


Rationale
Technegas (Cyclomedica Asia Pacific) is a versatile yet straightforward system for producing high-quality 99mTc-based ventilation studies using a carbon-based nanoparticle. Because Technegas is neither a gas nor produces aerosolized particles, it optimizes patient outcomes while maintaining staff safety. Technegas allows the protocol to move to 3-dimensional SPECT imaging with improved sensitivity and specificity (1–3). The nature of Technegas allows optimal ventilation imaging with good peripheral penetration, simple operation, efficient delivery, low radiation dose, and slow washout.
Clinical Indications
The primary clinical indication for Technegas ventilation is in conjunction with 99mTc-macroaggregated albumin perfusion lung imaging to evaluate suspected pulmonary embolism. In addition, Technegas ventilation imaging is used in evaluating chronic thromboembolic pulmonary hypertension, asthma, chronic obstructive pulmonary disease, emphysema, and quantitation before lung volume reduction surgery.
Contraindications
Technegas has no known contraindications.
Patient Preparation/Education
The key to successful Technegas delivery is patient compliance, achieved through patient education and practice, which should not be rushed. A detailed explanation of the ventilation process at a language level that the patient understands, with ample clarification and questions, is essential. The practice run should be done under the same conditions as the actual ventilation procedure, including position (upright or supine) and the nose peg. The practice session improves timing, ventilation, and patient compliance (especially with seals) and offers the opportunity to select the appropriate mouthpiece for that patient.
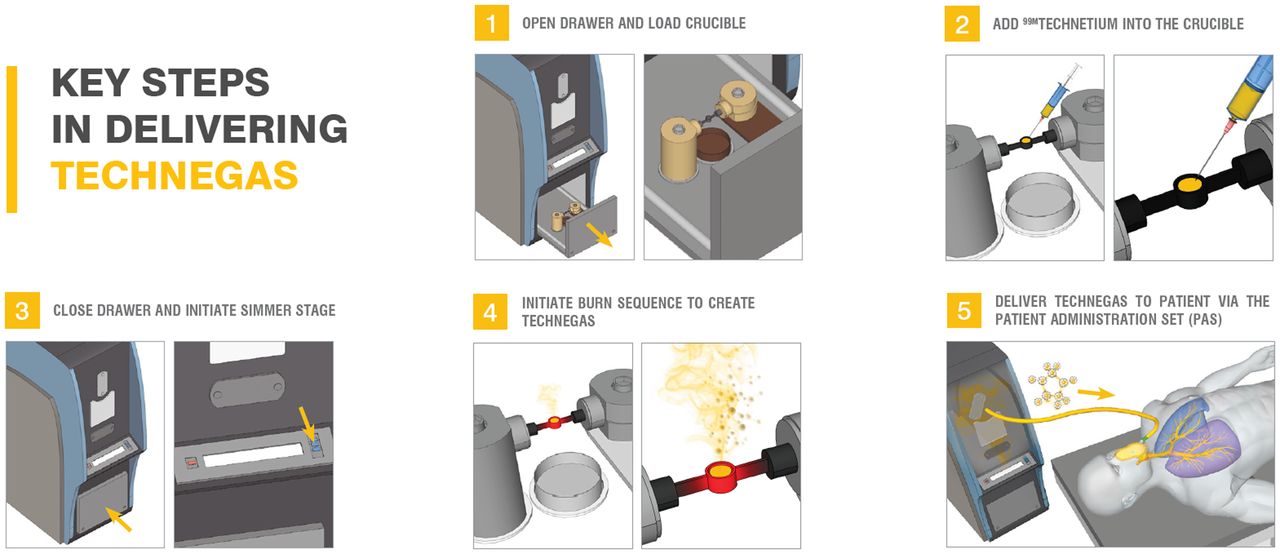
Technegas Preparation (4)
Prepare the system:
Connect and turn on the argon supply to a 15 L/min flow rate.
Connect to main power supply and switch on.
Press the open button to open the chamber.
Prepare the crucible (Fig. 1):
Using gloves and forceps, clear debris from the chamber and ash tray.
Wet the well of a new crucible with ethanol and drain but do not allow it to dry.
Use forceps to place the crucible between the chamber contacts, and ensure good contact by rotating forward and backward. Take care not to twist or fracture the crucible.
Add 200–900 MBq of 99mTc in 0.13–0.17 mL with the well vertical, but do not overfill the crucible.
Depress and hold the draw interlock and the close button until the chamber is completely closed.
Simmer (Fig. 1):
Press start to initiate the 6-min simmer cycle.
Prepare the patient, and practice the breathing technique required during the simmer cycle.
