


Abstract
123I-labeled 2β-carbomethoxy-3β-(4-iodophenyl)-N-(3-fluoropropyl)nortropane (123I-FP-CIT) was approved for clinical use in 2011 by the Food and Drug Administration. 123I-FP-CIT is a radioligand for brain dopamine transporter (DAT) imaging that is useful for the differential diagnosis of Parkinson disease (PD) and other diseases that mimic PD. The sensitivity and specificity of 123I-FP-CIT SPECT for PD diagnosis are more than 90% and equivalent to those of other DAT SPECT methods. In the near future, the clinical indications of DAT imaging are expected to be broadened; for example, including treatment response assessment, disease progression monitoring, and early diagnosis of premotor PD in each individual patient.
Parkinson disease (PD) is the second most common neurodegenerative disorder after Alzheimer dementia (1). Studies suggest that PD affects at least 500,000 people in the United States (2), and 1%–2% of people over 65 y old have PD (3). Approximately 50,000 new cases are diagnosed each year (4). The financial and public health impact of this disease is expected to increase as the average age of the population increases (2).
The classic motor symptoms of PD are tremor of a limb, rigid limbs, slow movement, and balance problems. The tremor often begins insidiously on one side of the body and spreads to the other side with a slowly deteriorating course (5,6). These symptoms are attributed mostly to dopamine deficit, secondary to progressive loss of dopamine-secreting neurons projecting from the substantia nigra to the striatum (7,8). Dopamine is a neurotransmitter that regulates movement, and therefore the lack of dopamine produces abnormal movement. The dopamine transporter (DAT) controls the intensity and duration of dopaminergic neurotransmission by rapid reuptake of dopamine into presynaptic terminals (9–11). DAT density correlates with the density of dopaminergic neurons and is used as an imaging biomarker for diagnosing PD.
A NEW ERA OF CLINICAL DOPAMINE TRANSPORTER IMAGING USING 123I-LABELED 2ς-CARBOMETHOXY-3ς-(4-IODOPHENYL)-N-(3-FLUOROPROPYL)NORTROPANE (123I-FP-CIT)
The Food and Drug Administration (FDA) approved the clinical use of 123I-FP-CIT (international nonproprietary name ioflupane, brand name DaTSCAN [GE Healthcare]) in January 2011 (12). 123I-FP-CIT is indicated for the visualization of the presynaptic DAT distribution within the striatum by SPECT in patients with suspected Parkinsonian syndromes. Striatal uptake of 123I-FP-CIT is reduced in patients with PD, which is a motor system disorder resulting from dopaminergic neurodegeneration.
DAT DENSITY AND 123I-FP-CIT UPTAKE
DAT is a sodium chloride–dependent transmembrane protein on the presynaptic dopaminergic nerve terminal that controls dopamine levels by active reuptake of dopamine from the synaptic cleft after its interaction with the postsynaptic receptor (11,13). Striatal 123I-FP-CIT uptake is correlated with DAT density (14). With dopaminergic neurodegeneration, DAT density decreases and therefore striatal 123I-FP-CIT uptake is reduced on DAT imaging.
WHY DO WE IMAGE STRIATAL DAT DENSITY?
Why do we image DAT density in the striatum when the major pathology of PD is in the neurodegeneration of dopaminergic cells in the substantia nigra? The reason is that DAT is specific to dopaminergic neurons and best correlates with the density of dopaminergic neurons. Imaging other aspects of dopaminergic neuronal function—for example, dopamine synthesis rate or dopamine receptor density—can evaluate dopaminergic neurodegeneration. Indeed, there are many radioligands available for imaging these other aspects of dopaminergic neuronal function. However, dopamine synthesis imaging has some drawbacks, and postsynaptic dopamine receptor imaging does not help in diagnosing PD patients because PD pathology is on the presynaptic side. 18F-l-6-fluoro-3,4-dihydroxyphenylalanine (18F-DOPA) is a representative radioligand for dopamine synthesis and reflects dopaminergic as well as noradrenergic neuronal function. 18F-DOPA imaging involves multiple steps including the uptake and conversion of fluorodopa to fluorodopamine (15). 18F-DOPA uptake is not a direct measure of nigral cell count (15). Furthermore, compensatory upregulatory changes of dopamine synthesis rate might occur in PD, hindering accurate measurement (15). DATs are known to be downregulated in PD patients as an early response to decreased synaptic dopamine concentration (16). DAT imaging might be a more sensitive indicator of dopaminergic degeneration than 18F-DOPA (17).
RADIOLIGANDS FOR DAT IMAGING AND THEIR CLINICAL AVAILABILITY
There are several radioligands for DAT imaging. Among DAT imaging methods, SPECT using 123I-β-CIT, 123I-FP-CIT, or 99mTc-TRODAT-1 has been most widely used and approved for clinical use in different countries. 123I-FP-CIT is not the first of its kind but has recently become the first and only U.S. FDA–approved radioligand for DAT imaging for clinical purposes. This newly approved radioligand actually was already authorized for clinical use in July 2000 in Europe (18), for the differential diagnosis of patients with clinically uncertain Parkinsonian syndrome. Its diagnostic indication expanded for the differential diagnosis of probable dementia with Lewy bodies (DLB) from Alzheimer disease in July 2006 (19). In addition to Europe, Korea recently approved 123I-FP-CIT for clinical use in 2011 (20). More than 300,000 people in 34 countries have undergone 123I-FP-CIT brain SPECT as of 2011 (21). Table 1 shows the approval year of several representative DAT imaging radioligands for clinical use. In Europe, 123I-β-CIT is also available for routine clinical use. Another radioligand for DAT imaging, 99mTc-TRODAT-1, was approved for routine clinical use in Taiwan in 2005 but was reported to be underutilized for bureaucratic and economic reasons despite the advantageous imaging properties of technetium (22). Several DAT radioligands for PET have been developed. 18F-FP-CIT is available for clinical use in Korea; its first approval anywhere in the world was by the Korean FDA in 2008 (23). A newer synthesis method published in 2007 contributed to the clinical use of 18F-FP-CIT by significantly improving the radiochemical yield (24).
