


Article Figures & Data
Figures
- FIGURE 1.
Sympathetic (brown) and parasympathetic (blue) innervation of heart and systemic vasculature. Postganglionic sympathetic neurons are seen innervating heart and systemic vasculature.
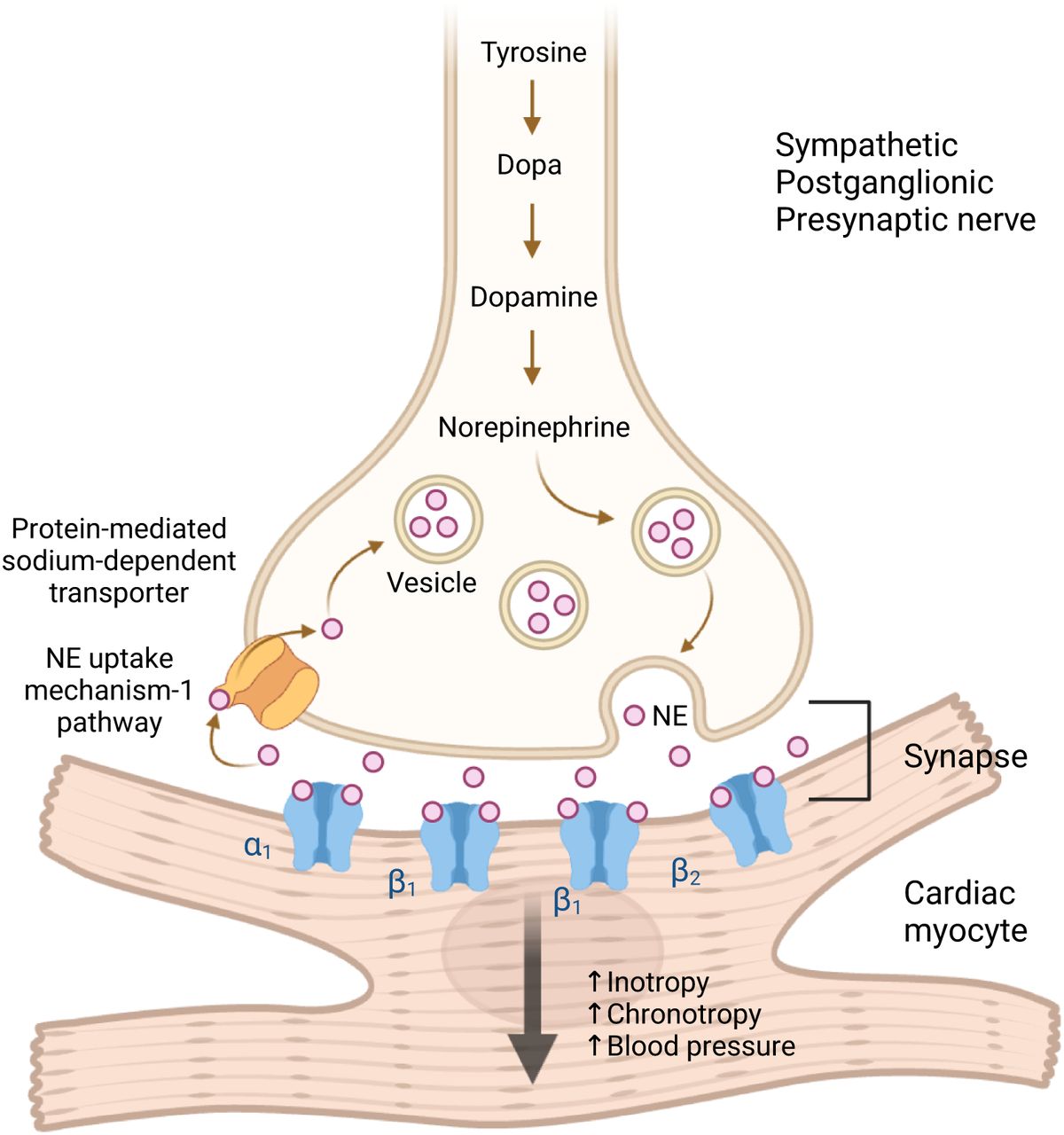
- FIGURE 2.
Diagram of sympathetic neuronal synapse with cardiac myocyte, demonstrating norepinephrine (NE) synthesis, storage, release, and reuptake.
- FIGURE 3.
Chemical structure of norepinephrine and norepinephrine radiolabeled with 123I-MIBG.