If the concentration of 99mTc is low and requires a top-up, press cancel twice at the end of the simmer process to allow the draw to be opened and additional 99mTc added to the well. Do not wet with ethanol for the reload. Close the chamber and reinitiate the 6-min simmer cycle.
Burn (Fig. 1):
Press the start button to initiate the 15-s burn.
Verify the burn and then disconnect the mains and argon.
Transport the Technegas generator to the patient.
Administer the Technegas within the 10-min window.
Ventilate the patient (Fig. 1):
Attach the patient administration set to the Technegas generator.
Commence the practiced breathing strategy with the patient.
Press the start button.
On inspiration, depress the patient delivery knob.
Monitor the lung count rate.
When the required count rate is achieved, release the delivery knob and allow the patient to take 4–5 breaths through the tube to clear the residual.
Dispose of the patient administration set.
Return the Technegas generator to argon and main power supply, which will automatically commence a purge.
Commence the ventilation imaging protocol.
Acquisition Parameters
Ventilation acquisition protocols vary among departments. Planar-only supine protocols generally use a high-resolution collimator and a 256 × 256 pixel matrix for 300,000–500,000 counts in 8 projections, listed here as dual-head projection pairs: anterior/posterior, left anterior oblique/right posterior oblique, right anterior oblique/left posterior oblique, and right lateral/left lateral. The corresponding perfusion study would adopt the same parameters with higher total counts of 800,000–1,000,000 per image. Alternative SPECT approaches are performed supine with the arms extended above the head. The ventilation time per projection is typically 12–15 s, whereas the perfusion is generally 8–10 s. Otherwise, ventilation and perfusion SPECT are usually performed with a 128 × 128 matrix using high-resolution collimation and a noncircular (elliptic or contoured) orbit with projections every 3° (120 projections). CT may be performed with the SPECT and can be low-dose, nondiagnostic CT for attenuation correction, diagnostic CT, or a CT pulmonary angiogram.
Image Processing
Planar data should be displayed, thresholded, and annotated with corresponding ventilation and perfusion images. SPECT data should undergo ordered-subset expectation maximization iterative reconstruction with a 3-dimensional Butterworth filter. Coregistration with the CT scan should be performed for attenuation correction, anatomic localization, and, if appropriate, fusion of contrast angiographic data.
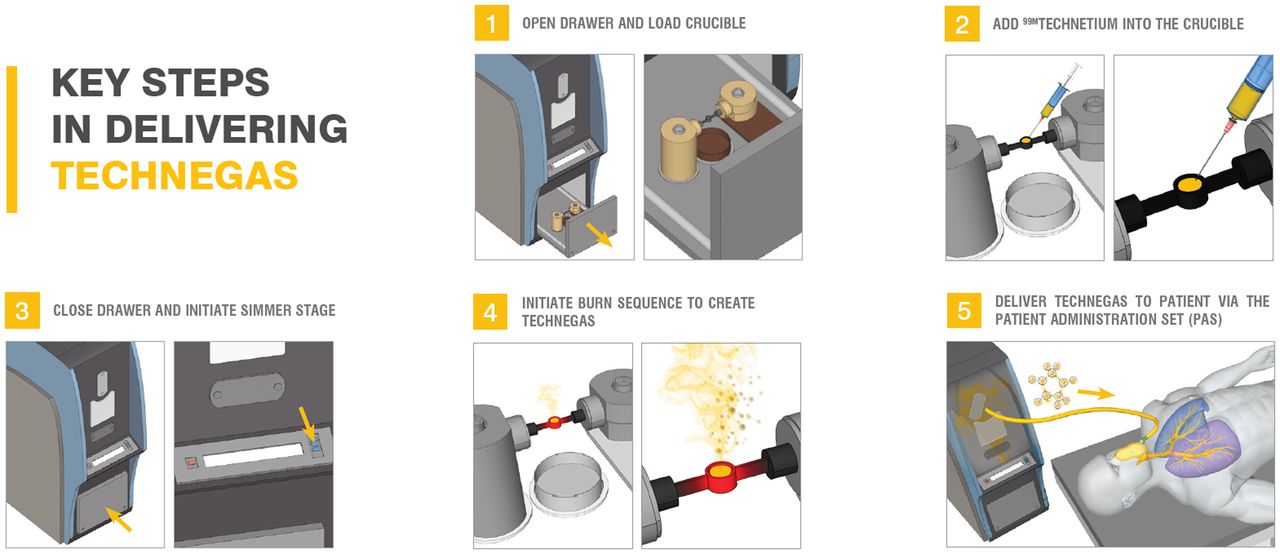
The 5 basic steps in delivering Technegas to patients. (Courtesy of Cyclomedica.)





{kind=link}