloarthropathies, reactive arthritis, and undifferentiated spondyloarthropathy. The prevalence of spondyloarthropathies in India is estimated to be between 0.1% and 0.4%, and that of AS is about 0.2% (1–4). AS, the prototype of spondyloarthropathies, is one of the most common inflammatory rheumatic diseases (5,6). In early AS and undifferentiated spondyloarthropathy, sacroiliitis is an early clinical finding and is generally presumed to be the first manifestation of the disease (7). The current criteria for classification of spondyloarthropathies are the European Spondyloarthropathy Study Group criteria and the Amor criteria, and the current criteria for the classification of AS are the modified New York criteria (8–10).
Disease classification based on the AS criteria depends on radiologic evidence of sacroiliitis. These criteria do not cover the early AS phase, because radiologic evidence often appears only late in the disease. This may cause a delay both in establishing the final diagnosis and in initiating early and appropriate treatment in AS patients (11). The diagnosis of sacroiliitis using more sensitive modalities such as MRI may reduce the time required to arrive at a final diagnosis of either AS or spondyloarthropathies (12,13). MRI is known to have higher sensitivity than plain radiography and other imaging modalities in detecting sacroiliitis (14–16). However, because of some inherent technical limitations and contraindications, it is not always possible to use MRI in the routine diagnosis of sacroiliitis (17).
Planar 99mTc-methylene diphosphonate (99mTc-MDP) bone scintigraphy has been extensively used in diagnosis of sacroiliitis (14,15). SPECT/CT allows 3-dimensional localization of tracer activity to the sacroiliac joints. Limited studies in a few patients have shown that SPECT/CT bone imaging may be useful for identifying sacroiliitis in spondyloarthropathy patients and thus may provide an alternative to MRI (14,18,19). In the present study, we compared the diagnostic utility of SPECT/CT with that of MRI for the detection of sacroiliitis in spondyloarthropathies in a large cohort.
MATERIALS AND METHODS
In total, 155 consecutively diagnosed patients with spondyloarthropathies (83 men and 72 women; age range, 18–60 y; mean, 35.8 ± 12.40 y) were prospectively included in the study, which was approved by the ethics committee of our institute. All recruited patients met the criteria of the European Spondyloarthropathy Study Group, having characteristic clinical symptoms consisting of an insidious onset of inflammatory back pain for more than 3 mo, with morning stiffness subsequently improving on exercise. Patients who had radiographic evidence of grade 2 sacroiliitis; had a history of Brucella, tuberculosis, septic sacroiliitis, endocrine/metabolic diseases, or any malignancy; or were pregnant were excluded from the study. Each patient underwent a functional clinical examination (using the Bath ankylosing spondylitis disease activity index [BASDAI]); measurement of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels; and imaging with 99mTc-MDP bone scintigraphy, SPECT/CT, and MRI of the sacroiliac joints.
99mTc-MDP Bone Scanning (Planar and SPECT/CT)
Anterior and posterior whole-body images were acquired 3 h after approximately 740.0 MBq of freshly prepared 99mTc-MDP had been intravenously injected. The images were acquired in a 256 × 1,024 matrix at a speed of 14 cm/min, using a double-head SPECT/CT γ-camera equipped with a low-energy, high-resolution collimator (Infinia Hawkeye 4; GE Healthcare).
Immediately after completion of the whole-body acquisition, SPECT images of the pelvic region were acquired in a 64 × 64 matrix using the step-and-shoot method, covering a 360° circular orbit in 60 projections (30 s/projection). After the SPECT acquisition, a nondiagnostic CT scan of the pelvic region was acquired in helical mode with a tube current of 2.5 mA. The SPECT/CT data were reconstructed using an iterative algorithm (ordered-subsets expectation maximization; 2 iterations and 10 subsets) by applying a Hann filter (cutoff frequency, 0.9) using the Volumetrix Protocol on a Xeleris 2 workstation (version 2006; GE Healthcare). Subsequently, the reconstructed data were displayed for visual interpretation of tracer uptake in the sacroiliac joints.
