


Article Figures & Data
Figures
- FIGURE 1.
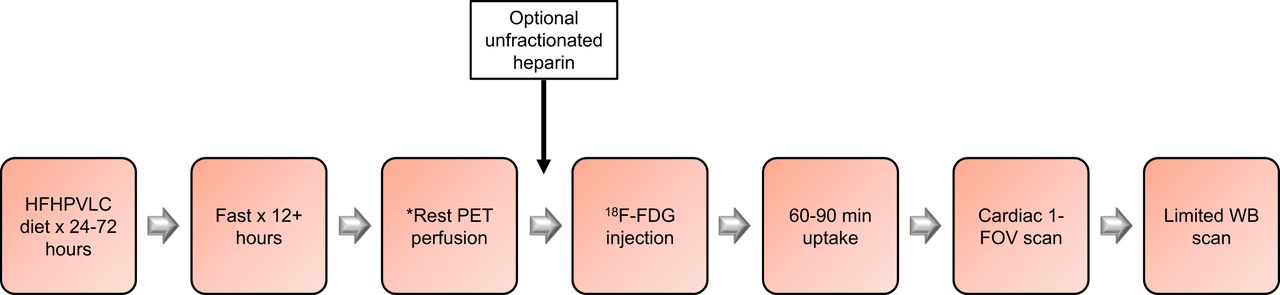
Workflow example for 1-d cardiac sarcoid PET/CT imaging. *One-day PET/CT protocols currently use 82Rb-chloride or 13N-ammonia for rest PET perfusion imaging. Use of 18F perfusion radiopharmaceuticals may require increased time between rest PET perfusion and 18F-FDG scans.
- FIGURE 2.
Scan 1 82Rb-chloride rest perfusion (top rows) and 18F-FDG cardiac metabolism (bottom rows). Rest perfusion images show small mid inferolateral wall defect (white arrows) and normal distribution of activity throughout remaining LV myocardium. Gated rest LVEF is 32%. 18F-FDG cardiac slices show suboptimal display intensity for 18F-FDG cardiac sarcoidosis imaging, as neither 18F-FDG myocardial blood-pool activity nor activity in LV myocardial wall can be appreciated in current display.
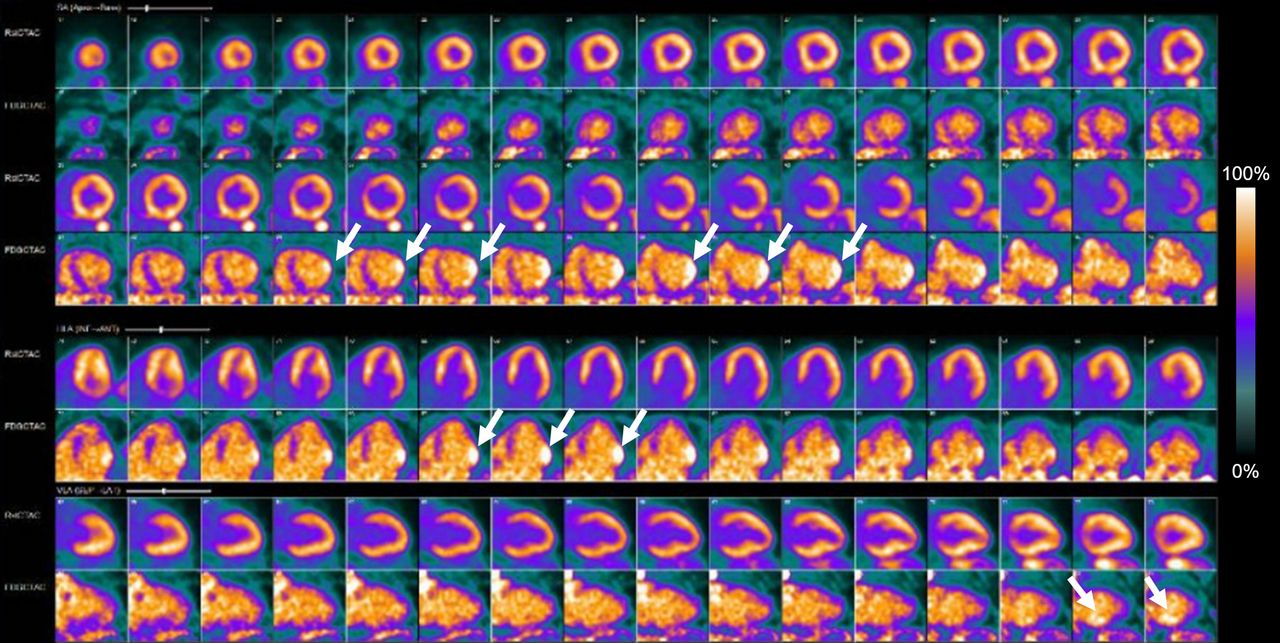
- FIGURE 3.
