


Abstract
We previously reported the 68Ga-labeled prostate-specific membrane antigen (PSMA)-11 and 99mTc-dimercaptosuccinic acid (DMSA) images of the first patient in our prospective research comparing renal 68Ga-PSMA-11 PET with 99mTc-DMSA scanning in adults with pyelonephritis. Here, we present the renal cortical 68Ga-PSMA-11 PET and 99mTc-DMSA images of our second patient, who had chronic recurring pyelonephritis and demonstrated renal parenchymal defects secondary to scarring in the kidney.
Renal cortical imaging with 99mTc-dimercaptosuccinic acid (DMSA) is widely used to detect renal parenchymal changes due to acute pyelonephritis (reduced uptake) and renal sequelae (scars) (absence of uptake) 6 mo after acute infection (1). 99mTc-DMSA scanning is also used to quantify differential renal function, detect various renal abnormalities, and assess the functional status of multicystic kidneys (1). The ability to depict renal scarring via a 99mTc-DMSA scanning is important because scarring is a common cause of hypertension and because extensive scarring can lead to progressive renal impairment and end-stage renal disease (2). The presence of scarring can lead to a change in the treatment plan, such as starting different antibiotics, starting corticosteroids, treating bladder or bowel dysfunction, or performing surgical interventions to prevent further scar formation (3). Potential new treatments such as cyclooxygenase-2 inhibitors, superoxide dismutases, and matrix metalloproteinase-9 inhibitors may also prevent scar formation (3). A nonfunctioning or poorly functioning kidney due to chronic recurrent pyelonephritis may be surgically removed, as it may cause systemic complications such as sepsis, septic shock, and hypertension (2).
68Ga-labeled prostate-specific membrane antigen (68Ga-PSMA) ligands or inhibitors are currently used for initial staging of high-risk prostate cancer and, in cases of biochemical recurrence, for identifying the site of recurrence (4–6). These radiotracers also exhibit high physiologic uptake in the renal cortex. PSMA is a type II transmembrane protein, also known as glutamate carboxypeptidase II or folate hydrolase, which is found mainly in prostate tissue and is overexpressed in prostate cancer, in some extraprostatic normal tissues such as the kidneys and salivary glands, and in various other malignancies (7–9). Immunohistochemical analyses demonstrated detectable PSMA levels in the brush borders and apical cytoplasm of a subset of proximal renal tubules (7,10). The reason for the presence of PSMA in the renal proximal tubules is unknown but may be due to folate metabolism—that is, potential reuptake of folate in the kidneys (11).
We previously published 68Ga-PSMA-11 PET images of the renal cortex of prostate cancer patients with and without cortical defects caused by various sizes of cysts (2,12,13). Given the high renal cortical uptake and excellent renal parenchymal distribution of 68Ga-PSMA-11, we started a prospective research study comparing renal 68Ga-PSMA-11 PET with 99mTc-DMSA scanning in adults with pyelonephritis. Our study was interrupted by the coronavirus disease 2020 Pandemic, but renal 68Ga-PSMA-11 PET and 99mTc-DMSA images of our first patient have been published (14). In our first patient, neither 68Ga-PSMA-11 PET nor 99mTc-DMSA scanning showed cortical defects, but 68Ga-PSMA-11 PET demonstrated image quality superior to that of 99mTc-DMSA scanning. In the current report, we present renal 68Ga-PSMA-11 PET and 99mTc-DMSA images of our second patient, who demonstrated cortical defects caused by scars.
MATERIALS AND METHODS
Our prospective study was approved by the Ethical Committee of the Health Sciences Center at Kuwait University and the Kuwait Ministry of Health. The study was conducted at Mubarak Al-Kabeer Hospital in Kuwait.
The patient provided written informed consent before the study. We obtained 68Ga-PSMA-11 PET/CT and DMSA images of the kidneys.
68Ga-PSMA ligand (PSMA-11) was radiolabeled at another institute (Radiopharmacy Unit at Kuwait Cancer Control Center) using a 68Ge/68Ga generator and a manual synthesis module (Isotope Technologies Garching).