Approval Year for Clinical Use of Radioligands for DAT Imaging
CHARACTERISTICS OF 123I-FP-CIT
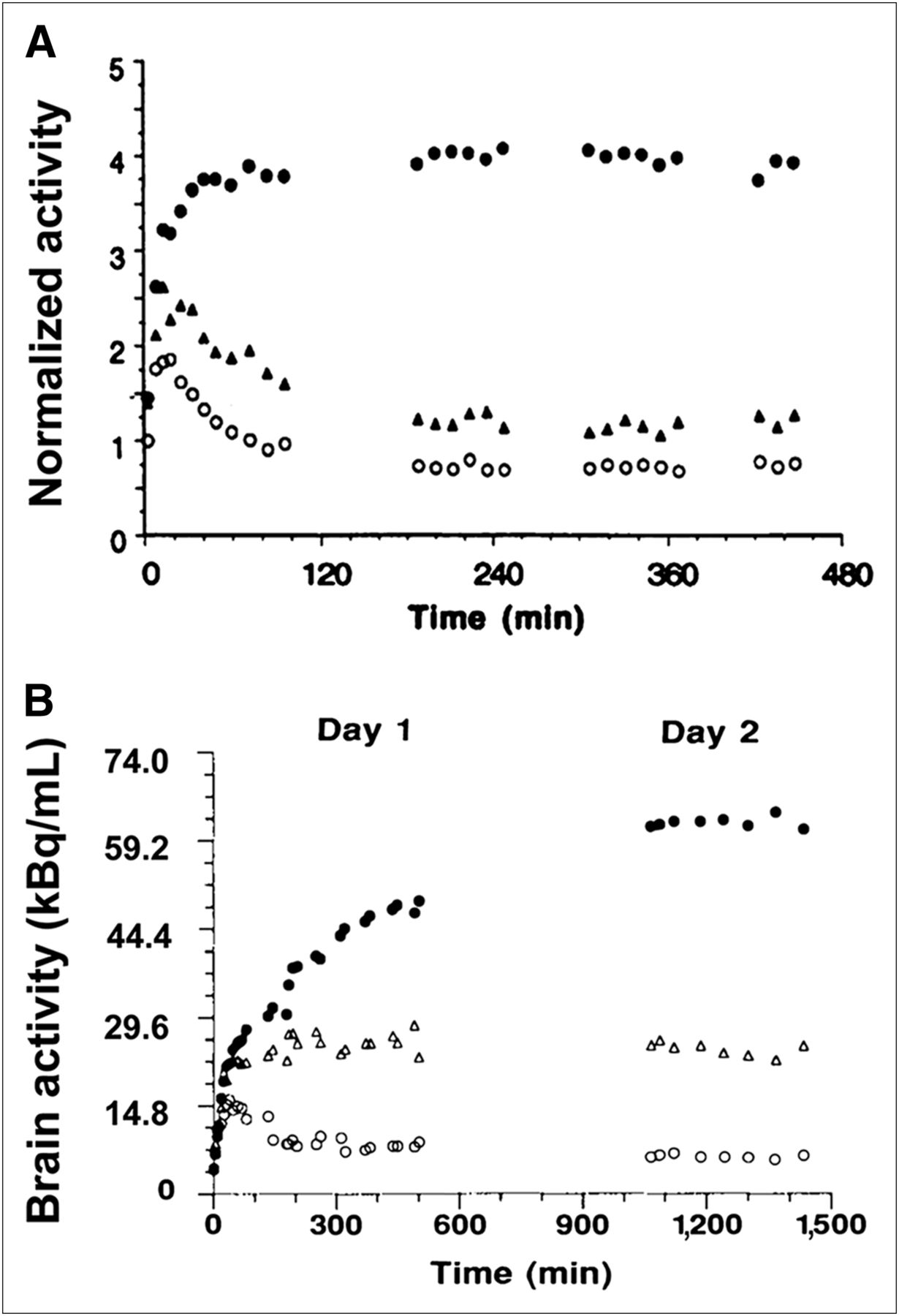
123I-FP-CIT is a radioiodinated cocaine analog. The physical half-life of 123I is 13 h, and the major γ-ray from 123I decay has an energy of 159 keV. 123I-FP-CIT is classified as a schedule II controlled substance under the Controlled Substances Act in the United States. Registration with the Drug Enforcement Agency is required to order it, and appropriate physician licensure and clinic registration are mandatory (16). The recommended dosage of 123I-FP-CIT is 111–185 MBq (3–5 mCi), typically 185 MBq (5 mCi). The effective dose of a single 123I-FP-CIT brain SPECT scan is estimated to be 2.3–4.4 mSv, which is similar to a chest CT dose (16). 123I-FP-CIT is taken up rapidly in the human striatum, and a stable level of striatal radioactivity (equilibrium of specific to nonspecific uptake of radioactivity) is achieved around 4 h after injection (Fig. 1A) (25). 123I-β-CIT was developed earlier than 123I-FP-CIT and is the first cocaine analog radioligand that came out. However, 123I-β-CIT slowly reaches a stable level of striatal radioactivity at 20–30 h after injection (Fig. 1B) (26), meaning that patients with difficulty in moving around need to visit the hospital for 2 d for injection and imaging procedures. Because of its faster kinetics, 123I-FP-CIT was a breakthrough for outpatient procedures. 123I-FP-CIT allows patients to be scanned on the same day at 3–6 h after injection. Another advantage of 123I-FP-CIT is that it has higher selectivity for DAT than 123I-β-CIT (25,27). However, nonspecific uptake in the background regions is higher with 123I-FP-CIT.
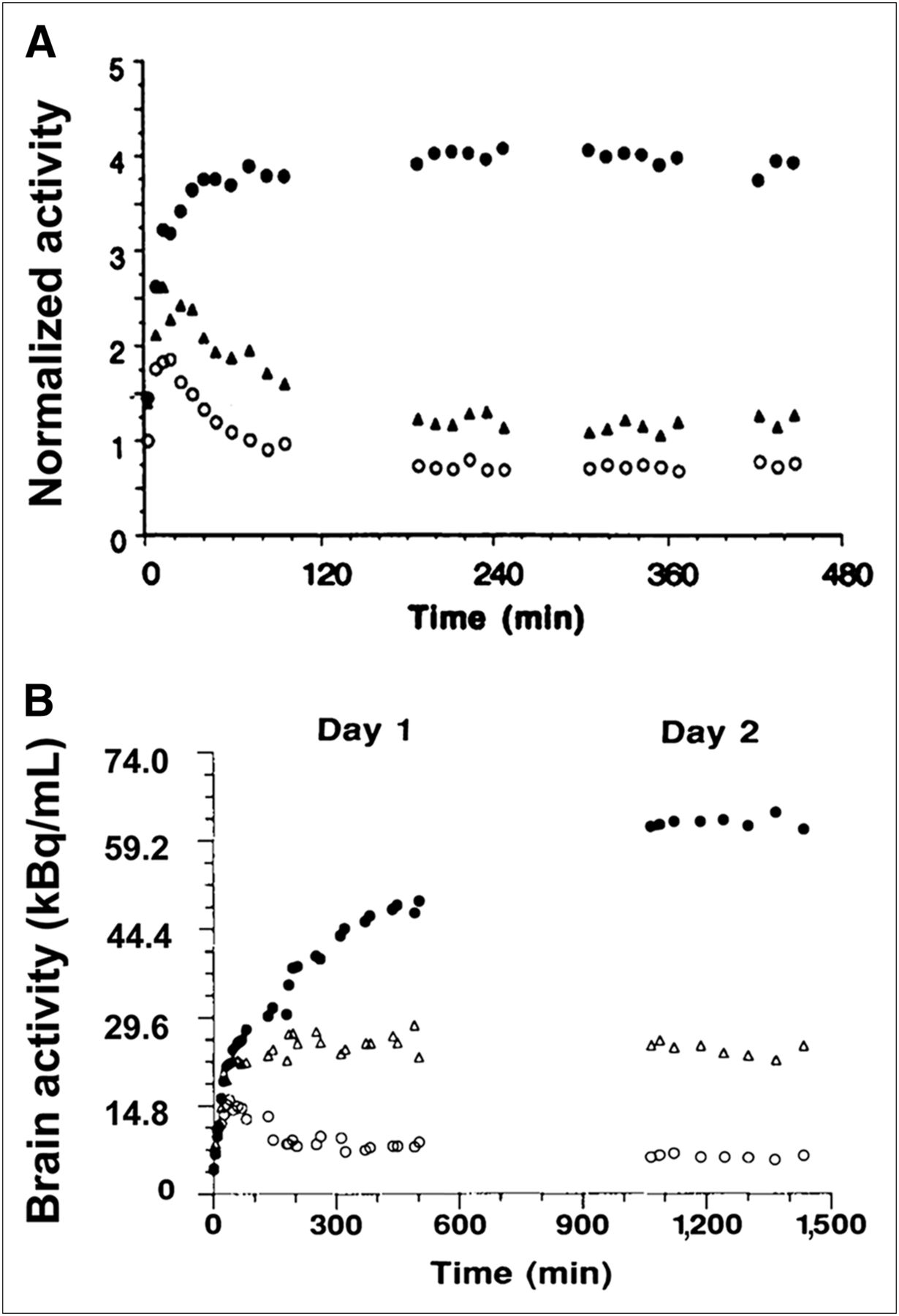
Faster kinetics of 123I-FP-CIT. In human striatum, 123I-FP-CIT (A) is taken up more rapidly than 123I-β-CIT (B). Practical clinical advantage of fast kinetics of 123I-FP-CIT is that patients can be scanned on same day 3–6 h after injection. (Panel B reprinted with permission of (26).)