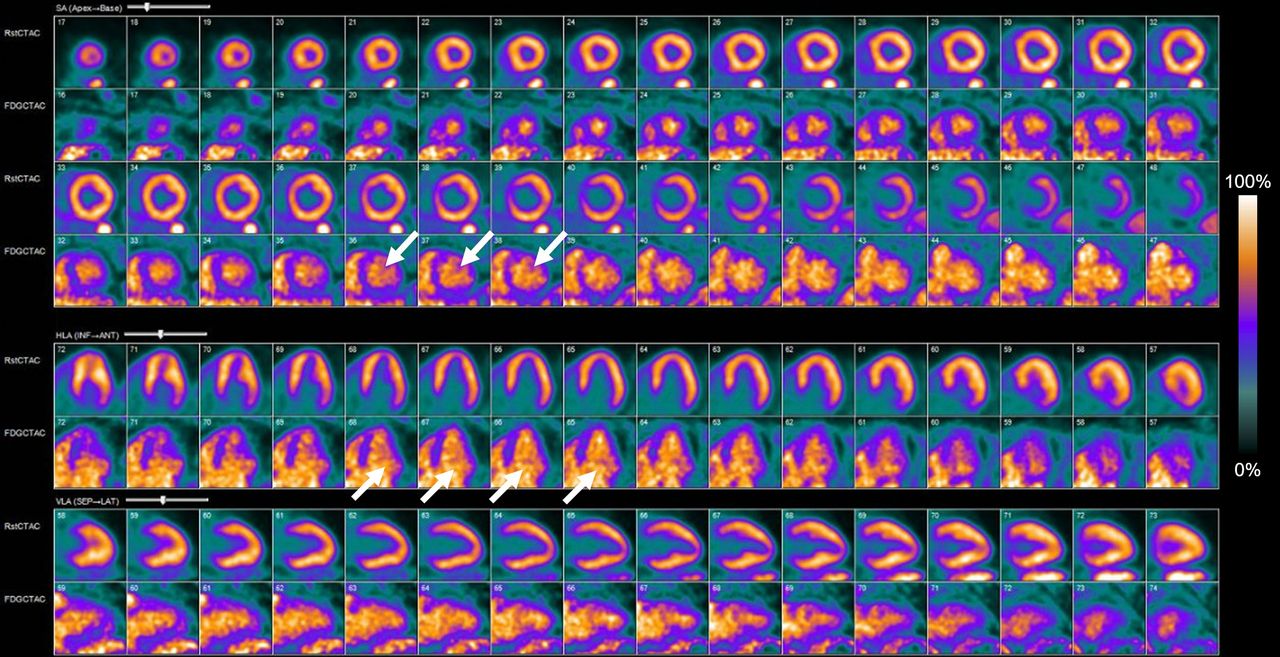
Scan 1 82Rb-chloride rest perfusion (top rows) and rescaled 18F-FDG cardiac metabolism (bottom rows). Images show appropriate 18F-FDG display intensity with blood-pool activity (white arrows) brighter than LV wall, indicating normal FDG uptake pattern. No evidence of any focally increased 18F-FDG uptake in LV myocardial wall is seen, which indicates negative examination for active cardiac sarcoidosis.
