


A 69-y-old man with a history of small cell lung cancer, esophageal cancer, and pulmonary hypertension stated that he had shortness of breath. The D-dimer level was elevated at 1,385.
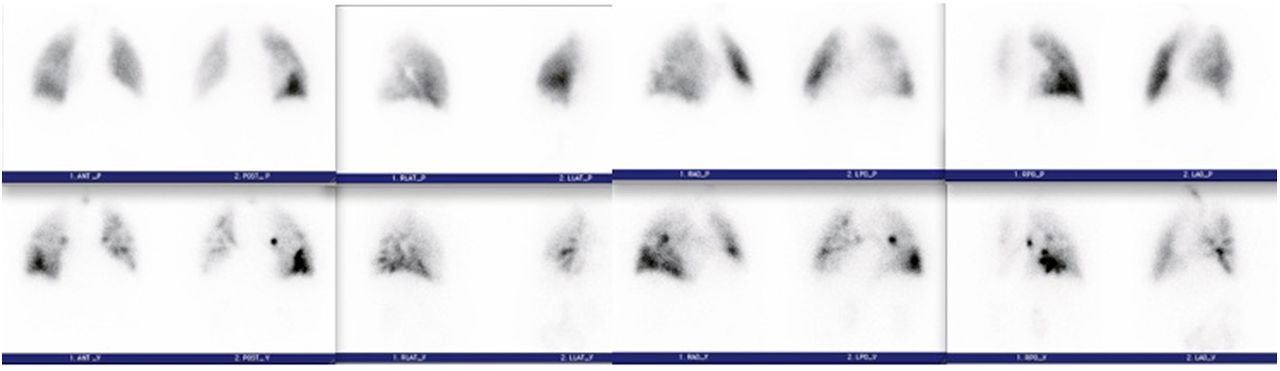
The patient inhaled a calculated 51.8 MBq (1.4 mCi) of 99mTc-diethylenetriminepentaacetic acid aerosol, after which planar images of the lungs in the standard 8 projections were obtained. After intravenous administration of 151.7 MBq (4.1 mCi) of 99mTc-labeled macroaggregated albumin (MAA), a set of projections corresponding to those obtained on the ventilation study was obtained (Fig. 1).

(Top) Perfusion images of lungs. Views from left to right are anterior/posterior, lateral, right anterior oblique/left posterior oblique, and left anterior oblique/right posterior oblique. (Bottom) Ventilation images in projections corresponding to perfusion images.
QUESTION 1
This patient has a history of pulmonary hypertension. What difference in the technique had to be addressed before the study was performed? Why?
Reduction of the number of 99mTc-MAA particles to less than 100,000 to lessen the likelihood of blockade of the capillaries.
Reduction of the 99mTc dose to decrease the radiation dose to the patient.
Completion of perfusion images first. If these are normal, the ventilation images do not need to be completed, thus decreasing the radiation dose to the patient.
Reduction of the number of 99mTc-MAA particles to 100,000–200,000 to lessen the likelihood of blockade of the capillaries.
QUESTION 2
After reviewing the lung scan images and comparing them to the chest radiograph (Fig. 2), what is your assessment of the findings based on the modified PIOPED II interpretation criteria (Table 1)?
High probability of pulmonary embolism, as there are 2 large segmental mismatched defects in the right lower lobe.
Nondiagnostic scan for pulmonary embolism, as there is 1 moderate segmental triple match in the superior segment of the right lower lobe.
Low probability of pulmonary embolism.
Nondiagnostic scan for pulmonary embolism, as there is 1 large segmental triple match in the superior segment of the right lower lobe, although more information would be valuable for an accurate interpretation.