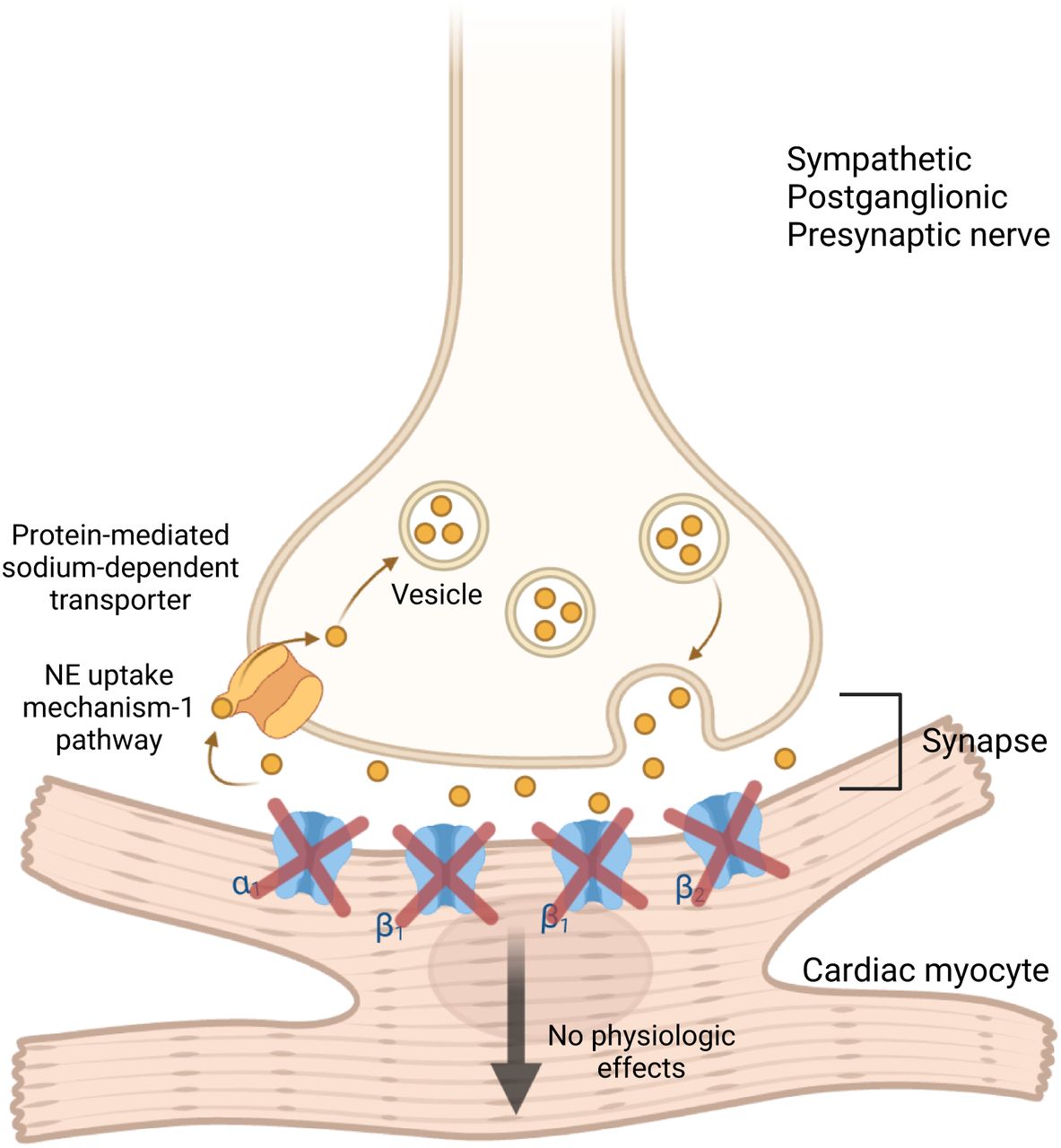
- FIGURE 4.
Sympathetic postganglionic presynaptic nerve synapsing with cardiac myocyte. 123I-MIBG uptake at synapse mimics norepinephrine (NE) reuptake and does not bind to adrenergic receptors on myocyte membrane nor result in downstream sympathetic effects.
- FIGURE 5.
After injection of 123I-MIBG (yellow), patient undergoes imaging with 3 generalized outcomes. Normal physiologic uptake signifies global radiotracer distribution throughout heart’s sympathetic regions significantly more than background mediastinal activity. Globally decreased (lighter yellow) or focally absent uptake (black) signifies conditions with abnormally reduced sympathetic innervation, such as PD or heart failure. Lastly, focally decreased uptake can be observed in conditions causing localized defects in sympathetic innervation, such as ischemic infarcts.
- FIGURE 6.
Example of 123I-MIBG ROIs drawn for HMR calculation. Horizontal black line indicates location of clavicular heads, below which there is freehand rectangle for mediastinal background ROI (our technologists freehand draw these rectangles). Yellow circle encloses myocardial uptake.