- FIGURE 4.
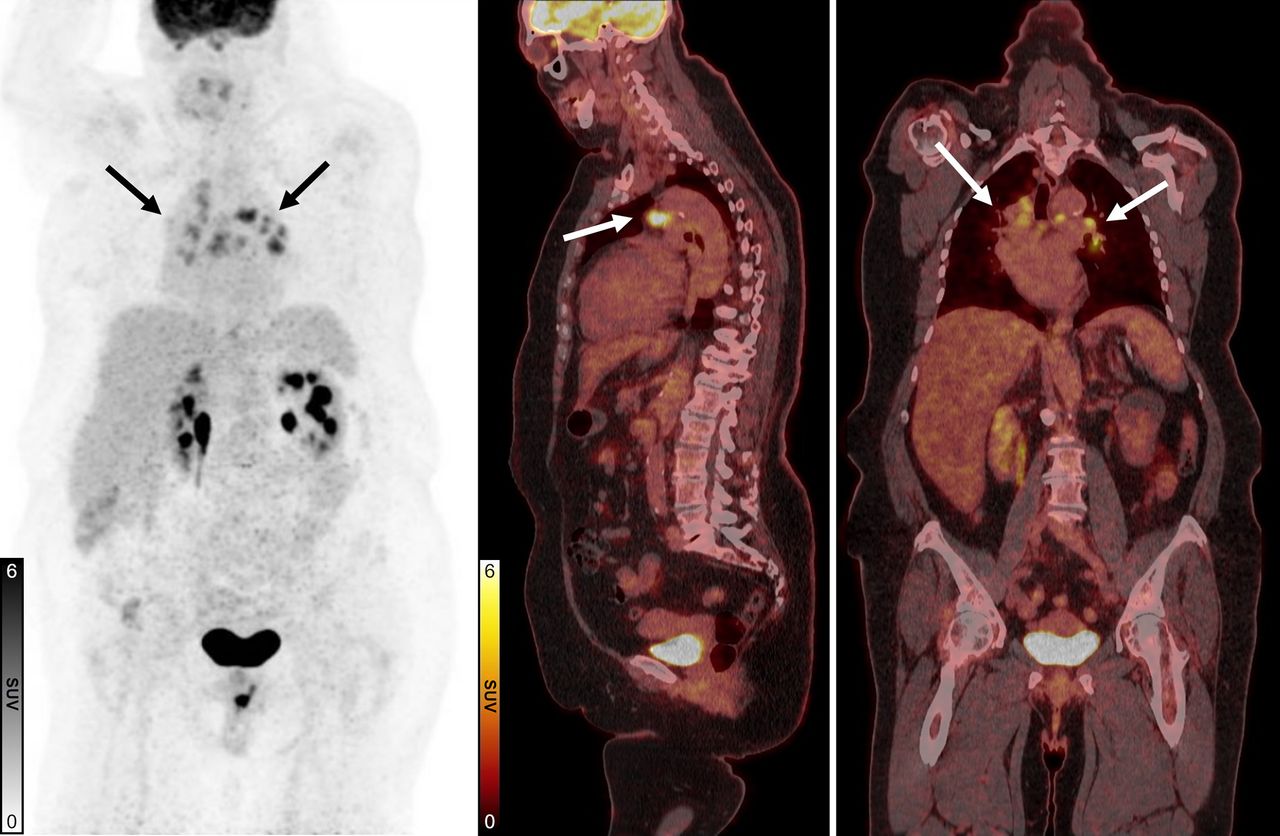
Scan 1 18F-FDG maximum-intensity projection (left), fused 18F-FDG PET/CT sagittal (middle), and fused 18F-FDG PET/CT coronal (right) views. Images show diffuse hypermetabolic uptake (arrows) in mediastinal and hilar lymphadenopathy biopsy-proven noncaseating granulomatous disease. 18F-FDG PET/CT scan 1 is negative for cardiac sarcoidosis but positive for extracardiac sarcoidosis.