For visual scoring, a score of 0 was assigned when tracer uptake in the sacroiliac joint was less than that in the sacrum; a score of 1, when equal to that in the sacrum; and a score of 2, when greater than that in the sacrum. A score of 2 was considered positive for the diagnosis of sacroiliitis on planar bone scanning and SPECT/CT. Planar bone scintigraphy and SPECT images were scored independently by 2 experienced nuclear physicians. In cases of discrepancy, a consensus was reached by discussion. The accuracy of planar and SPECT/CT techniques in the detection of sacroiliitis in spondyloarthropathies was compared with that of MRI as the criterion standard.
MRI
MRI was performed using 3.0-T (Verio; Siemens) or 1.5-T (Aera; Siemens) whole-body MR units equipped with a standard head coil. The axial images had a field of view of 350 mm with a 4-mm slice thickness to show the whole paravertebral area. The axial and coronal T1-weighted images (repetition time, 600 ms; echo time, 15 ms) were acquired after gadolinium–diethylenetriaminepentaacetic acid (0.05 mol/kg) contrast administration. A matrix of 224 × 256 was used for the axial images. MRI findings were analyzed independently by an experienced radiologist. Sacroiliitis was diagnosed if MRI showed any one of the following features: a loss of normal uniform cartilage signal intensity; bone marrow edema and synovial enhancement; or an increase in signal intensity in the joint, erosions, sclerosis, and ankylosis (chronic sacroiliitis).
Clinical Markers
ESR (Westergren) and CRP (ELISA with ELISA plate reader) levels were used to assess inflammation. Biochemical evidence of disease activity was defined by the presence of a high ESR level (>20 mm/h; reference range, 0–20 mm/h) and a high CRP level (>5 mg/L; reference range, 0–5 mg/L). The disease activity was assessed using a standard questionnaire based on BASDAI scoring, in which a score of 3.9 or less denotes no active disease, a score of 4–6.9 denotes ambiguity about the presence of disease activity, and a score of 7.0 or more denotes definitive disease activity.
The 3 imaging procedures were performed within 2 wk after the clinical assessment. All patients gave written informed consent to participate in the study.
Statistical Analysis
Statistical analysis was done using SPSS software for Windows (version 17.0; SPSS, Inc.). Data were represented in the form of tables and bar diagrams. Sensitivity, specificity, accuracy, and positive and negative predictive values were calculated using MRI as the reference standard. Agreement between planar 99mTc-MDP bone scanning, SPECT/CT, and MRI was tested using κ-statistics. Correlation with MRI findings was done using inflammatory markers (ESR, CRP) and functional assessment of disease activity by the BASDAI criteria. κ-values lower than 0.4, between 0.4 and 0.75, and greater than 0.75 were considered to represent poor, fair to good, and excellent agreement, respectively. Statistical significance for all analyses was assessed at a P value of less than 0.05.
RESULTS
The demographic details of the patients—that is, age, disease duration, pain scoring (based on the BASDAI criteria), and the results of the laboratory investigations (ESR and CRP)—are presented in Table 1. The results are presented as mean, median, and range. The mean age was 35.8 ± 12.4 y, and the mean disease duration was 14.2 ± 19.5 mo. The mean ESR (mm/h) and CRP values were 26.6 ± 17.5 and 15.3 ± 10.2, respectively. The mean BASDAI score was 2.9 ± 1.9.
Clinical and Laboratory Findings
We found that 62.0% (95/155) of the patients had AS, 33.0% (50/155) had undifferentiated spondyloarthropathy, and 3.8% (7/155) had reactive arthritis. The remaining 1.2% (3/155) had psoriatic arthritis. Of the 155 patients, 104 had HLA-B27–positive results. MRI was positive for sacroiliitis in 111 patients and negative for sacroiliitis in 44 patients. The findings were suggestive of acute or active sacroiliitis in 83 patients (20 unilateral, 63 bilateral) and chronic sacroiliitis in 28 patients. Planar 99mTc-MDP bone scan findings were positive for sacroiliitis in 54 patients and negative in 101 patients. On the other hand, SPECT/CT findings were positive for sacroiliitis in 108 patients and negative in 47 patients.