Renal PET/CT images were obtained on a time-of-flight PET/CT camera (Philips Gemini) 60 min after intravenous injection of 48.1 MBq (1.3 mCi) of 68Ga-PSMA-11. We intentionally used a low activity to reduce the radiation dose to the patient. A low-dose, unenhanced CT scan of the region of the kidneys was obtained for attenuation correction, anatomic localization, and gross anatomic correlation before the PET acquisition (30 mAs, 120 kV, pitch of 0.829, 0.5-s rotation time, 64 × 0.625 collimation, and 5-mm slice thickness). The PET acquisition time was 10 min per bed position for 2 bed positions. Because a low dose of activity was administered, the image acquisition time was longer than usual. The PET images were corrected for attenuation on the basis of the CT data, reconstructed using a standard iterative algorithm, and reformatted into transaxial, coronal, and sagittal slices. Maximum-intensity-projection images were also generated. Because of intense activity in the kidneys, the PET images were reviewed in a low-intensity setting to better assess the renal cortical uptake and distribution. Attenuation-corrected (AC) PET images, uncorrected (non-AC) PET images, PET/CT images, and low-dose CT images were reviewed to assess the anatomic location, size, and morphology of the kidneys; the uptake and distribution of radiotracer in the renal parenchyma; and any parenchymal defects or other abnormalities. Quantification of renal 68Ga-PSMA-11 uptake was also performed. Because of unexpected high splenic uptake in this patient, we could not use automated volume-of-interest analysis with the software we had. We manually drew regions of interest around the kidneys in multiple transaxial slices to calculate the total activity in each kidney. In addition, we measured SUVmax and SUVmean in both kidneys in both normal areas and areas with a parenchymal defect by placing a spheric region of interest over the renal cortex without exceeding the renal border.
Four days after PET imaging, 99mTc-DMSA images were obtained 3 h after intravenous injection of 111 MBq (3 mCi) of 99mTc-DMSA using a Symbia S SPECT scanner (Siemens) equipped with a high-resolution parallel-hole collimator. Multiple planar images were obtained in anterior, posterior, right posterior oblique, and left posterior oblique projections (10 min each, with a 20% window centered at 140 keV, a 256 × 256 matrix, and a zoom of 1.3). SPECT images of the kidneys were also obtained (a 20-s acquisition per view, 60 views, a 360° rotation, a 128 × 128 matrix, no zoom, and a 20% window centered at 140 keV). A standard iterative algorithm was used for image reconstruction. Images were reformatted into transaxial, coronal, and sagittal views. Uptake for each kidney was quantified using anterior and posterior planar images and the geometric mean.
RESULTS
The patient was a 49-y-old woman with a history of recurring pyelonephritis over the previous 14 mo. The last episode was a severe emphysematous pyelonephritis that occurred 2 mo before the current study (positive urine culture for Candida albicans) and was treated with antibiotics for 1 mo as an inpatient treatment. At the time of the study, the patient did not have any symptoms and urine cultures were negative. Renal ultrasound performed a month before the study demonstrated a dilated left renal pelvis and calyces with stones, preserved cortical thickness, and corticomedullary differentiation.
Planar and SPECT 99mTc-DMSA images demonstrated cortical defects, reduced uptake, and cortical irregularity in the upper and lower poles of the left kidney (Fig. 1). In the right kidney, no cortical defects were identified, with only slightly reduced uptake in the upper and lower poles, which could be a normal finding.