DAT IMAGING PROTOCOL USING 123I-FP-CIT
Images are usually obtained at 4 h after the injection of 123I-FP-CIT, but they can be obtained 3–6 h after injection. The oral administration of potassium perchlorate or potassium iodide solution, or Lugol solution, is recommended before the 123I-FP-CIT injection, to block thyroid uptake of free radioactive iodide. In Europe, where 123I-FP-CIT has been used for a decade, Lugol solution is often not administered and some clinicians believe that it may not be necessary. Fasting is unnecessary, and patients do not need to be kept in a dim or quiet environment. Antiparkinsonian drugs including l-dopa, dopamine agonists, monoamine oxidase-B inhibitors, and catechol-O-methyl transferase inhibitors do not need to be discontinued. They showed no significant effect on the striatal 123I-FP-CIT uptake (28,29). However, selective serotonin reuptake inhibitors, which are used to treat depression in PD patients, influence 123I-FP-CIT uptake by binding to serotonin transporters (30). Central nervous system stimulants (amphetamine analogs, sympathomimetics including some nasal decongestants) also affect DAT binding, and it is recommended that they be stopped for 4 wk (28). Technical details, including parameters for image acquisition and processing, are well described in the practice guidelines of the Society of Nuclear Medicine and Molecular Imaging and a workbook from GE Healthcare (16,31).
VISUAL INTERPRETATION AND SEMIQUANTITATIVE ANALYSIS
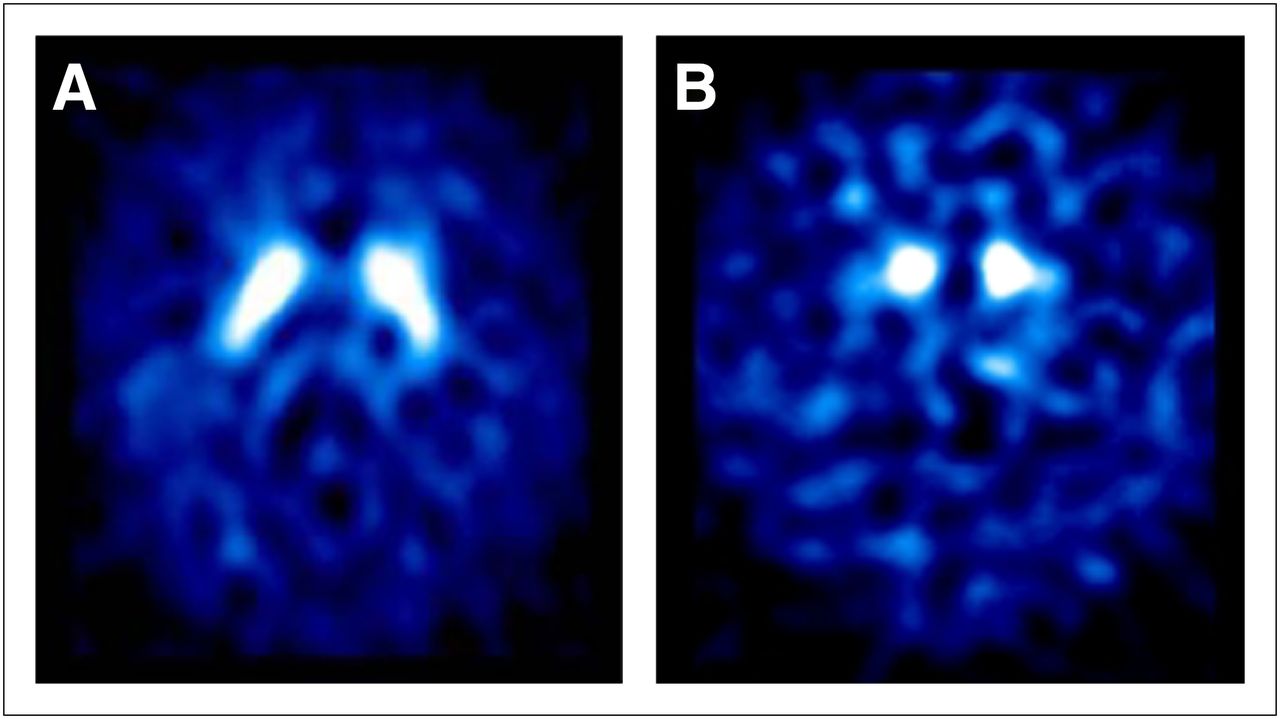
DAT SPECT results can be easily classified as normal or abnormal by visual interpretation based on the striatal activity. 123I-FP-CIT uptake pattern and density in the striatum are examined in terms of the shape of the bilateral striata, symmetry, gradient between the caudate nucleus and the putamen, and the degree of reduction. Normally, the bilateral striata appear as symmetric comma-shaped hot uptake on the imaging. In PD, 123I-FP-CIT uptake, in other words DAT density, is usually asymmetric in the left and right striata. The side with relatively lower uptake generally matches contralaterally to the clinically more affected side. As for anterior–posterior asymmetry, the putamen demonstrates more reduction than the caudate nucleus, and uptake in the dorsal–posterior putamen is more reduced than that in the other parts of the putamen (32). Figure 2 shows 123I-FP-CIT SPECT images of normal and abnormal brain. The semiquantification of DAT density in the striata can be made by calculating the ratio of specific to nonspecific binding using the cerebellum or occipital lobe as a reference region. Striatal DAT density (or striatal binding ratio) is determined by the formula mean counts of striatal region of interest divided by mean counts of a reference region of interest minus 1. For quantifying activities in small structures such as a brain stem area, a PET scan is preferable because of its superior spatial resolution (Fig. 3). Currently, there are no FDA-approved quantitative software packages for calculating the ratio of specific to nonspecific binding, but similar to the evolution of cardiac nuclear medicine, validated software packages approved by the FDA are being developed. It would be helpful to report semiquantitative evaluation results along with descriptive findings.