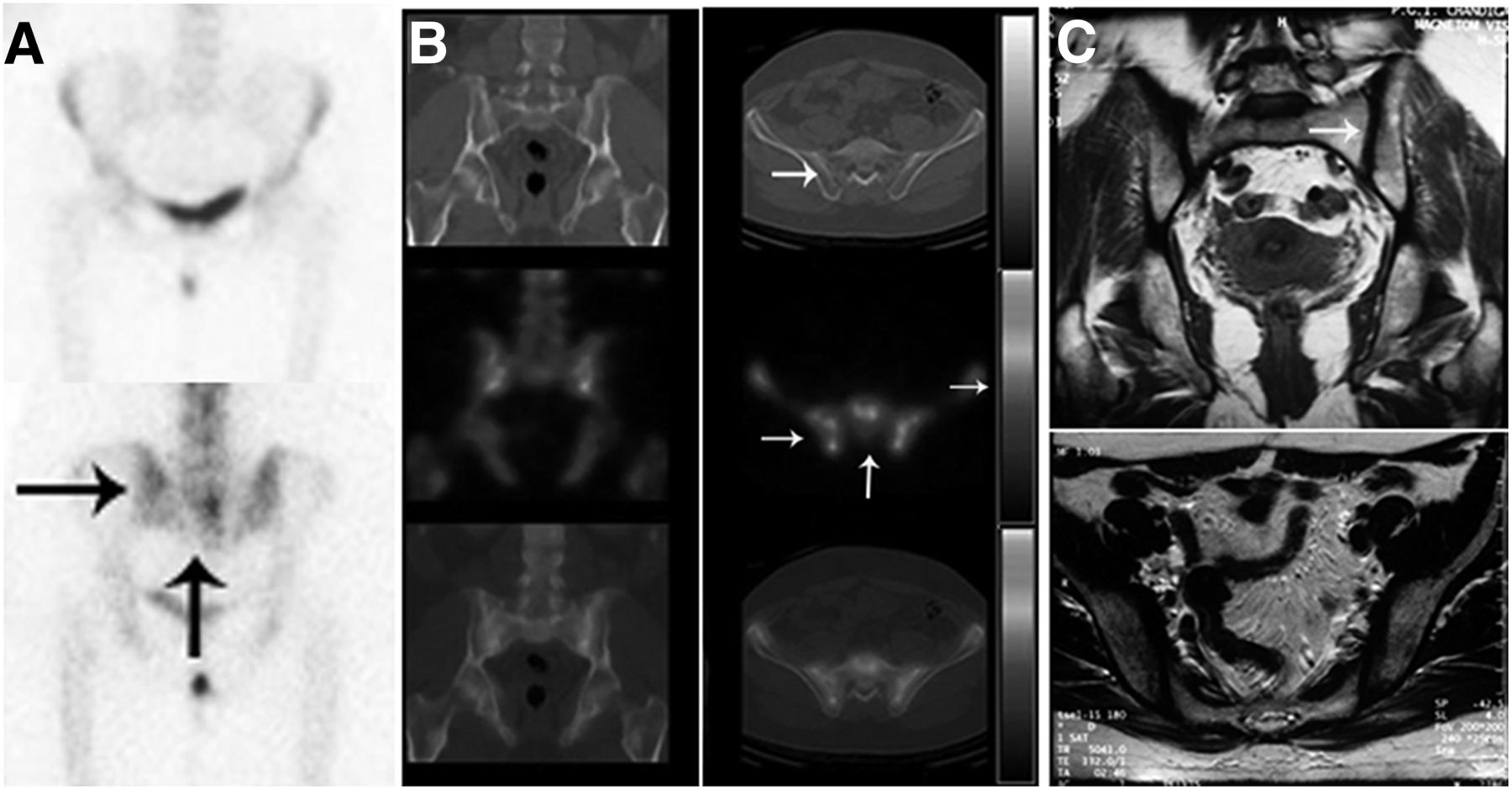
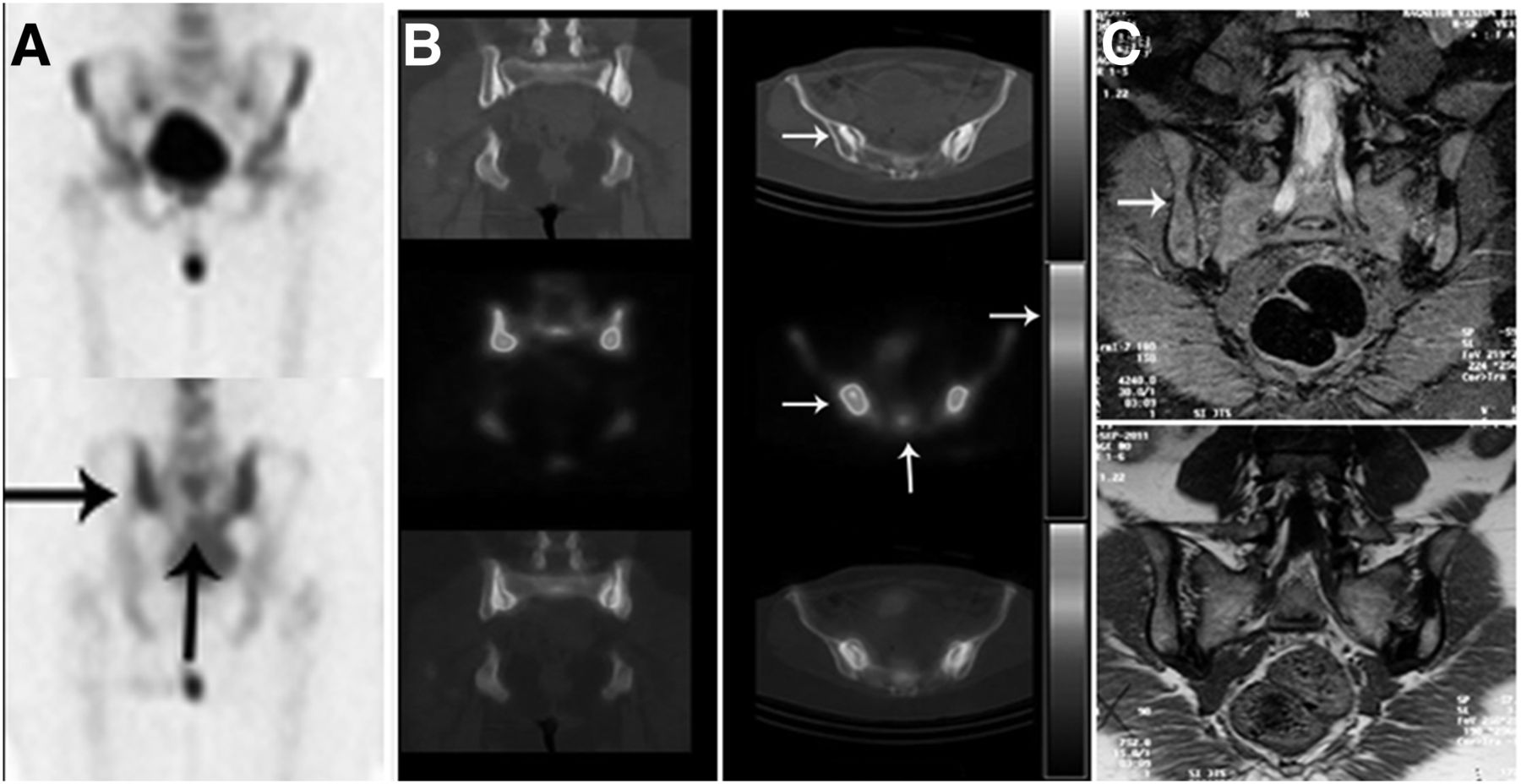
Figure 1 shows negative findings for sacroiliitis on planar bone scanning (A), SPECT/CT (B), and MRI (C), with a score of 1 on both planar imaging (anterior and posterior images) and SPECT/CT. Figure 2 presents findings positive for bilateral sacroiliitis on SPECT/CT (B) and MRI (C), with a score of 2 on SPECT/CT due to accurate localization of tracer activity in the sacrum and sacroiliac joints. The planar bone scan (A) showed tracer uptake equally in the sacrum and sacroiliac joints.