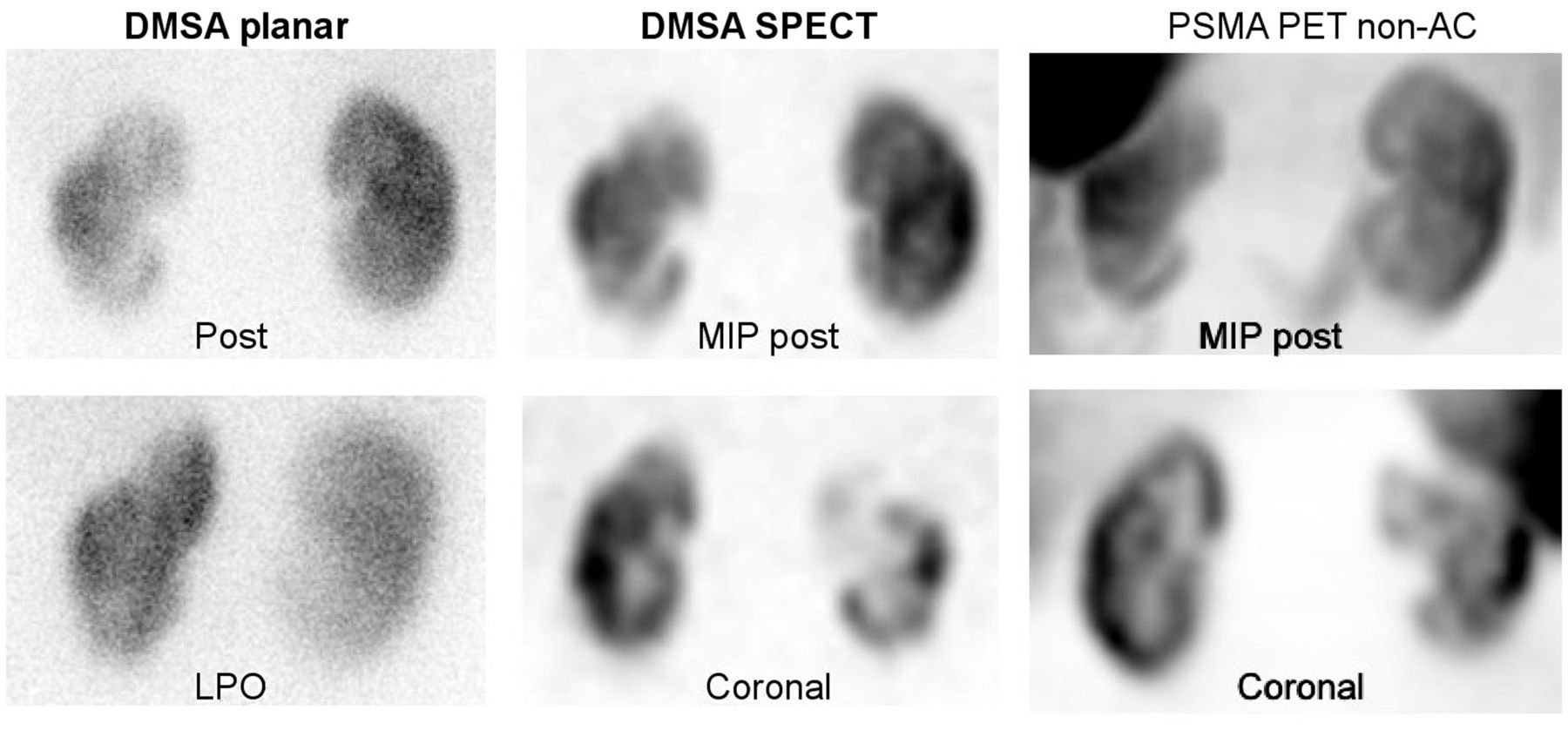
99mTc-DMSA planar (posterior and left posterior oblique), 99mTc-DMSA SPECT (maximum-intensity projection in posterior view and selected coronal slice), and 68Ga-PSMA-11 (non-AC maximum-intensity projection in posterior view and non-AC selected coronal slice) images demonstrating cortical defects or scars and reduced uptake in upper and lower poles of left kidney. Non-AC PET can be seen to have higher resolution than non-AC SPECT. LPO = left posterior oblique; MIP = maximum-intensity projection.
In the upper pole of the right kidney, the AC PET images had an artifact that seemed secondary to some possible unilateral patient motion that occurred as the patient passed urine during imaging. AC PET also showed reduced uptake and cortical defects in the upper and lower poles of the left kidney (Fig. 2). Splenic uptake was higher than usual in this patient, likely because of 68Ga-colloid formation. In the normal physiologic distribution of 68Ga-PSMA-11, splenic uptake is much lower than renal uptake and does not interfere with image interpretation (Fig. 3).