- FIGURE 5.
Scan 2 82Rb-chloride rest perfusion (top rows) and 18F-FDG cardiac metabolism (bottom rows). Images show diagnostic evaluation with 18F-FDG blood-pool activity indicating adequate dietary preparation. Rest images show borderline hypoperfusion in basal to mid inferolateral wall and moderate LV enlargement. Rest gated images showed 31% LVEF. 18F-FDG images show suspected early-to-progressive stable cardiac sarcoidosis with moderate inflammatory 18F-FDG uptake in basal to mid inferolateral wall (arrows).
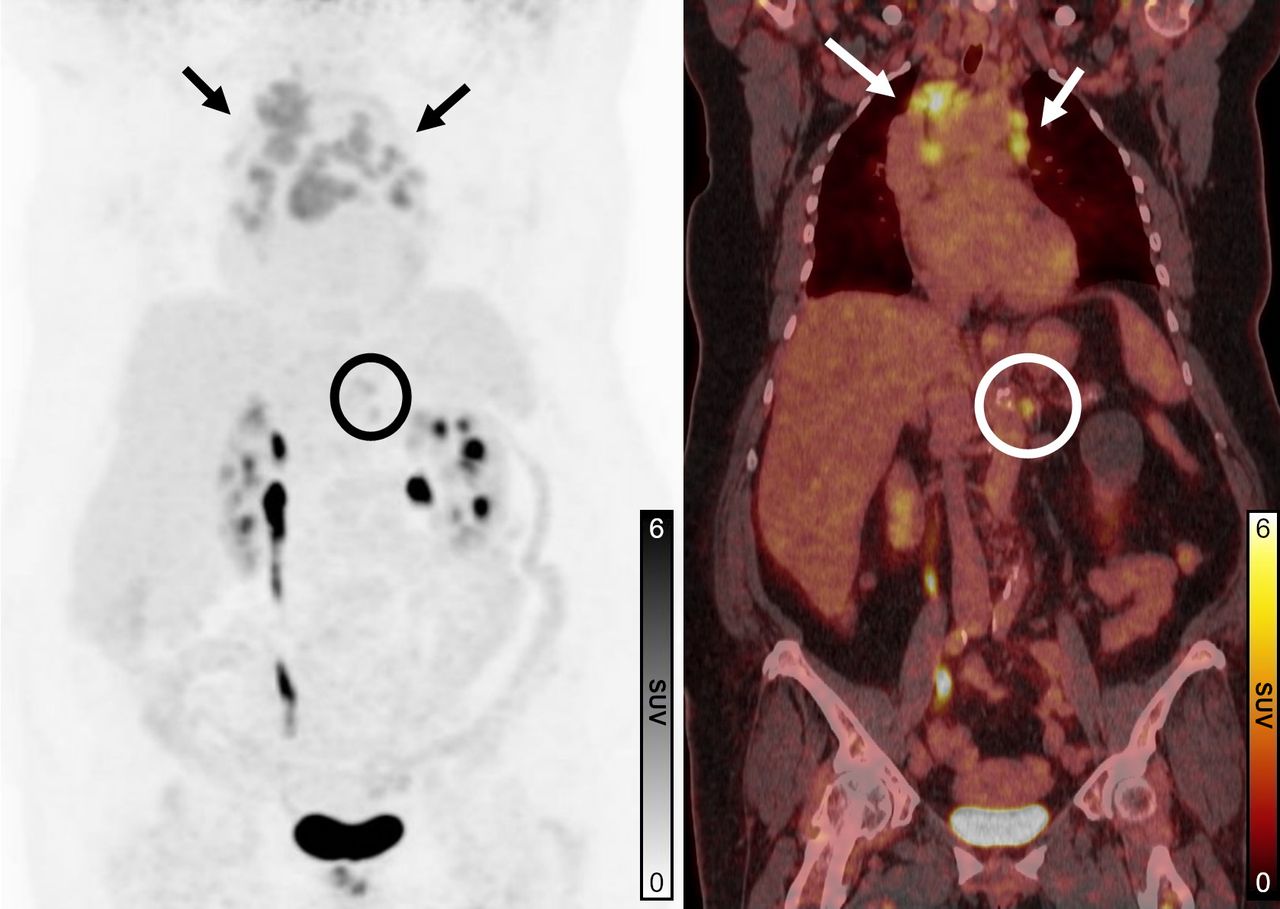
- FIGURE 6.