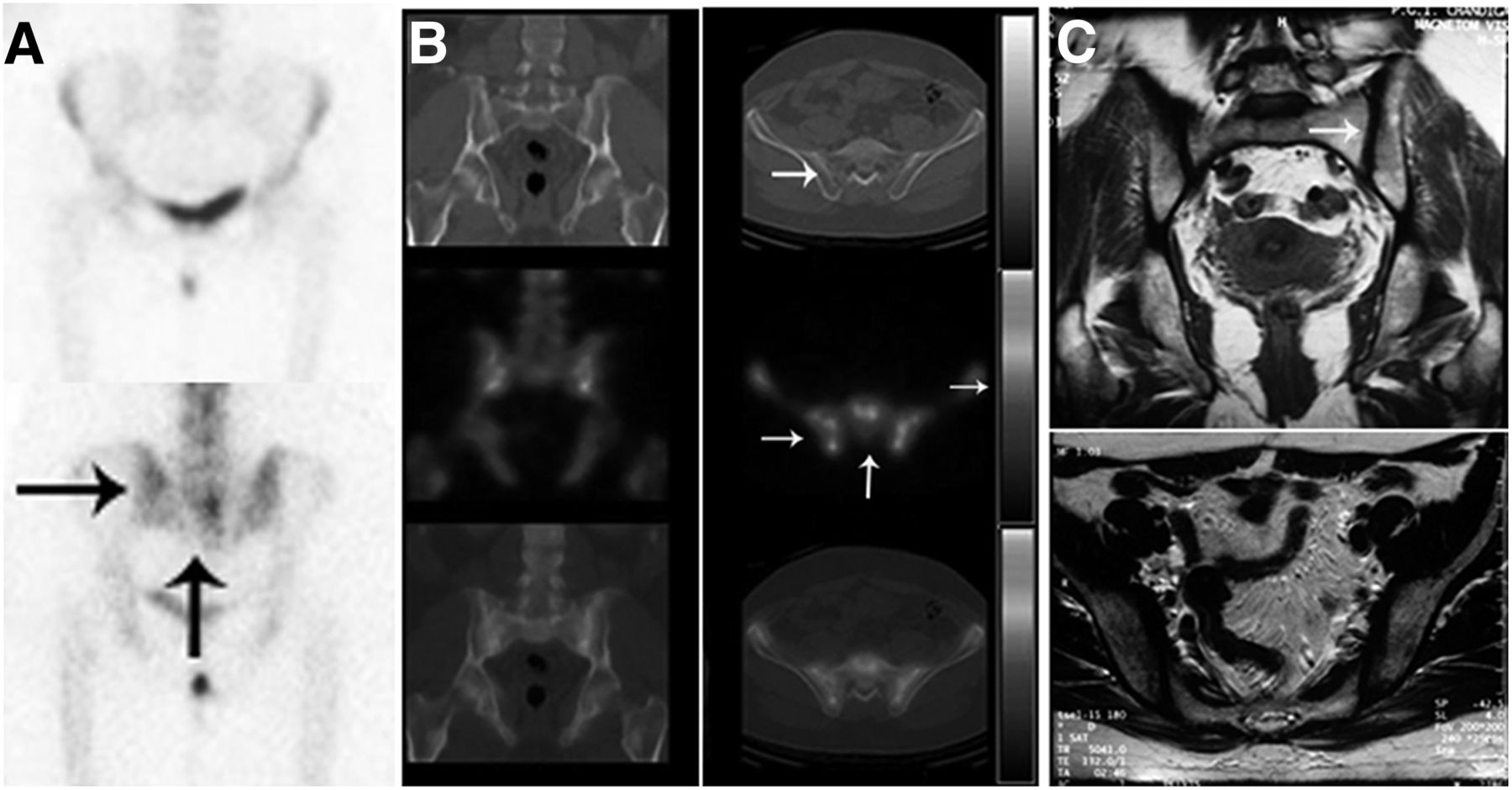
Three imaging modalities showing no sacroiliitis in 25-y-old man with 6-mo history of lower backache. (A) Anterior and posterior whole-body planar 99mTc-MDP bone scanning demonstrates equal tracer uptake (arrows) in sacrum and sacroiliac joints. (B) Hybrid SPECT/CT of pelvic region shows equal tracer uptake (arrows, middle) in sacrum and sacroiliac joints and no abnormal CT finding (arrow, top). (C) MR images of left and right sacroiliac joints also show no features of sacroiliitis.

