


Abstract
Rotor syndrome (RS) is a benign, inherited, commonly misdiagnosed cause of conjugated hyperbilirubinemia whose identification prevents unnecessary invasive investigations. We present the case of a 3-y-old boy with phenotypic and laboratory findings of RS but negative genetic test results, whose diagnosis was confirmed by hepatobiliary scintigraphy.
Rotor syndrome (RS) is a benign, inherited, commonly misdiagnosed cause of conjugated hyperbilirubinemia (1) whose identification prevents unnecessary invasive investigations. It is characterized by mild conjugated hyperbilirubinemia (2–5 mg/dL); icteric sclera usually presents shortly after birth, and urinary coproporphyrin excretion is elevated (2). Genetic diagnosis reveals a homozygous inactivation of SLCO1B1 and SLCO1B3 genes (3). We present the case of a 3-y-old boy with phenotypic and laboratory findings of RS but negative genetic test results, whose diagnosis was confirmed by hepatobiliary cholescintigraphy (HBS).
CASE REPORT
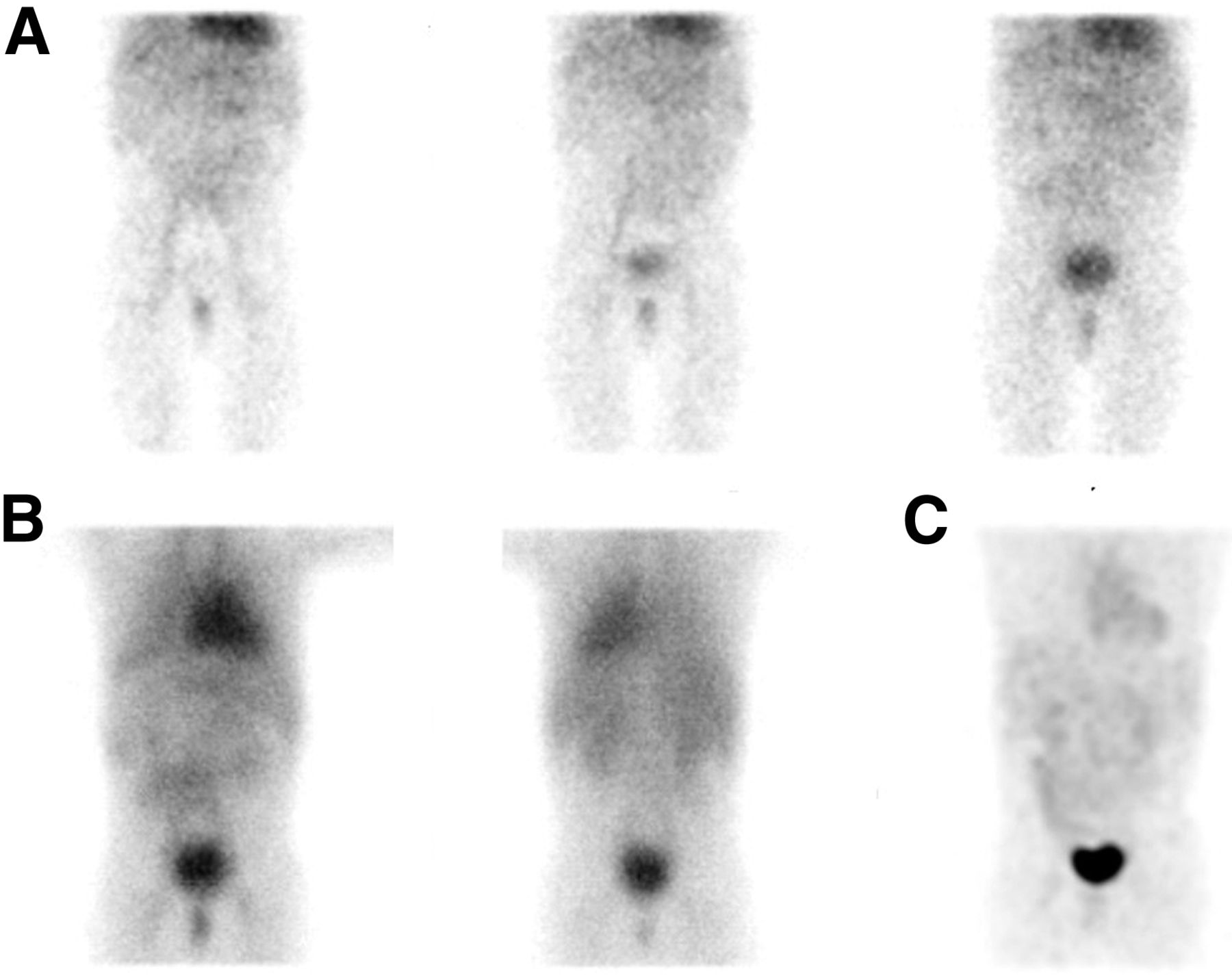
A 3-y-old boy presented with persistent jaundice since birth. The physical examination was unremarkable, except for mild icterus of the sclerae. Serum total biliburin was elevated (2.59 mg/dL), with a conjugated fraction of 2.41 mg/dL. The results of liver function tests, abdominal ultrasound, serology for viral and autoimmune hepatitis, and tests for genetic disorders, such as cystic fibrosis and Wilson disease, were normal. Additional investigation revealed elevated coproporphyrin I (97 nmol/L; reference range, <40 nmol/L) and III (109 nmol/L; reference range, <75 nmol/L). Eventually, the patient underwent HBS after intravenous injection of 45 MBq of 99mTc-mebrofenin, according to the European pediatric dosage card (version 5.7.2016). During dynamic acquisition of data, the perfusion phase (2 s/frame for 60 s) was normal, whereas the following data (1 min/frame for 60 min) were significantly abnormal. No succession of the normal scintigraphic phases (hepatic, biliary, and intestinal) was noticed, as 99mTc-mebrofenin liver uptake was too slow (Fig. 1A). The biliary duct system and gallbladder were not seen, whereas a faint visualization of the liver and small bowel was more evident on the delayed static images (Figs. 1B and 1C). In contrast, an extremely prolonged blood-pool phase (visualization of the heart and spleen) and prominent renal excretion, mimicking liver failure, were noticed.