Scan 2 18F-FDG maximum-intensity projection (left) and 18F-FDG PET/CT fused coronal (right) images. Persistent 18F-FDG–avid bilateral mediastinal and hilar/perihilar adenopathy is visualized from known extracardiac sarcoidosis (arrows). Solitary 18F-FDG–avid left upper abdominal node is suspicious for additional sarcoid involvement (circles).
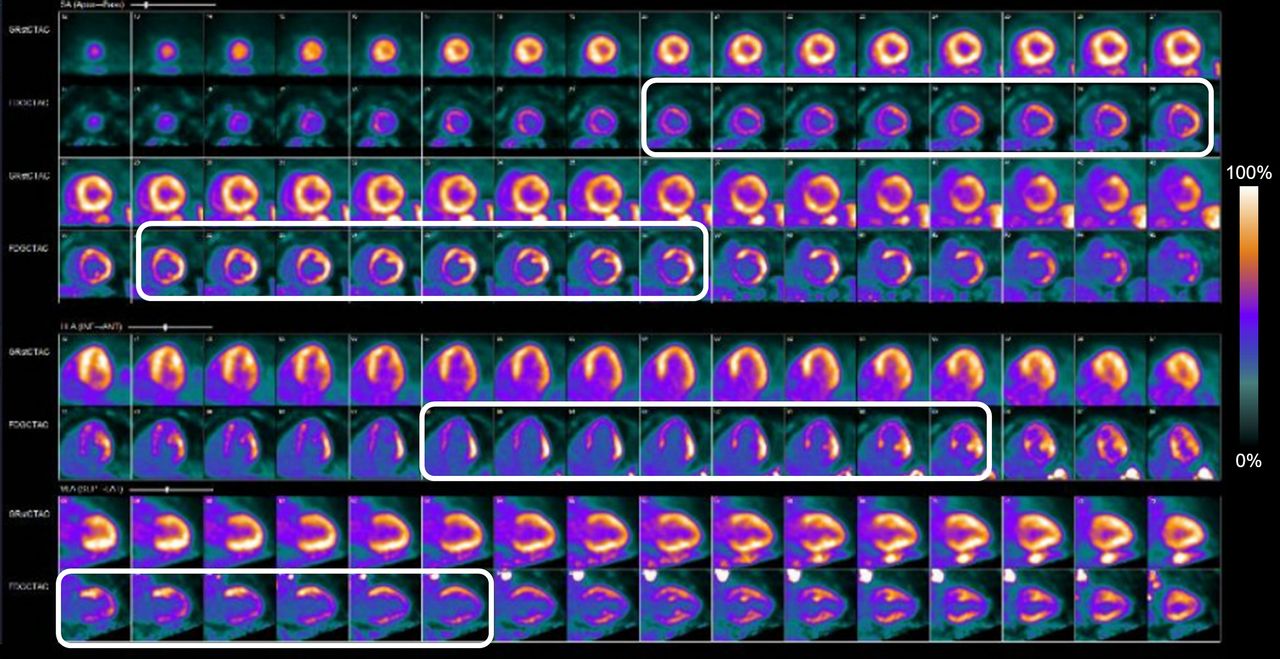
- FIGURE 7.