Hybrid SPECT/CT and MR showing bilateral sacroiliitis, with normal findings on planar bone scanning, in 47-y-old male AS patient with 10-mo history of lower backache. (A) Anterior and posterior whole-body planar 99mTc-MDP bone scanning indicates symmetric tracer uptake (arrows) in sacrum and sacroiliac joints (negative for sacroiliitis). (B) Hybrid SPECT/CT shows increased tracer uptake (arrows) localized in and around both sacroiliac joints as compared with sacrum (suggestive of bilateral sacroiliitis), similar to MRI findings (arrow). (C) MRI shows bilateral sacroiliitis (arrow).
The comparative diagnostic utility of the clinical markers and imaging techniques is presented in Table 2. Planar 99mTc-MDP bone scanning demonstrated a low sensitivity (42.0%), accuracy (53.0%), and negative predictive value (36.0%) for the diagnosis of sacroiliitis. In comparison, SPECT/CT offered higher values of 90.0%, 87.0% and 75.0%, respectively. Likewise, the positive predictive value for SPECT/CT was higher (92.0%) than that for planar bone scanning (85.0%). The two techniques, however, demonstrated a similar specificity of 80.0%.
Sensitivity, Specificity, Accuracy, and Positive and Negative Predictive Values Using MRI as Reference Standard
Agreement between each modality and the reference standard, MRI, was tested using κ-statistics. The κ-values for planar 99mTc-MDP bone scanning and SPECT/CT were 0.167 and 0.673, respectively, indicating poor agreement for planar bone scanning and good agreement for SPECT/CT. Pearson correlation coefficient analysis demonstrated a good correlation (r = 0.659; P < 0.001) between SPECT/CT and MRI. The accuracy of SPECT/CT (87%) was better than that of ESR (58.1%), CRP (32.9%), BASDAI scoring (77%), and planar bone scintigraphy (53%). Similar results were found for sensitivity and negative predictive value. The specificity of SPECT/CT (80%) was lower than that of BASDAI scoring (88.6%) and equal to that of planar bone scintigraphy (80%). The positive predictive value of SPECT/CT (92%) was a bit lower than that of BASDAI scoring (93.6%)
DISCUSSION
Inflammatory involvement of the sacroiliac joints is an important criterion for establishing the diagnosis of spondyloarthropathies (7), which occur most commonly in young patients. An early diagnosis is critical for initiating appropriate treatment in these patients and for increasing their productivity. Plain radiography has always been a part of the diagnostic work-up and the classification criteria for spondyloarthropathies. However, radiographic evidence of sacroiliitis usually does not become apparent until a few years after the symptomatic onset of the disease (11). MRI has been found to be superior to other imaging techniques for the accurate detection of early cartilaginous changes and bony erosions (14,19). MRI is contraindicated in patients with claustrophobia, pacemakers, and metal implants. These patients may require an alternative imaging technique for the diagnosis of sacroiliitis.