Brain 123I-FP-CIT SPECT images. Transaxial slices at striatal level. (A) Normal 123I-FP-CIT uptake, which is often described as comma shaped, is seen in healthy subject. (B) Striatal uptake is decreased in patient with PD. Reduction is more prominent in putamen than in caudate nucleus.

Superior spatial resolution of brain 18F-FP-CIT PET images. Superior spatial resolution of brain PET enables us to see caudate nucleus and putamen separately, and to analyze small brain structures such as in brain stem area. Another advantage of 18F-FP-CIT PET is that it can be acquired 2–3 h after injection.
CLINICAL APPLICATION OF DAT IMAGING
In clinical practice, DAT imaging assists mainly when there is clinical diagnostic uncertainty between true parkinsonism and other movement disorders (33). Patients may show a subtle and unclear initial presentation, atypical progression, or atypical therapeutic response. One in 5 suspected Parkinsonian syndrome cases remains clinically uncertain (34). Another good indication for DAT imaging might be a potential drug-induced parkinsonism (DIP) case where removing the patient from a drug is difficult (33). One criterion used to diagnose DIP is the discontinuance of a patient’s medications to determine whether symptoms improve. However, when, for example, antiepileptic or antipsychotic drugs are suspected to have induced parkinsonism in a patient, it might be more practical to image striatal DAT density than to try to discontinue those drugs. In the same context, DAT imaging is also useful when a levodopa trial is problematic (33). DAT imaging is not necessary in clinically definite PD patients. DAT imaging is currently not recommended as a stand-alone diagnostic tool (33). It does not help to differentiate PD from atypical Parkinsonian syndrome (APS) (e.g., multiple-system atrophy, progressive supranuclear palsy). Both