Scan 3 82Rb-chloride rest perfusion (top rows) and 18F-FDG cardiac metabolism (bottom rows). Rest MPI shows no significant perfusion defects in LV. 18F-FDG PET images show diffusely increased myocardial uptake (rectangles), more prominent in lateral wall. This pattern of diffusely increased 18F-FDG cardiac uptake indicates hyperinsulinemic state, suggesting possible inadequate dietary compliance, and limits evaluation of 18FDG-PET images for cardiac sarcoidosis. Gated rest images show estimated LVEF of 24%.
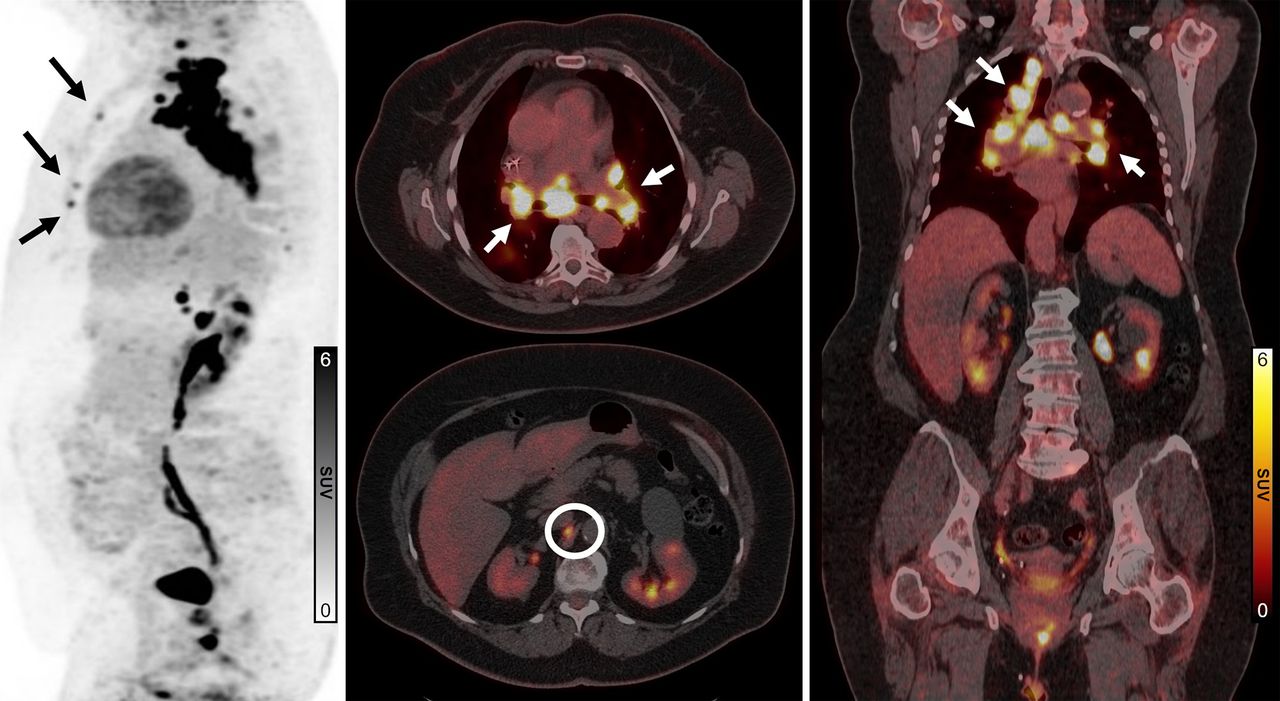
- FIGURE 8.
Scan 3 18F-FDG sagittal maximum-intensity projection (left), 18F-FDG PET/CT fused axial (middle), and 18F-FDG PET/CT fused coronal (right) views. Images show mediastinal, supraclavicular (white arrows), and retroperitoneal (circle) hypermetabolic lymphadenopathy with new or enlarged lymph nodes since scan 1, consistent with sarcoidosis with possible involvement of bilateral ribs (black arrows).