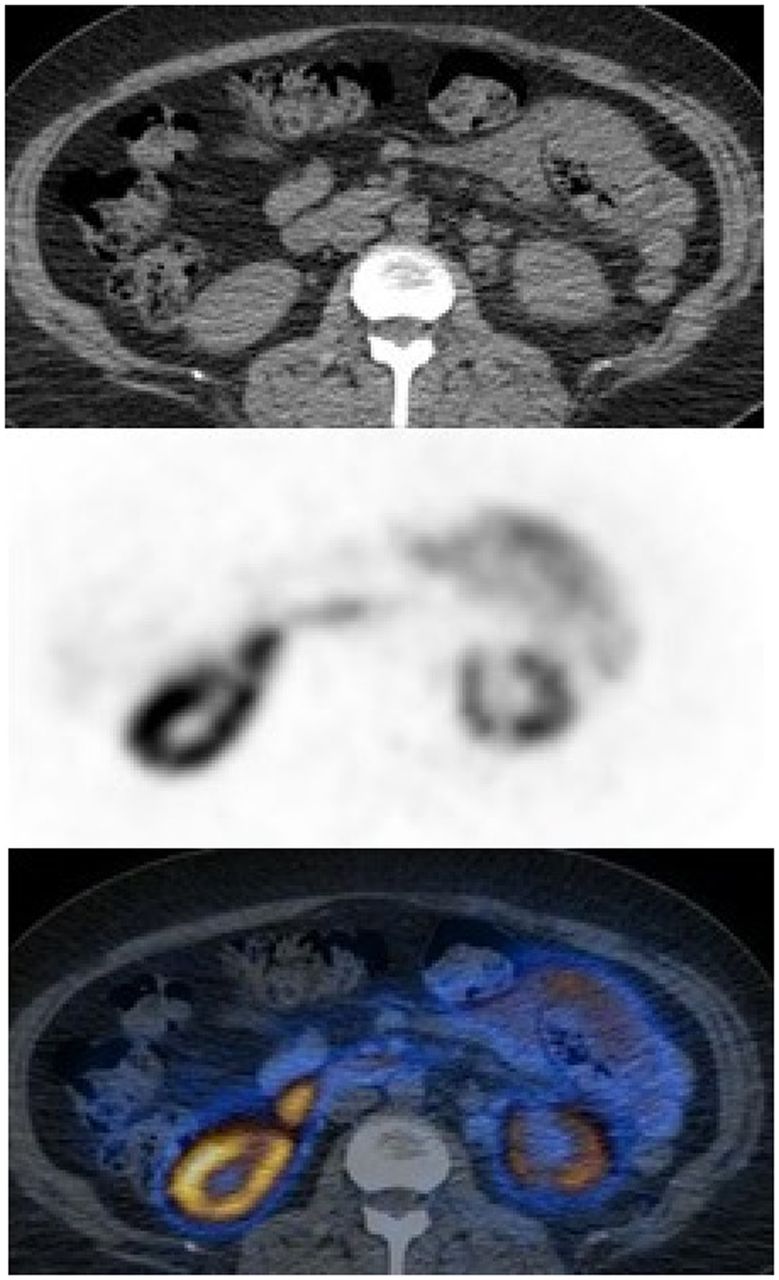
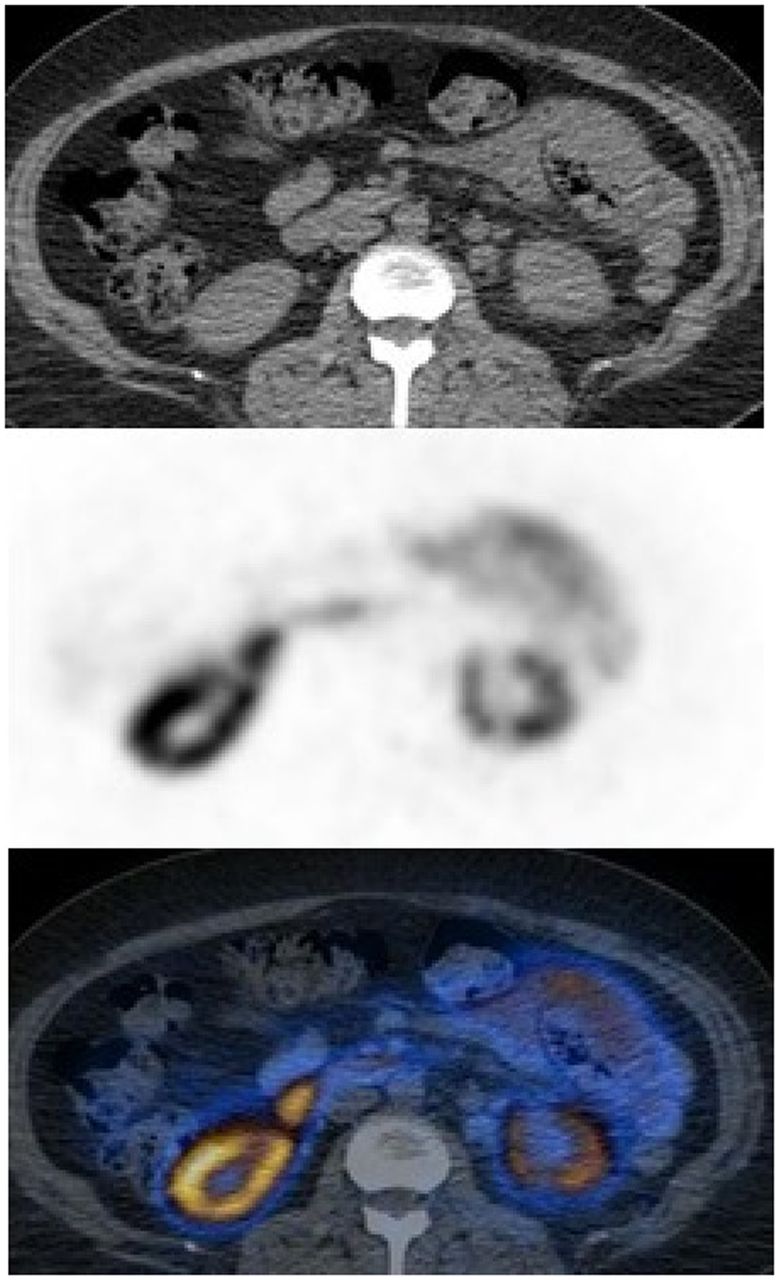
68Ga-PSMA-11 PET/CT (selected transaxial CT [top], PET [middle], and AC PET/CT [bottom]) images demonstrating reduced uptake in lower pole of left kidney and small cortical defect.
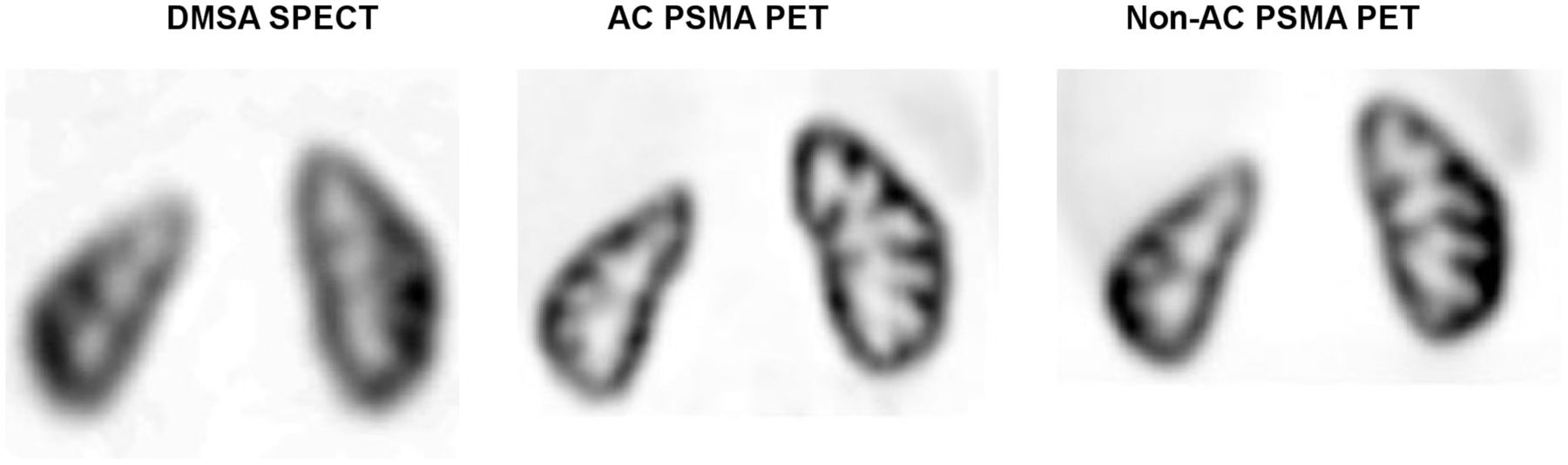
99mTc-DMSA SPECT (selected coronal slice) and 68Ga-PSMA-11 PET (AC and non-AC selected coronal slices) images of another patient with history of chronic recurrent pyelonephritis demonstrating mildly reduced uptake and cortical thinning in upper pole of right kidney with no parenchymal defects. Normal distribution of 68Ga-PSMA-11 is seen, with only mild activity in liver and spleen.