PD and APS have presynaptic dopaminergic degeneration and demonstrate decreased striatal uptake on DAT imaging. Postsynaptic dopaminergic imaging needs to be added to increase diagnostic accuracy (35). Postsynaptic D2 receptor binding is normal or increased in PD whereas it is decreased in APS (36). 18F-FDG PET has been also used to distinguish PD from APS using their different metabolic patterns (37–39). Whether DAT imaging is useful in the assessment of treatment response, monitoring of disease progression, and early diagnosis of PD in the premotor stage is still in its research phase.
DIFFERENTIAL DIAGNOSIS OF PARKINSONISM
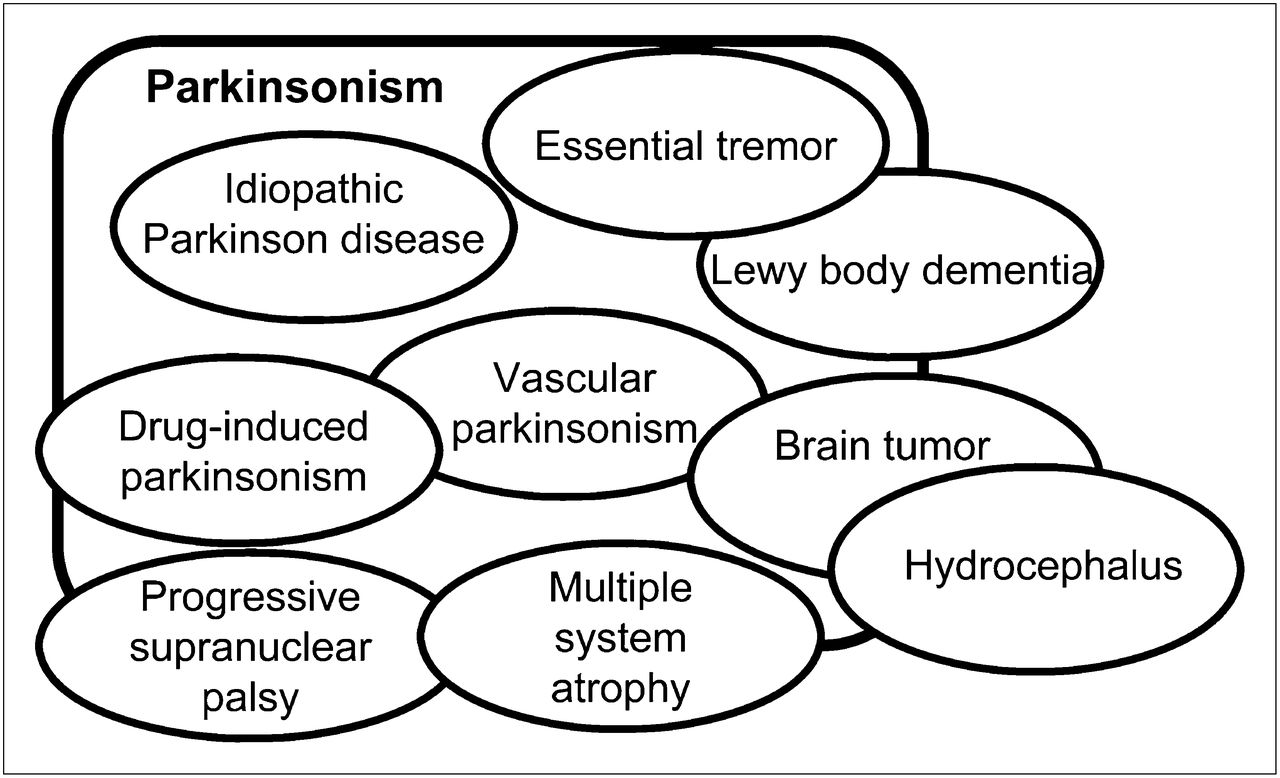
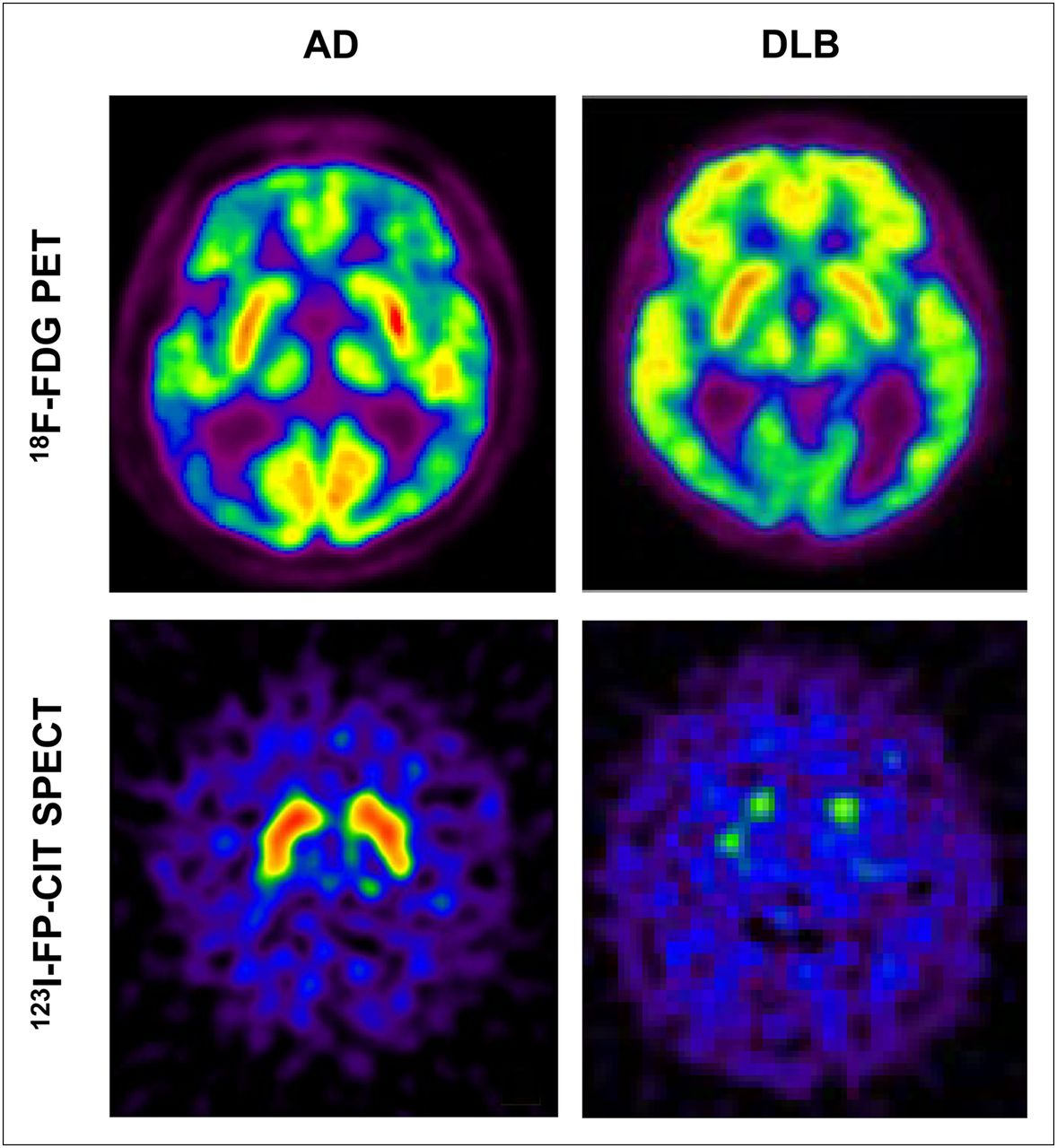
Diagnostic possibilities in parkinsonism or tremor include a variety of diseases (Fig. 4). DIP, which is induced by dopamine receptor antagonist drugs, and essential tremor, which has characteristic kinetic or postural tremor, are 2 of the most common diagnostic errors (40,41). They show normal DAT imaging results, which make it easy to differentiate them from PD (Fig. 5). Parkinsonism can also come from a cerebral infarct. Vascular parkinsonism may occur when there are vascular lesions in the basal ganglia or in the subcortical white matter (42). In vascular parkinsonism, DAT imaging shows normal or near-normal results, unless there is focal basal ganglia infarction, which leads to the characteristic punched-out deficit (13). DAT imaging is also useful to differentiate the cause of dementia. The 2 most common forms of dementia, Alzheimer disease and DLB, share clinical features and are often difficult to differentiate. With DAT imaging, these 2 disorders can be easily distinguished. DLB has dopaminergic degeneration, but Alzheimer disease does not (Fig. 6).
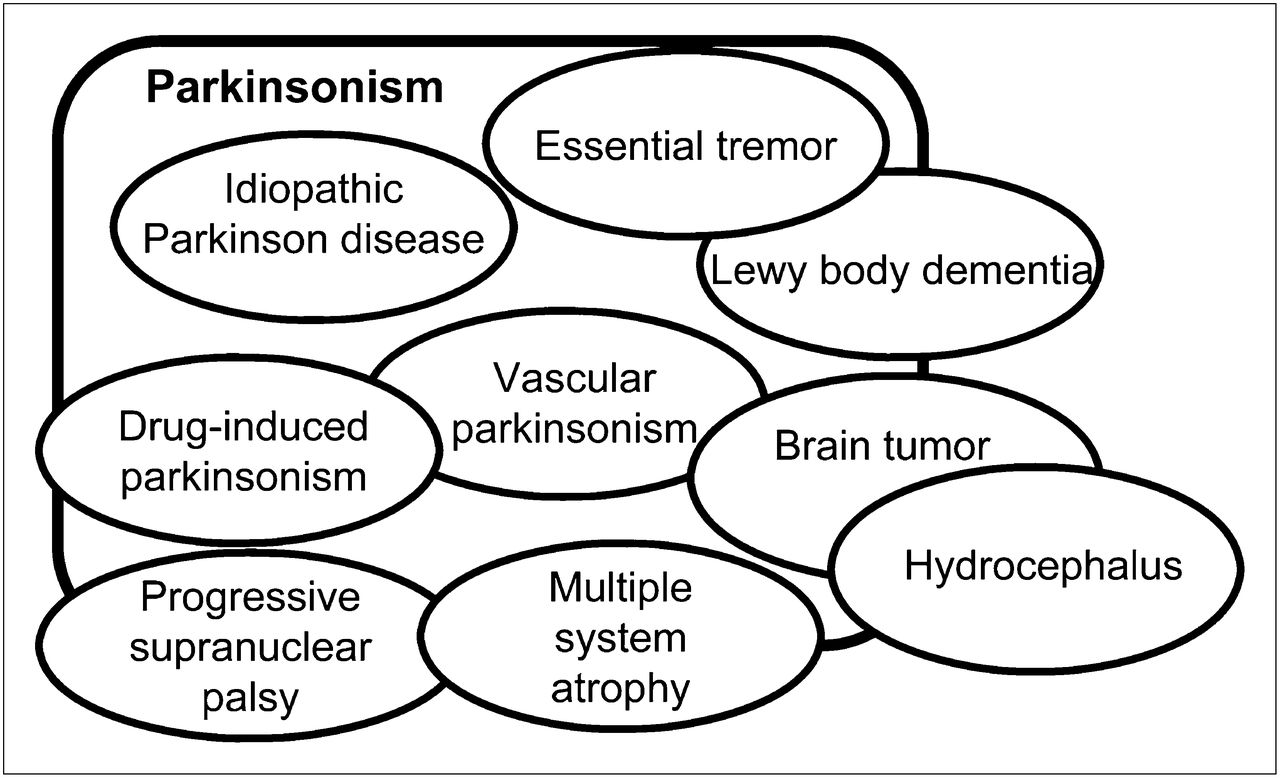
Variety of diseases mimicking idiopathic PD.
