


Abstract
Infection prevention and control practices represent a vital behavioral skill set, especially in the era of COVID-19. Standard precautions, correct use of personal protective equipment, proper hand hygiene, and appropriate cleaning and disinfecting are necessary to prevent health-care–acquired infections in care facilities.
- COVID-19
- standard precautions
- personal protective equipment
- hand hygiene
- health-care–acquired infections
Coronavirus disease 2019 (COVID-19) has brought infection prevention and control into the spotlight as health-care facilities implement specific infection prevention and control procedures to protect staff and patients from the novel virus. COVID-19 proved that emerging infectious diseases pose an ever-present challenge for care providers. To achieve success, infection prevention practices must be coordinated throughout the care continuum and must be inherent behavior. Many of the fundamental infection control practices used in everyday practice are equally important during the pandemic. Therefore, technologists now have an opportune time to review and brush up on best practices for infection prevention and control. This article will provide a basic review of the current recommendations on infection prevention for hospitals, ambulatory care centers, and outpatient clinics.
HEALTH-CARE–ACQUIRED INFECTIONS (HAIS)
HAIs, also referred to as nosocomial infections, are infections acquired by patients when receiving care in a health-care facility such as a hospital, ambulatory care center, outpatient clinic, or doctor or dental office. Over the last decade, infection prevention and control have been at the forefront of the battle to improve health-care quality, as morbidity and mortality statistics are concerning and the economic impact is appalling. The Centers for Disease Control and Prevention (CDC) 2015 HAI Prevalence Survey data revealed that approximately 1 in 31 hospital patients developed at least 1 HAI, resulting in 687,000 HAIs and 72,000 deaths (1). Robust infection prevention education focusing on implementing standard precautions, increased hand hygiene compliance, and proper use of personal protective equipment (PPE) resulted in a 16% reduction in HAIs in 2015 compared with 2011.
Specifically, health-care facilities have worked diligently to arrest central line–associated bloodstream infections, vancomycin-resistant enterococci, Clostridium difficile, methicillin-resistant Staphylococcus aureus, and surgical site infections. The CDC’s National Healthcare Safety Network, the most widely used HAI tracking system, provides data to identify problem areas and measure progress in infection prevention efforts to eliminate HAIs (2). The Healthcare Infection Control Practices Advisory Committee, a federal advisory committee, guides both the Department of Health and Human Services and the CDC on infection control practices and strategies for the surveillance, prevention, and control of HAIs, antimicrobial resistance, and adverse events in U.S. health-care settings (3).
TYPES OF PRECAUTIONS
Transmission-Based Precautions
Transmission-based precautions, used in concert with the standard precautions described below, are implemented when patient infection or colonization is suspected (4). The intent is to isolate and contain the contagion. Transmission-based precautions include placement of the patient in a single room to isolate transmission. Transportation of the patient out of the room should be limited, and the patient should wear a mask when being transported or receiving care. The required PPE for staff includes gown, gloves, and an N95 filtering facepiece respirator (FFR) to limit aerosol transmission risk. Staff and visitor contact with the patient should be limited.