In the present study, we found that the BASDAI test demonstrated low sensitivity (69.4%) and accuracy (77.0%) for the detection of sacroiliitis. These results agree with those of previous investigators, who found no significant association between MRI findings and BASDAI results (20). Likewise, we observed that the levels of acute-phase reactants also exhibited low sensitivity and accuracy, at 52.0% and 58.1%, respectively, for ESR and 17.1% and 32.9%, respectively, for CRP. The role of ESR and CRP in the diagnosis of sacroiliitis remains controversial (21). Interobserver variations in the grading of sacroiliac radiographs have been reported (22,23).
Many studies have compared the diagnostic utility of planar or SPECT bone scanning with that of plain radiography, CT, and MRI. However, to the best of our knowledge, no previous study has compared the role of hybrid imaging (i.e., SPECT/CT) with that of MRI. Our study compared clinical markers, planar imaging, bone SPECT/CT, and MRI for the diagnosis of sacroiliitis in a cohort of 155 patients having spondyloarthropathies. The low-dose nondiagnostic CT done as part of SPECT/CT was used for localization of the tracer activity only. Statistical analysis of the scan results shows that SPECT/CT has higher sensitivity, diagnostic accuracy, and positive predictive value than planar bone scanning.
It has been reported previously that the pooled sensitivity of planar bone scanning, in comparison with the reference standard, MRI, in the detection of sacroiliitis in AS was 59.5% (24,25). Contrast-enhanced MRI has been reported to be superior to quantitative sacroiliac scintigraphy and conventional radiography in detecting early sacroiliitis. However, its specificity is limited by previous inflammatory episodes (15). The observed variation in the sensitivity of planar bone scanning for detecting sacroiliitis is attributed to factors such as sex, ethnicity, past history of drug therapy, imaging time, urinary bladder activity, past history of trauma or fracture, patient movement, injection site, and the region of interest selected for quantitative studies (26). In the present study, we found that planar bone scanning had a sensitivity of only 42.0%, compared with 90.0% for SPECT/CT.
Hanly et al. observed that 99mTc-MDP SPECT exhibited higher sensitivity than planar scintigraphy (27); the investigators subsequently reported that MRI was the most sensitive technique, and SPECT the most specific, for detection of sacroiliitis (28). These authors highlighted the fact that SPECT alone does not identify the cause of inflammatory disease or the characteristics of sacroiliitis. Therefore, SPECT/CT of the pelvic region may overcome the technical limitations of both planar bone scintigraphy and SPECT alone in the evaluation of sacroiliitis. The use of SPECT of the pelvic region provides 3-dimensional imaging of the distribution of radioactivity in and around the sacroiliac joint. The SPECT/CT image helps identify the location of the tracer in the sacrum and the iliac bones forming the sacroiliac joint (Fig. 2B). If diagnostic CT is done as a part of SPECT/CT, one can note erosions and subchondral sclerosis, joint space alterations, and new bone formation, which can play a complementary role in making the final diagnosis of sacroiliitis.
In the present study, SPECT/CT imaging significantly improved the sensitivity of planar bone scanning in the detection of sacroiliitis in spondyloarthropathies. When 99mTc-MDP bone scanning is combined with SPECT/CT, sacroiliitis can be accurately detected in seronegative spondyloarthropathy patients, with diagnostic accuracy comparable to that of MRI, the criterion standard.
Regarding limitations of this study, nondiagnostic CT was done as a part of the SPECT/CT study to localize the tracer activity. The fact that the incremental value of CT changes was not evaluated separately may lead to a higher accuracy for SPECT/CT.
CONCLUSION
99mTc-MDP SPECT/CT imaging has diagnostic accuracy comparable to that of MRI for the evaluation of sacroiliitis in spondyloarthropathies and can be used as an alternative when MRI is contraindicated. For diagnosis of sacroiliitis, SPECT/CT shows better accuracy than planar bone scintigraphy, ESR, CRP, and BASDAI scoring.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 10, 2017.
REFERENCES
- Received for publication April 1, 2017.
- Accepted for publication July 29, 2017.





{kind=link}
{kind=link}