Abnormal 99mTc-mebrofenin hepatobiliary scintigraphy findings consistent with RS in 3-y-old boy. (A) Left to right: 10th-, 30th-, and 50th-minute frames of dynamic acquisition. (B) Delayed static images at 1.5 h (anterior [left]/posterior [right]). (C) Delayed maximum-intensity-projection 3-dimensional anterior reconstructed image at 3 h.
A molecular genetic analysis with next-generation sequencing was performed, but no sequence of the SLCO1B1 and SLCO1B3 genes involved in RS was detected. During a follow-up of 2 y, the patient had a favorable clinical course without any complications.
DISCUSSION
HBS is an inexpensive and straightforward method and represents the imaging test of choice for RS, allowing accurate differential diagnosis (3). Even without considering clinic–laboratory findings, this too-faint hepatic visualization, although suggestive of hepatocellular disease, is unlikely to be consistent with cirrhosis or hepatitis. The abnormal, instead of normal, hepatic perfusion phase (increased or anticipated) due to liver arterialization is more likely in these disorders. Dubin–Johnson syndrome, a similar syndrome of conjugated hyperbilirubinemia, presents, in contrast, HBS findings of intrahepatic cholestasis (no biliary phase, associated with prolonged, rapid, and intensive, instead of slow and negligible, liver radiotracer uptake) (3,4).
Concerning the genetic diagnosis of RS, SLCO1B1 and SLCO1B3 genes are essential, as they provide instructions for making proteins, called organic anion transporting polypeptide 1B1 (OATP1B1) and organic anion transporting polypeptide 1B3 (OATP1B3), that are expressed in the sinusoidal membrane of hepatocytes and ensure the reabsorption of conjugated bilirubin from the blood into the liver (3). In RS, the homozygous inactivation of both genes results in nonfunctional or absent proteins and increased bilirubinemia and porphyrinuria (3,5).
Our case, because of the clinical, laboratory, and HBS findings, was considered to be affected by RS and most likely represents the first report of a case without sequences from the 2 known genes associated with RS.
CONCLUSION
In the rare case of a child with typical RS clinical and laboratory features, the diagnosis of RS might be confirmed only by typical HBS findings and might not require genetic testing, which is an expensive, time-consuming, and, as we can conclude, not always cost-effective diagnostic tool.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 15, 2021.
REFERENCES
- Received for publication September 27, 2020.
- Accepted for publication January 27, 2021.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.