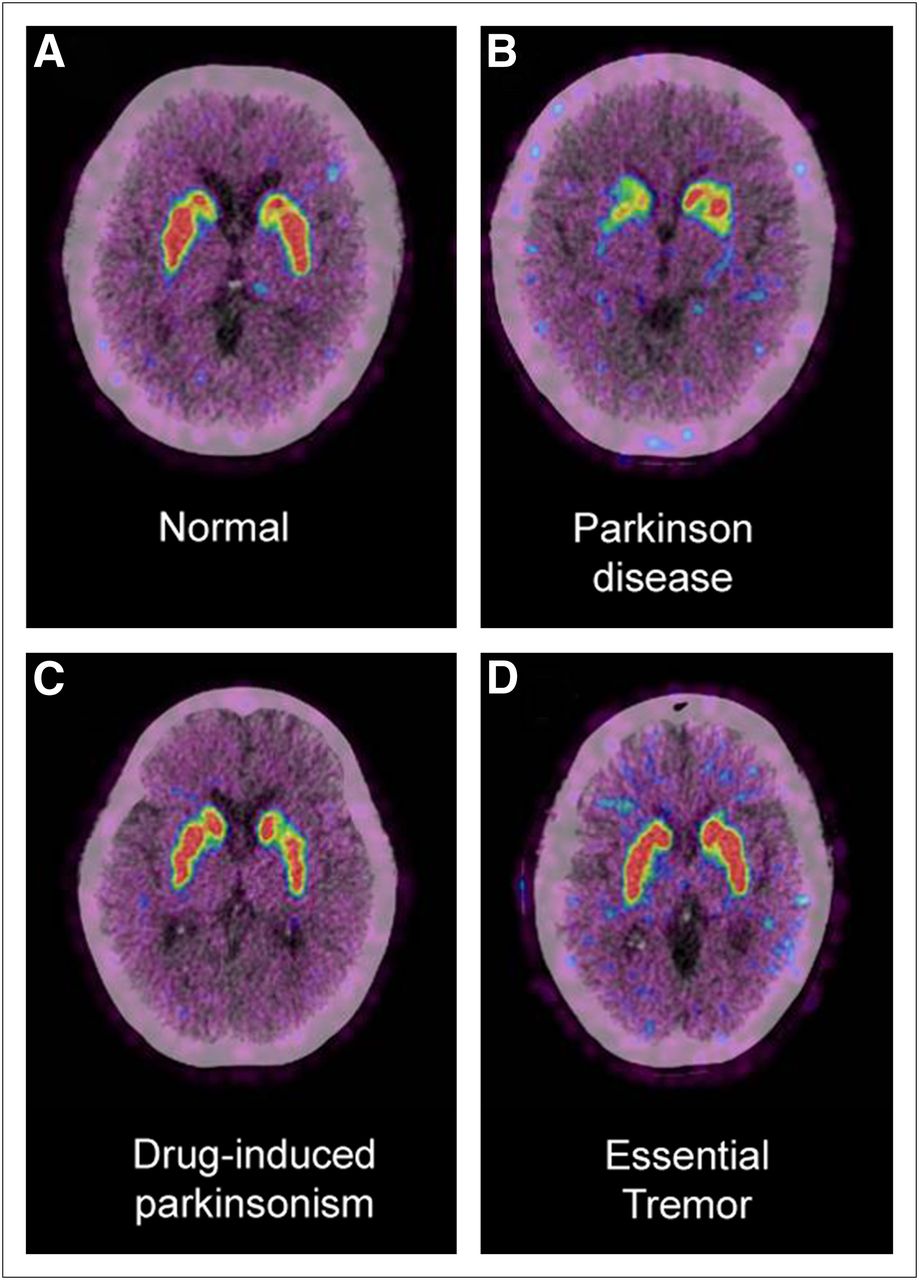
Differential diagnosis of parkinsonism using brain 18F-FP-CIT PET. Brain PET/CT images of 18F-FP-CIT uptake at level of striatum demonstrate different DAT density in different conditions. DAT density is decreased in PD patient (B), whereas DAT density is normal in healthy subject (A) and in patients with drug-induced parkinsonism (C) and essential tremor (D). DAT imaging is useful for differential diagnosis of various causes of parkinsonism. Clinical diagnosis of parkinsonism is quite often straightforward, obviating additional tests, but when overlap and incomplete syndromes are present, improvements in diagnostic accuracy may be possible using DAT imaging.
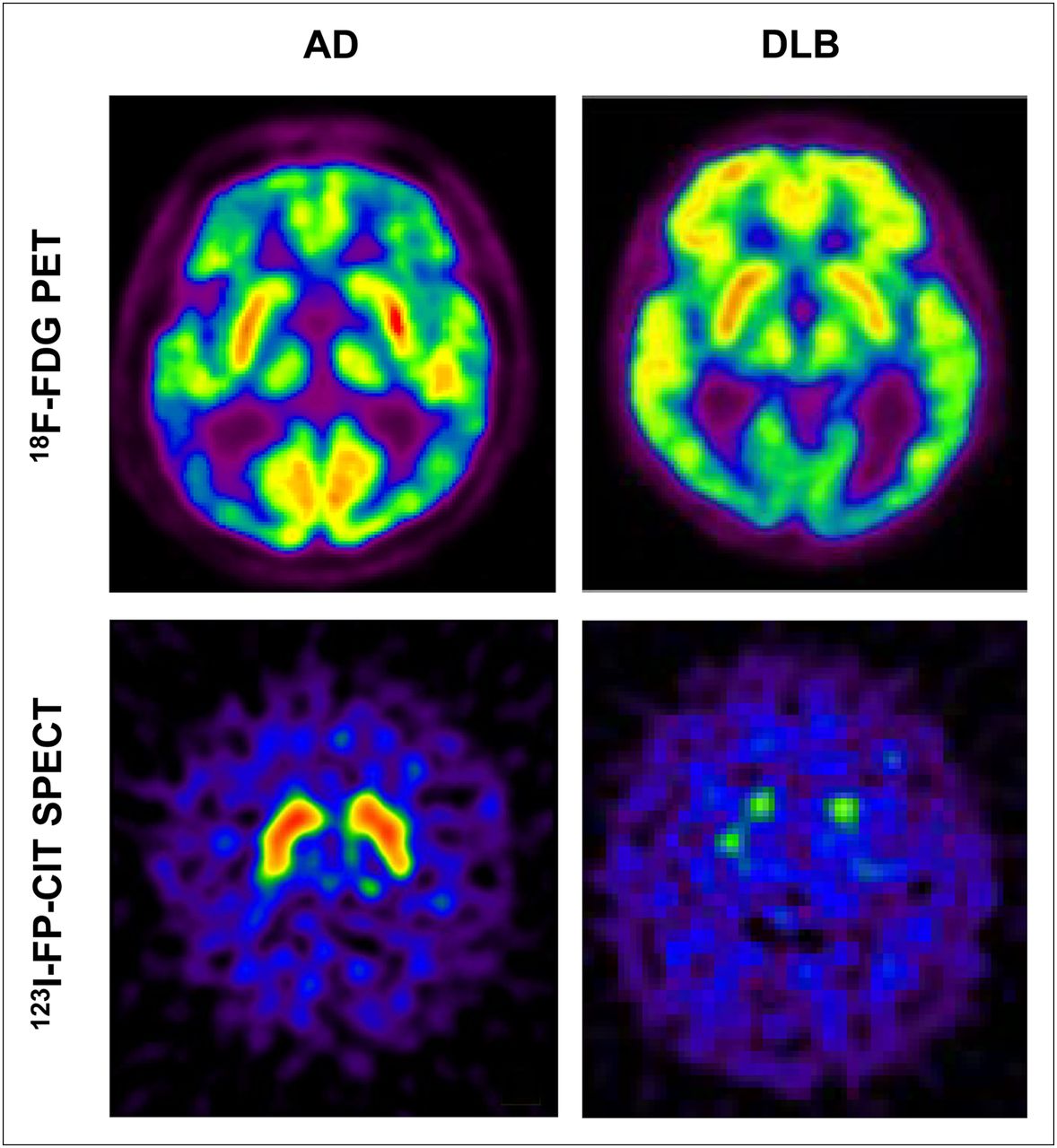
Differential diagnosis of dementia using brain 123F-FP-CIT SPECT. The 2 most common forms of dementia, Alzheimer disease (AD) and DLB, share clinical features and are often difficult to differentiate. 18F-FDG PET is useful when typical bilateral temporoparietal hypometabolism is seen in AD and occipital hypometabolism is seen in DLB, as demonstrated in these images; however, that is not always case. With DAT imaging, for example, using 123I-FP-CIT, these 2 disorders can be more easily distinguished. Striatal dopaminergic deficit occurs in DLB but not in AD.