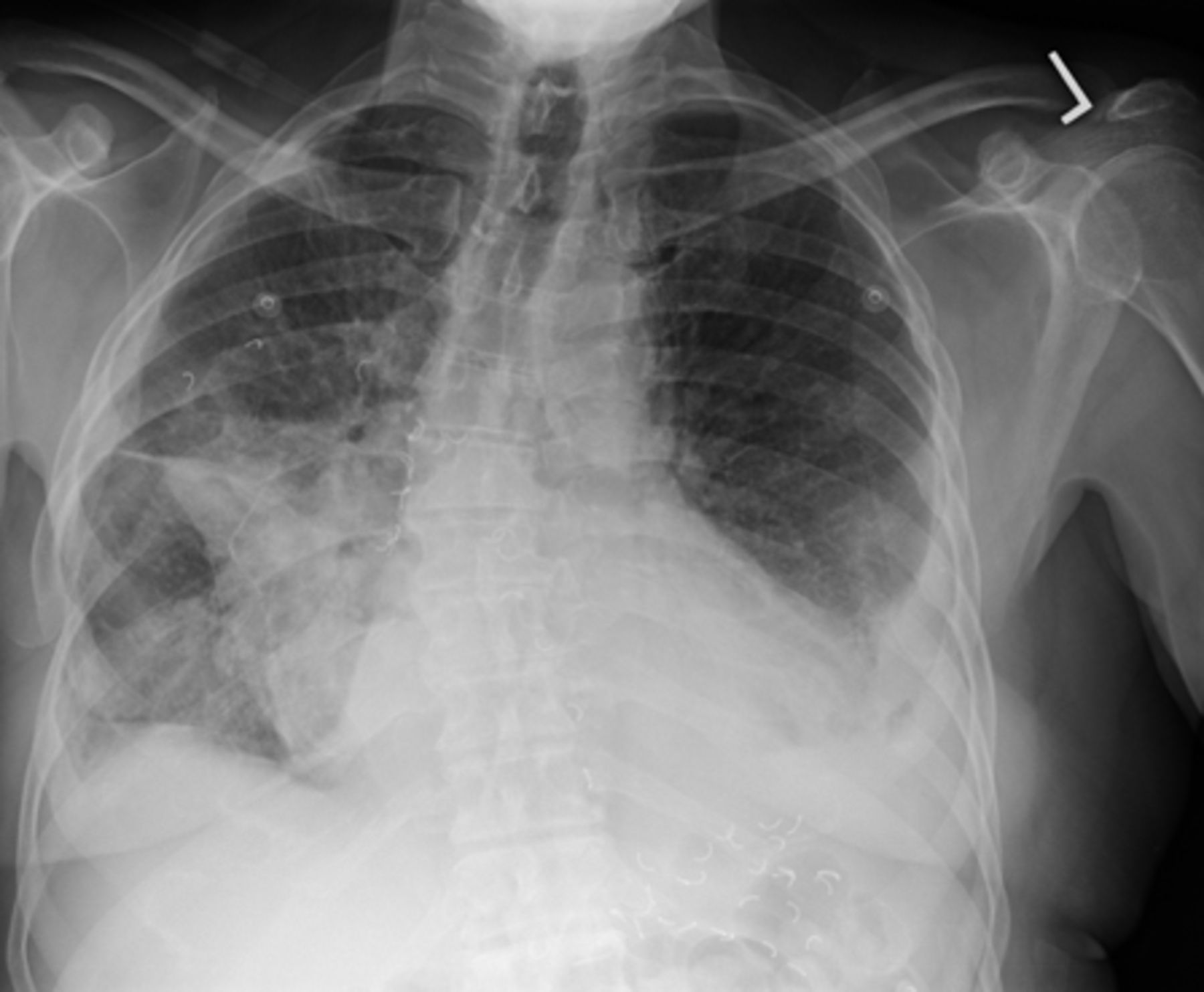
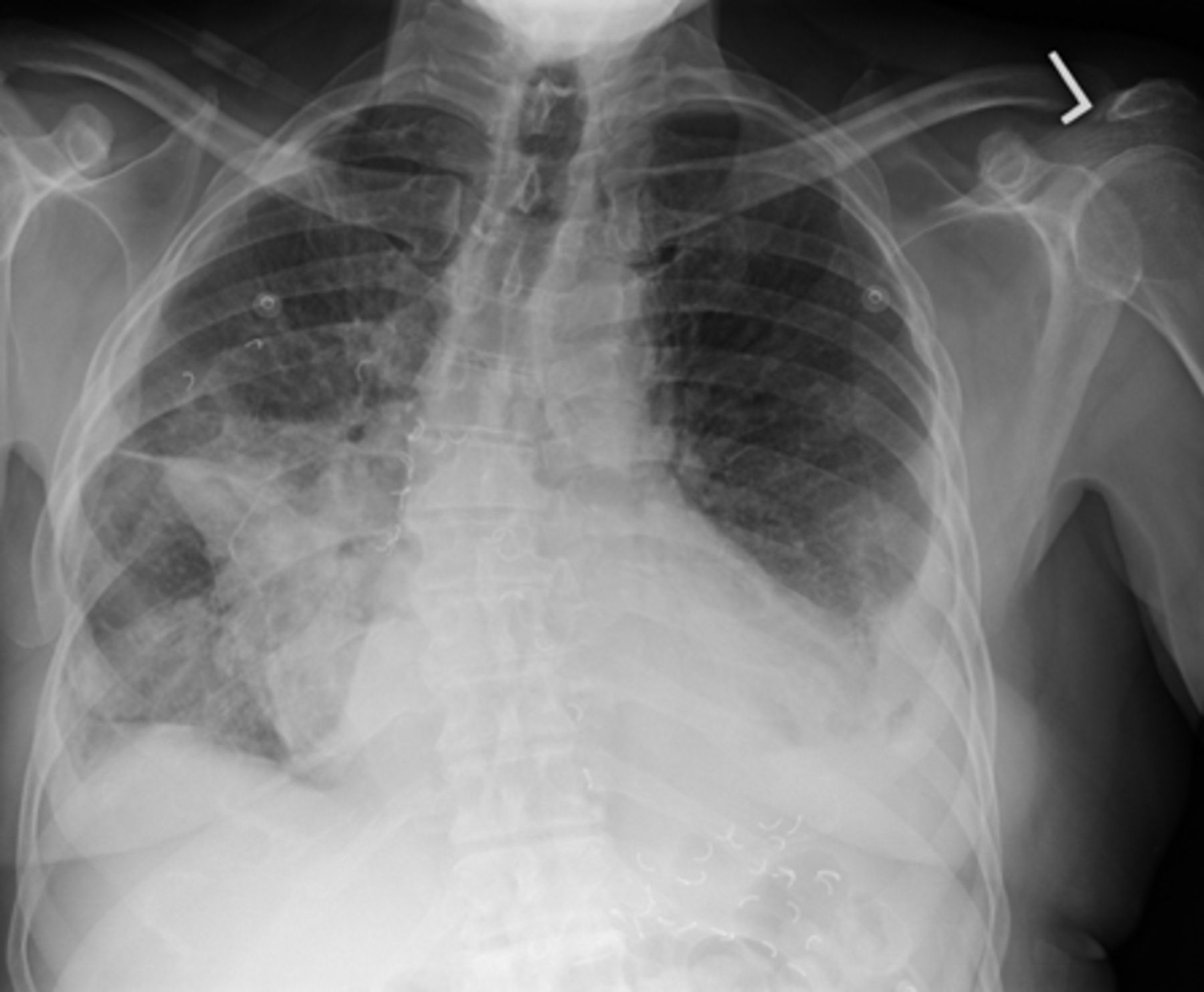
Chest posteroanterior radiograph that was completed approximately 12 h before lung scan.
Ventilation, Perfusion, and Radiographic Interpretive Criteria for Pulmonary Embolism
QUESTION 3
The patient also underwent CT of the chest with intravenous contrast material (Fig. 3) within the last week. Do the CT findings change your previous diagnosis?
No, the patient still has a high probability of pulmonary embolism.
No, the patient still has a nondiagnostic scan for pulmonary embolism.
The scan is technically nondiagnostic; however, it appears that the patient has postsurgical changes within the opaque region identified on the chest radiograph.
No, the patient still has a high probability for pulmonary embolism even though there are postsurgical changes within the opaque region identified on the chest radiograph.

Contrast-enhanced chest CT scan. (A) From left to right: 3 axial slices (lung window) from cranial to caudal. (B) Coronal slice (soft-tissue window) illustrating extent of gastric pull-through, which caused large defect on ventilation–perfusion images.
QUESTION 4
Besides lymph node involvement and distant metastatic disease, what additional information is needed for staging purposes?
The lymph node location is needed because lymph nodes above and below the diaphragm may change the stage of the disease.
The endoscopic ultrasonography and pathology report is needed because the extent of invasion of the cancer can change the stage of the disease.
Whether a lymph node is present in the supraclavicular regions needs to be known because the patient would be deemed a nonsurgical candidate.
The location of the distant metastatic disease is needed because this information may change the stage of the patient.
DISCUSSION
Knowing the entire history of a patient is important when reviewing studies, especially when the patient may have postsurgical changes that may interfere with one’s interpretation. Patients with benign and malignant disease of their esophagus may undergo radical resection and reconstruction with an intrathoracic stomach, colon, or jejunum pulled up through the mediastinum, retrosternally or subcutaneously. These postsurgical changes will appear as a widened mediastinum, usually on the right side. The history is important, as air-space disease, mass lesions, pleural effusion, or lobar collapse may look the same as one another on a chest radiograph. Knowing the history of our patient, we were able to relay this information to the referring physician and communicate that the mismatch was most likely due to the patient’s gastric pull-through and radiotracer activity located within the stomach. Strictly speaking, with the PIOPED criteria the patient would still remain at intermediate probability of pulmonary embolism because the corresponding ventilation–perfusion defects correlated with the parenchymal opacity seen in the lower lung zone on the chest radiograph. The PIOPED criteria look only at comparing the lung scan to the chest radiograph and not any other helpful imaging, such as the CT scan of the chest.
Footnotes
Published online Jul. 18, 2013.
↵* For the answers, see page 242.





{kind=link}
{kind=link}
{kind=link}