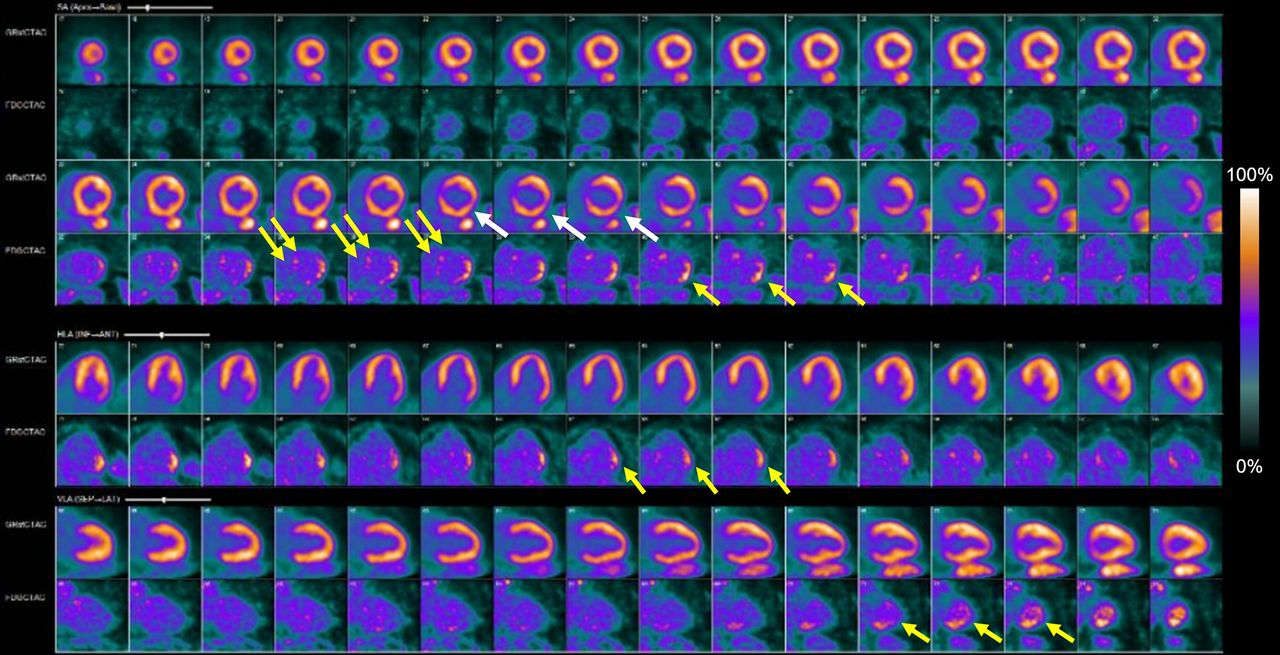
- FIGURE 9.
Scan 4 82Rb-chloride rest perfusion (top rows) and 18F-FDG cardiac metabolism (bottom rows). Rest perfusion images show medium-sized mild defect in basal to mid lateral and inferolateral wall (white arrows). Gated rest LVEF was 31%. 18F-FDG images show diffusely suppressed myocardial uptake, indicating adequate dietary preparation. Medium-sized area of increased 18F-FDG uptake is visualized in basal to mid lateral and inferolateral wall (single yellow arrows) similar to scan 2. New small-sized area of mildly increased 18F-FDG uptake is visualized in basal anteroseptal wall (double yellow arrows).