DIAGNOSTIC VALUE OF DAT IMAGING
Brain CT or MRI is usually performed in the diagnostic work-up of parkinsonism. However, there is no PD-specific finding on those images. Structural imaging modalities are mainly required to rule out secondary forms of parkinsonism (43). DAT imaging enables the in vivo demonstration of striatal dopamine activity (Fig. 7). 123I-FP-CIT SPECT has high power to discriminate PD from normal aging, particularly when DAT density in the putamen is evaluated (44). The sensitivity and specificity of 123I-FP-CIT SPECT for differentiating essential tremor from PD are reported to be 95% and 94%, respectively (44). One multicenter study showed that 123I-FP-CIT DAT SPECT contributed to a change in diagnosis in 52% of patients and also prompted changes in the clinical management in 72% of patients (34).
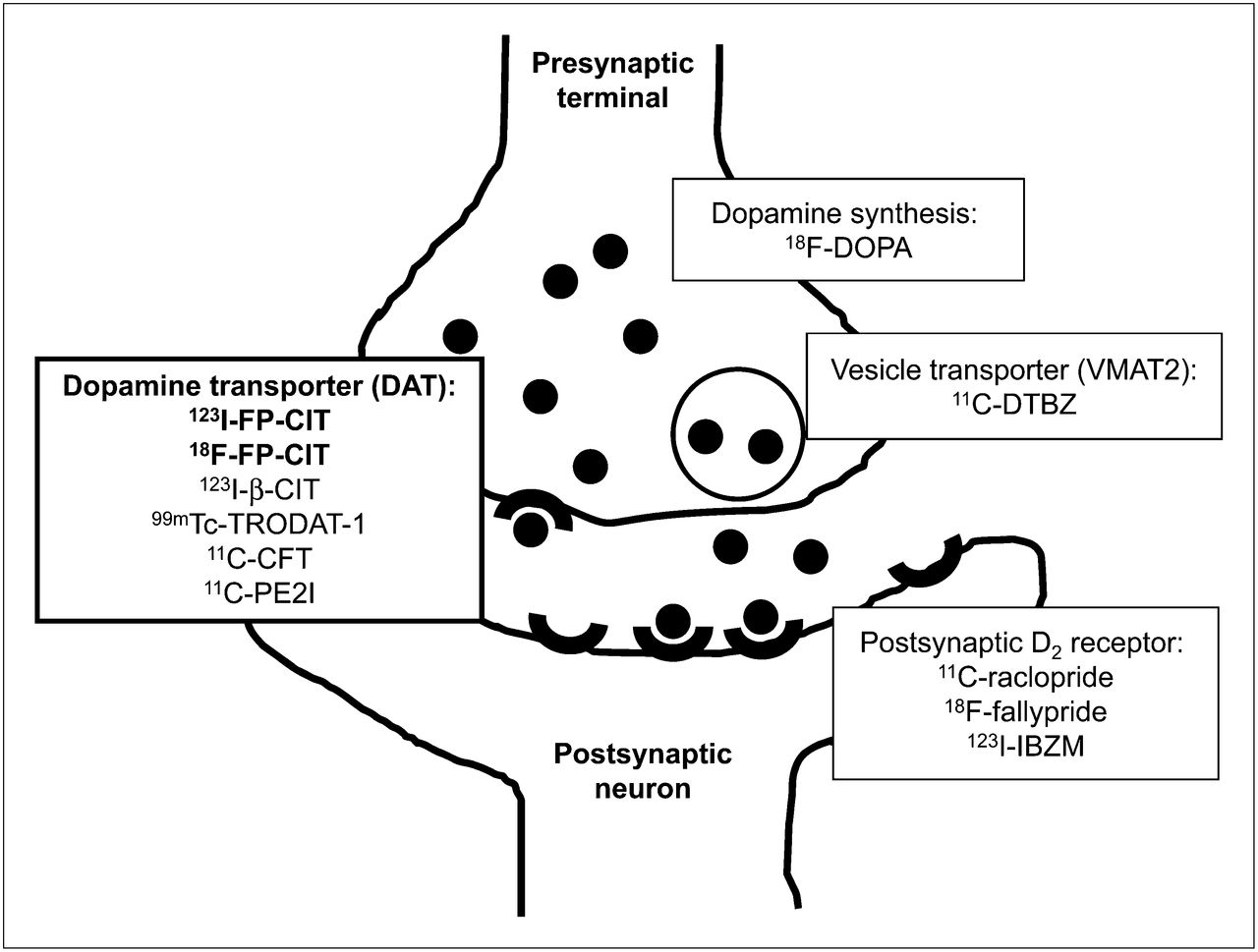
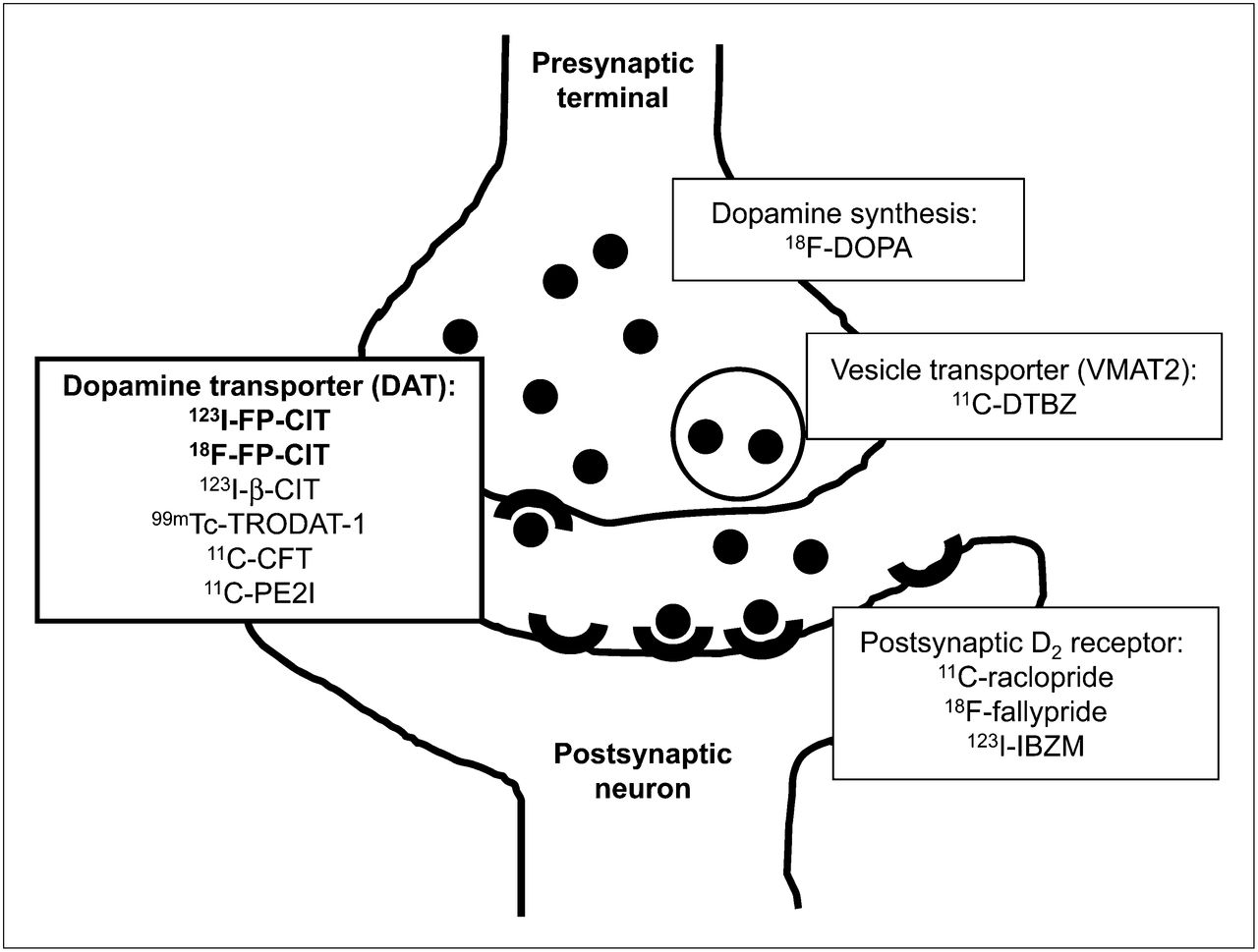
Molecular targets for imaging dopamine system. Illustration is of dopamine nerve terminal and examples of several radioligands that enable in vivo demonstration of dopamine synthesis, rerelease into synaptic cleft, uptake by postsynaptic receptors, and active reuptake by DAT, respectively. Each step of dopamine synthesis, release, and reuptake can be imaged and measured with nuclear medicine molecular imaging techniques.
DAT DENSITY AND DISEASE SEVERITY
The most frequently asked question by most PD patients might be how severe their symptom is and in what stage of disease they are categorized. Evaluating disease severity is important in establishing a proper treatment strategy. The Unified Parkinson Disease Rating Scale and Hoehn and Yahr Scale are the most commonly and most widely used scales to assess the clinical severity of PD. They are also used in research to determine the eligibility of patients to participate in research (45). According to the Hoehn and Yahr Scale, increasing Parkinsonian motor impairment can be charted from unilateral (stage I) to bilateral involvement (stage II) without balance difficulties, to the presence of postural instability (stage III), loss of physical independence (stage IV), and being wheelchair- or bed-bound (stage V) (46). Striatal presynaptic dopaminergic function evaluated by DAT imaging reflects Hoehn and Yahr staging (32,47) and is correlated with the motor Unified Parkinson Disease Rating Scale (32). The reduction of striatal DAT density is more profound in the advanced stages than in the early stages. Nondopaminergic symptoms such as swallowing and speech difficulties, sleep disturbance, constipation, depression, and dementia also matter to the quality of life for PD patients (48). Our nuclear medicine molecular imaging technique is expected to play a key role in investigating nondopaminergic neuronal systems in order to better understand and treat PD.