Non-AC PET images demonstrated similar findings to 99mTc-DMSA images, with cortical defects, reduced uptake, and irregularity in the upper and lower poles of the left kidney (Fig. 1). In the upper and lower poles of the right kidney, there was mildly reduced uptake similar to that on 99mTc-DMSA images. Bowel activity in the left upper quadrant did not affect the assessment of the left kidney but caused some overlap on the left kidney on maximum-intensity-projection images. Low-dose CT demonstrated small calculi in the lower pole of the left kidney. There were no cysts in the kidneys on low-dose CT.
Renal uptake was 35.5% on the left and 64.5% on the right with 99mTc-DMSA and 34.5% on the left and 65.5% on the right with 68Ga-PSMA-11.
SUVmax and SUVmean were 53 and 43, respectively, in the normal right-kidney parenchyma. In the left kidney, SUVmax and SUVmean were 6.4 and 4, respectively, for the upper pole; 21.6 and 17.6, respectively, for the lower pole; and 52 and 41, respectively, for the mid cortical region.
DISCUSSION
99mTc-DMSA scanning is the current gold standard to assess the renal parenchyma and detect renal scarring, as has been described in detail in our recently published articles (2,12–14). Identification of renal scarring in patents with pyelonephritis is important because scarring is a common cause of hypertension and extensive scarring can cause progressive loss of renal function (2). In the management of patients with scarring due to pyelonephritis, further scarring might be prevented by a change in treatment plan, such as starting different antibiotics, supporting with other medications, treating bladder and bowel dysfunction, or performing surgical intervention (correcting vesicoureteral reflux) (3). Potential new treatments may also prevent further scar development (3).
There is a shortage of DMSA cold kits in various countries, including the United States, and 99mTc-DMSA was therefore added to the drug-shortages list of the U.S. Food and Drug Administration in 2014 and has been commercially unavailable since then (15). Currently, there is not a good alternative to 99mTc-DMSA scanning. 99mTc-glucoheptonate is only partially concentrated in the kidneys and then is excreted in the urine (1). 68Ga-alizarin red S was studied in animals and humans as a renal cortical PET radiotracer in the 1980s but was not used after that time (16). In a recent metaanalysis study, we compared 99mTc-DMSA scanning with MRI and found MRI and 99mTc-DMSA scanning to have overall equivalent sensitivity in detecting parenchymal changes in pyelonephritis, particularly in scar detection (17). MRI also has certain limitations and is not commonly in routine use to assess patients with pyelonephritis (18). We need new radiotracers, particularly PET tracers, that can selectively accumulate in the renal parenchyma and, compared with 99mTc-DMSA scanning, provide higher-resolution images of the kidneys, detect smaller cortical defects, and better quantify split renal function.
In our current patient, both 68Ga-PSMA-11 PET (AC and non-AC) and 99mTc-DMSA scanning demonstrated cortical defects or scars in the left kidney with comparable image quality. Because of high splenic uptake from 68Ga-colloid formation and some motion-related artifacts in the right kidney, image quality in our current patient was lower than in our previously reported patient (Fig. 3) (14). During the labeling procedure, formation of 68Ga-colloid may occur and 68Ga-colloid will accumulate in the spleen, liver, and bone marrow (19). Thin-layer chromatography is used to measure colloid content. We did not repeat the 68Ga-PSMA-11 PET study in this patient because we did not want our patient to receive additional radiation exposure. Despite splenic uptake and some motion on the right side, AC and non-AC images successfully demonstrated scars in the left kidney.
Previously reported studies have demonstrated a good correlation between renal 99mTc-DMSA uptake and renal function tests such as effective renal plasma flow, glomerular filtration rate, and creatinine clearance (20–24). In our recently submitted retrospective study on 25 prostate cancer patients (Jan Henning Schierz et al., unpublished data, 2021), renal 68Ga-PSMA-11 uptake appeared to correlate well with the results of renal function tests (creatinine and glomerular filtration rate).