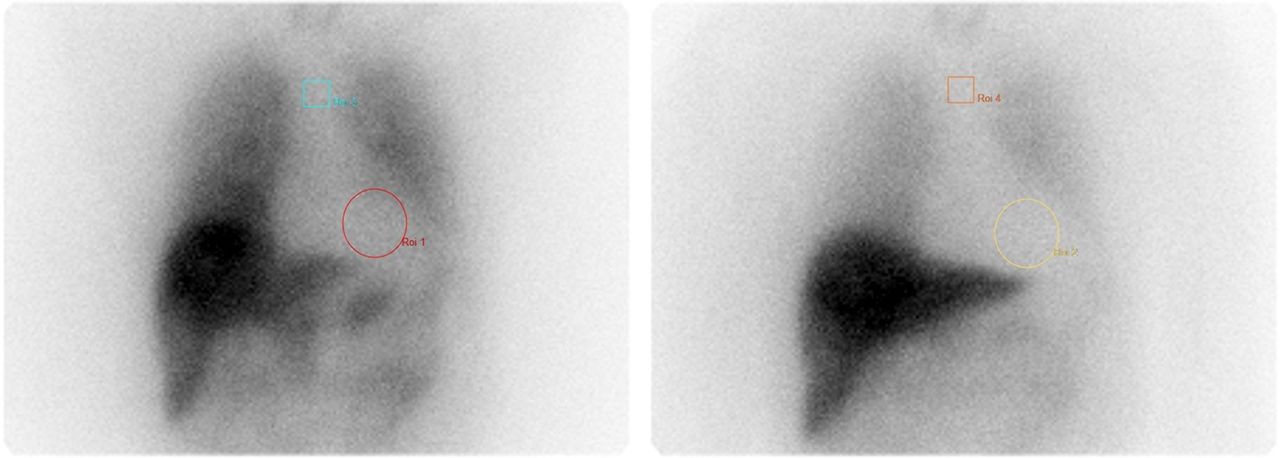
- FIGURE 7.
Example of early (15 min) (A) and delayed (4 h) (B) images for 123I-MIBG scan demonstrating abnormal increased WR of 42.45%.







Tables
Indication Contraindication and precaution Patient preparation and education Radiopharmaceutical, dose, and administration Evaluation of cardiac sympathetic innervation Known hypersensitivity to iobenguane or iobenguane sulfate When medically feasible, withhold drugs known to interfere with uptake of 123I-MIBG 123I-MIBG For diagnosis and prognosis of diseases such as congestive heart failure, myocardial infarction, diabetes mellitus, neurodegenerative disorders, cardiac transplant, differentiating various neurodegenerative diseases such as PD from MSA, dementia of Lewy body from Alzheimer disease Risk of serious reactions in infants due to benzyl alcohol preservative: neonates and infants can experience serious and fatal adverse reactions, including “gasping syndrome” with benzyl alcohol–preserved drugs such as current commercially available 123I-MIBG in the United States (AdreView) Nursing mothers should pump and discard breast milk for 6 d after 123I-MIBG administration to minimize the risk to nursing infants Activity: Adults ≥16 y or children <16 y and ≥70 kg is 10 mCi (370 MBq)
Children <16 y and <70 kg is 0.14 mCi/kg (5.2 MBq/kg)
Minimum recommended activity is 1 mCi (37 MBq)
No appropriate use criteria have been developed to date for cardiac 123I-MIBG scans Severe renal impairment can cause increased radiation exposure due AdreView clearance by glomerular filtration and nondialyzable property Patients should stop eating food containing vanillin and catecholaminelike compounds (e.g., chocolate and blue cheese) for approximately 1 wk prior Technique of administration: Standard slow intravenous injection over 1–2 min
Pregnancy: radioactive iodine can cross the placenta and permanently impair fetal thyroid function, causing fetal harm; do not administer to pregnant women Pretreatment with potassium iodine given orally at least 1 h before injection of the radiopharmaceutical: Adult dose: 130 mg of potassium iodide (2 drops or 0.13 mL of saturated solution of potassium iodide) in 1 ounce = 30 mL of distilled water
Pediatric Dose:
○ 1–36 mo: 42.5 mg of potassium iodate
○ 3–12 y: 85 mg of potassium iodate
○ Above 12 y old: 170 mg of potassium iodate
○ Alternative is potassium perchlorate (400 mg for adults, body weight-adjusted for children)
Lactation: 123I is present in breast milk, and there is no information on its effect on breastfed infants Pediatric use: safety and effectiveness have not been established in newborns <1 mo old or in any pediatric patients with congestive heart failure Drug group Drug name Withdrawal time Mechanism of action Adrenergic neuron blockers Guanethidine, reserpine 48 h 2, 3 α-blockers Phenoxybenzamine (intravenous doses) 15 d 5 Antiarrhythmics for ventricular arrhythmias Amiodarone Not practical to withdraw 1, 3 Antipsychotics (neuroleptics) Chlorpromazine 24 h 1 Antipsychotics (neuroleptics) Fluphenazine 24 h or 1 mo for depot 1 Antipsychotics (neuroleptics) Haloperidol 48 h or 1 mo for depot 1 β2 stimulants Salmeterol, salbutamol 24 h 3 Calcium channel blockers Diltiazem, nifedipine 24 h 4 Calcium channel blockers Felodipine, amlodipine, nicardipine, verapamil 48 h 4 Combined α- and β-blocker Labetalol 72 h 1, 3 Cocaine 7–14 d 1 Inotropic sympathomimetics Dobutamine, dopamine 24 h 3 