COST EFFECTIVENESS OF DAT IMAGING
Although DAT imaging may be expensive, the cost effectiveness of DAT imaging is reported to be good (49–51). For example, Van Laere et al. (51) analyzed the cost effectiveness of 123I-FP-CIT SPECT in patients with inconclusive Parkinsonian features, by working on a complete Belgian registry of 1,701 consecutive patients. They found that the initial diagnosis was changed in 51.5% of patients, and the management was altered in 49%. However, cost effectiveness may differ from country to country according to each country’s health care systems. There is not enough evidence to generalize the cost effectiveness of 123I-FP-CIT at the moment.
CONCLUSION
A new era of DAT imaging has begun with the approval of 123I-FP-CIT for clinical use by the FDA. 123I-FP-CIT binds to DAT protein and enables reliable visualization of DAT distribution in the striatum. 123I-FP-CIT SPECT and SPECT or PET using various other DAT radioligands are useful as diagnostic adjuncts in movement disorders and dementia. They give diagnostic capability to physicians that may lead to timely and appropriate treatments for patients with suspected Parkinsonian syndrome.
Acknowledgments
We give special thanks to Eplida S. Crawford, CNMT, clinical associate professor, University at Buffalo, for helpful comments and suggestions on the manuscript. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 16, 2012.
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNMMI WEB SITE (http://www.snmmi.org/ce_online) THROUGH DECEMBER 2014.
REFERENCES
- Received for publication July 23, 2012.
- Accepted for publication October 10, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- A NEW ERA OF CLINICAL DOPAMINE TRANSPORTER IMAGING USING 123I-LABELED 2ς-CARBOMETHOXY-3ς-(4-IODOPHENYL)-N-(3-FLUOROPROPYL)NORTROPANE (123I-FP-CIT)
- DAT DENSITY AND 123I-FP-CIT UPTAKE
- WHY DO WE IMAGE STRIATAL DAT DENSITY?
- RADIOLIGANDS FOR DAT IMAGING AND THEIR CLINICAL AVAILABILITY
- CHARACTERISTICS OF 123I-FP-CIT
- DAT IMAGING PROTOCOL USING 123I-FP-CIT
- VISUAL INTERPRETATION AND SEMIQUANTITATIVE ANALYSIS
- CLINICAL APPLICATION OF DAT IMAGING
- DIFFERENTIAL DIAGNOSIS OF PARKINSONISM
- DIAGNOSTIC VALUE OF DAT IMAGING
- DAT DENSITY AND DISEASE SEVERITY
- COST EFFECTIVENESS OF DAT IMAGING
- CONCLUSION
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.