There are certain advantages of 68Ga-PSMA-11 PET over 99mTc-DMSA scanning, such as a shorter waiting time after injection (1 h vs. 3 h), a shorter half-life (68 min vs. 6 h), and superior image quality, particularly with AC PET. The image acquisition time for our current patient was 20 min with 68Ga-PSMA-11 PET because we used a low dose of activity to reduce the radiation dose to the patient (2 bed positions, 10 min per bed position, 48.1 MBq [1.3 mCi]). The image acquisition time for DMSA scanning was 55 min (30-min planar, 25-min SPECT). A longer acquisition time can cause patient discomfort and patient motion and result in image artifacts, requiring additional images and sedation in pediatric patients. The image acquisition time with 68Ga-PSMA-11 PET can be further reduced to 6–7 min per bed position for 74 MBq (2 mCi), 4–5 min per bed position for 111 MBq (3 mCi), and 2–3 min per bed position for 148 MBq (4 mCi), but the kidney and effective doses will increase with higher activities. As we reported in our previous articles, absorbed adult kidney doses of 68Ga-PSMA-11 and 99mTc-DMSA are 0.24 and 0.18 mGy/MBq, respectively, and effective adult doses are 0.022 and 0.0088 mSv/MBq, respectively (25,26). In our previously reported patient, estimated effective doses of 111 MBq (3 mCi) of 99mTc-DMSA and 74 MBq (2 mCi) of 68Ga-PSMA-11 were 0.98 and 1.63 mSv, respectively. In our current patient, 48.1 MBq (1.3 mCi) of 68Ga-PSMA-11 yielded an effective dose of 1.05 mSv, which is similar to the effective dose of 99mTc-DMSA. The additional radiation dose from CT in PET/CT is low because it is a low-dose CT scan and covers only the region of the kidneys. Non-AC PET also provides high-quality images of the renal parenchyma as seen in our current patient and in previous reports, and low-dose CT can therefore be omitted.
PET/CT cameras provide higher-resolution images than standard γ-cameras. In our patient, even low-dose non-AC PET provided images higher in quality than—or comparable in quality to—99mTc-DMSA SPECT. SPECT/CT provides higher-resolution images than SPECT, but we intentionally did not perform SPECT/CT on our patient to reduce the radiation dose in this research patient. Overall, PET/CT is known to provide higher-resolution images than SPECT/CT. On the other hand, SPECT systems with cadmium-zinc-telluride detectors have better resolution than conventional scanners with sodium iodide detectors (27).
The use and availability of 68Ga-PSMA ligands for prostate cancer have been increasing. Recently, 68Ga-PSMA-11 has been approved by the Food and Drug Administration for prostate cancer imaging. One limitation of 68Ga-PSMA-11 PET is that it costs more than 99mTc-DMSA scanning: approximately $450 and $300, respectively, in our institute.
Quantification of uptake for each kidney showed results similar to those of 99mTc-DMSA scanning and 68Ga-PSMA-11 PET. Because of high splenic uptake and limitations in our software, we could not perform automated volume-of-interest analysis on PSMA images, but in our recently submitted study, automated volume-of-interest analysis successfully provided total counts, volume, and SUVs for each kidney.
In our current patient, and in our previous patient with chronic pyelonephritis, 68Ga-PSMA-11 PET appears to be a potential alternative to 99mTc-DMSA scanning. As discussed for our previous patient, its biodistribution and radiation dose in the pediatric population are not known, and further work is required to understand its mechanism of uptake, to determine the optimal injected activity, and to determine its dosimetry before its use as a renal cortical tracer can be supported.
CONCLUSION
The renal cortical scars caused by pyelonephritis were demonstrated well by 68Ga-PSMA-11 PET.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENT
68Ga-PSMA ligands are investigational PET radiotracers and as of now have not been approved by the U.S. Food and Drug Administration or European Medicines Agency. This article is about off-label use of 68Ga-PSMA-11 for renal PET/CT imaging in adults.
Footnotes
Published online July 30, 2021.
REFERENCES
- Received for publication April 8, 2021.
- Revision received May 20, 2021.





{kind=link}
{kind=link}
{kind=link}