Opioid analgesics Tramadol 24 h 1 Opioid 7–14 d Sedating antihistamines Promethazine 24 h 1 Sympathomimetics for glaucoma Brimonidine 48 h 3 Systemic and local nasal decongestants Pseudoephedrine, phenylephrine 48 h 3 Systemic and local nasal decongestants Ephedrine 24 h 1 Antipsychotics (neuroleptics) Clozapine 7 d 1 Antipsychotics (neuroleptics) Olanzapine 7 − 10 d 1 Antipsychotics (neuroleptics) Quetiapine 48 h 1 Antipsychotics (neuroleptics) Risperidone 5 d or 1 mo for depot 1 Tricyclic antidepressants Imipramine, nortriptyline, doxepin 24 h 1 Tricyclic antidepressants Amitriptyline 48 h 1 Tricyclic-related antidepressants Venlafaxine 48 h 1 Tricyclic-related antidepressants Mirtazapine 8 d 1 Vasoconstrictor sympathomimetics Norepinephrine 24 h 3 Table adapted from articles reviewing the practical aspects of 123I-MIBG imaging (30,36,37). Mechanism of action 1: inhibition of norepinephrine uptake mechanism-1 pathway. Mechanism of action 2: inhibition of uptake by active transport into vesicles. Mechanism of action 3: depletion of granules. Mechanism of action 4: increased uptake and retention.
Parameter Characteristic Standard/preferred/optional Camera type Large–field-of-view γ-camera Standard Energy peak 159 keV Standard Energy window 20% Standard Collimator Low-energy, high resolution, parallel hole Standard Patient position Supine Standard Field of view Heart/chest Standard Injection-to-imaging time (delayed images) Late images at 3 h 50 min Standard Planar Standard Acquisition type Static Standard Detector configuration 180° Standard Views Anterior and lateral Standard Number of views 2 Standard Counts/time per view 10 min per image Standard Matrix 256 × 256 (minimum 128 × 128) Standard Magnification Zoom = 1 Standard SPECT or SPECT/CT Optional Acquisition type Step and shoot Optional Patient position Supine Optional Orbit 360° Optional Matrix 128 × 128 Optional Magnification Zoom = 1 Optional Pixel size Per camera settings Optional Projections per detector 120 steps (60 steps/detector) Optional Time per projection 30 s per step Optional CT attenuation correction Standard attenuation correction Optional CT parameters 120 kV, 25 mA, pitch = 1.25 Optional CT parameters Slice thickness, 2.5 mm; 1 s/rotation Optional - TABLE 4.
Large Clinical Trials and Cohort Studies Using 123I-MIBG for Heart Failure Prognostication and PD or DLB Diagnosis
Indication Study Type of study Year Study patients Delayed time Delayed HMR threshold or mean ± SD WR threshold or mean ± SD Heart failure Seo et al. Single center 2022 148 3.3 h 1.9 Nakata et al. Multicenter 2013 1322 3–4 h 1.68 43% Doi et al. Single center 2012 468 4 h 1.57 and 1.50 ± 0.36 41.3% ± 9.8% Jacobson et al. Multicenter 2010 961 3 h 50 min 1.6 and 1.39 ± 0.18 41.8% ± 17.3% Nakata et al. Single center 1998 414 3–4 h 1.74 and 1.56 ± 0.36 PD or DLB Odagiri et al. Single center 2016 54 3 h 1.59 ± 0.34 for PD/1.31 ± 0.21 for DLB Oka et al. Single center 2011 110 3–4 h 1.58 ± 0.43 Kashihara et al. Single center 2006 188 4 h 1.37 ± 0.27 for PD/1.47 ± 0.37 for DLB Nagayama et al. Single center 2005 391 4 h 1.38 ± 0.29 for PD/1.17 ± 0.06 for DLB Variety of delayed times were used, with 4 h being most common. Various thresholds and mean values for delayed HMR and WR were used or discovered. 1.6 delayed HMR threshold used in ADMIRE-HF trial does tend to fit many trial thresholds and mean values (32,46,48,55–60).
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.