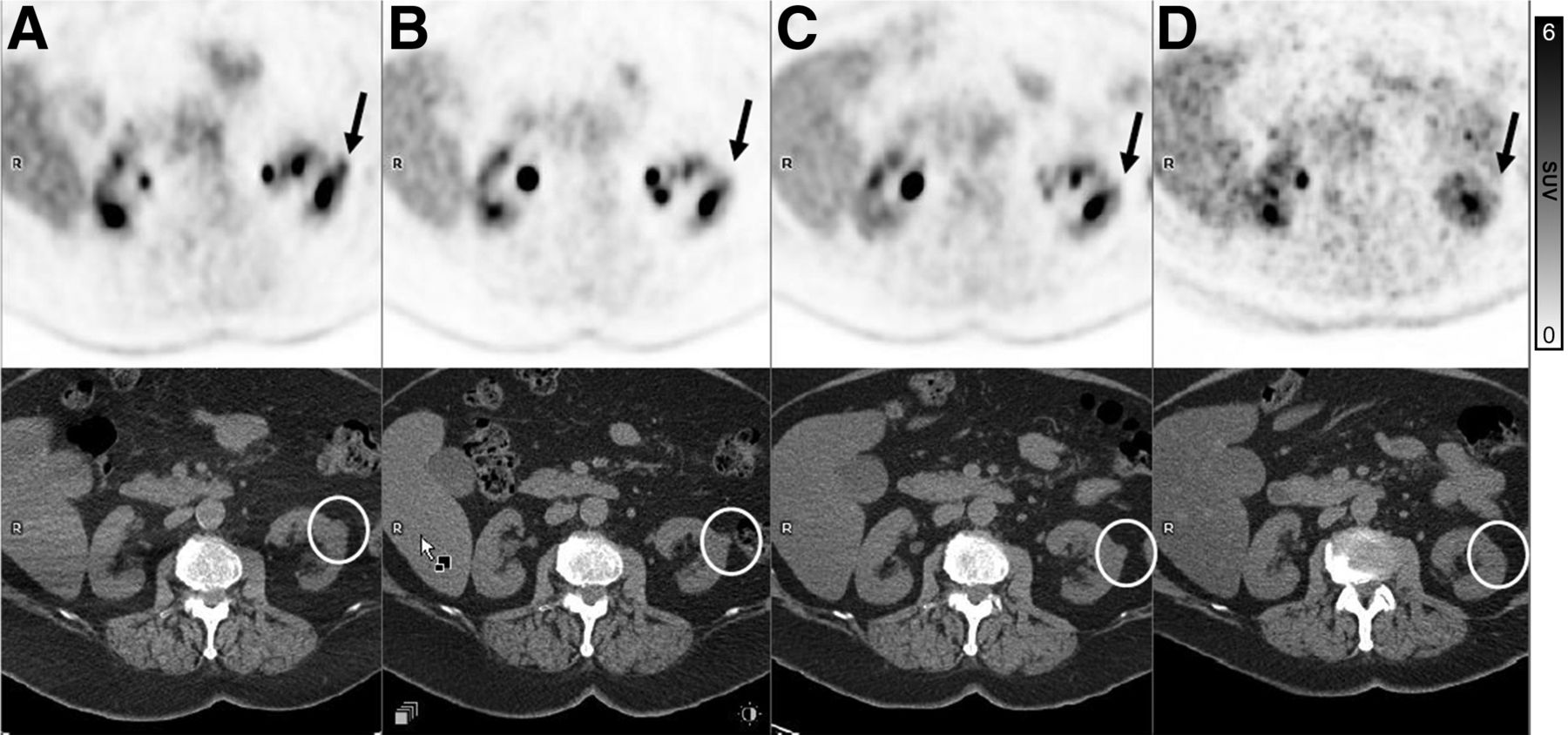
- FIGURE 10.
18F-FDG PET axial (top row) and CT axial (bottom row) images from scan 4 (A), scan 3 (B), scan 2 (C), and scan 1 (D). CT axial images from limited WB 18F-FDG PET/CT scan show incidental 18F-FDG–avid exophytic 1.7-cm isodense nodule in mid left renal pole (circles). This lesion is new since scan 1, has slowly enlarged since most recent examination, and displays increased 18F-FDG activity on scan 4 (arrows).











In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.