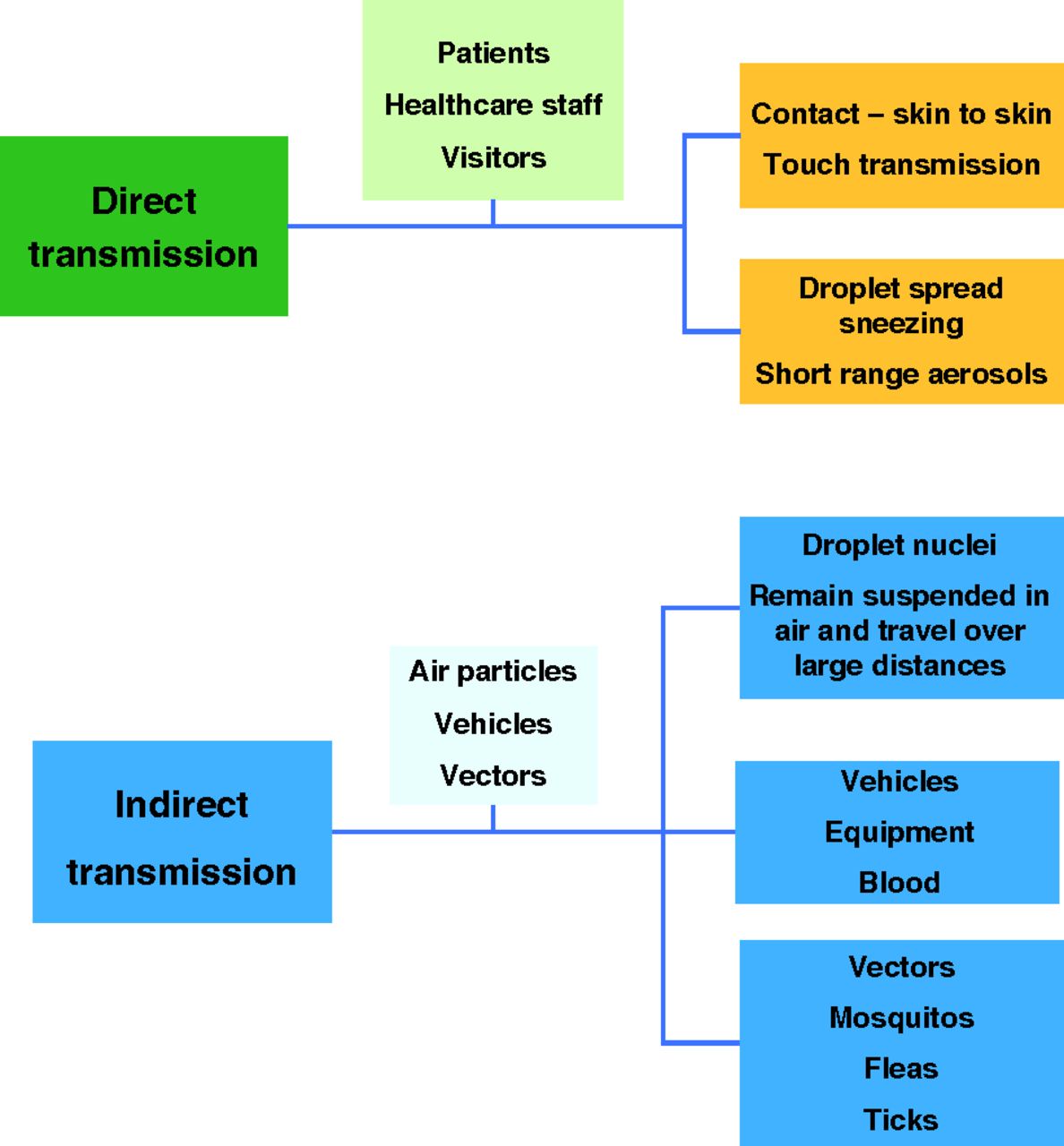
Direct transmission occurs when microbes transfer to a person directly from an infected person instead of from a contaminated intermediate object or person. Blood, body fluids, breaks in the skin, and uncovered sneezing are examples of direct transmission. Droplet transmission results from respiratory droplets emitted from sneezing, coughing, speaking, or respiratory suction procedures. Respiratory droplets travel a short distance and necessitate facial protection.
Indirect transmission involves transfer of the infectious agent through a contaminated intermediate object or person. It is difficult to determine how indirect transmission occurs, but evidence suggests that contaminated hands of health-care workers, as well as patient-care devices such as intravenous pumps, blood pressure cuffs, and instruments, contribute to transmission.
Airborne transmission involves airborne droplet nuclei or small particles that remain in the air and are dispersed over long distances by air currents. Measles and chickenpox are examples of droplet-nuclei airborne transmission (Fig. 1).
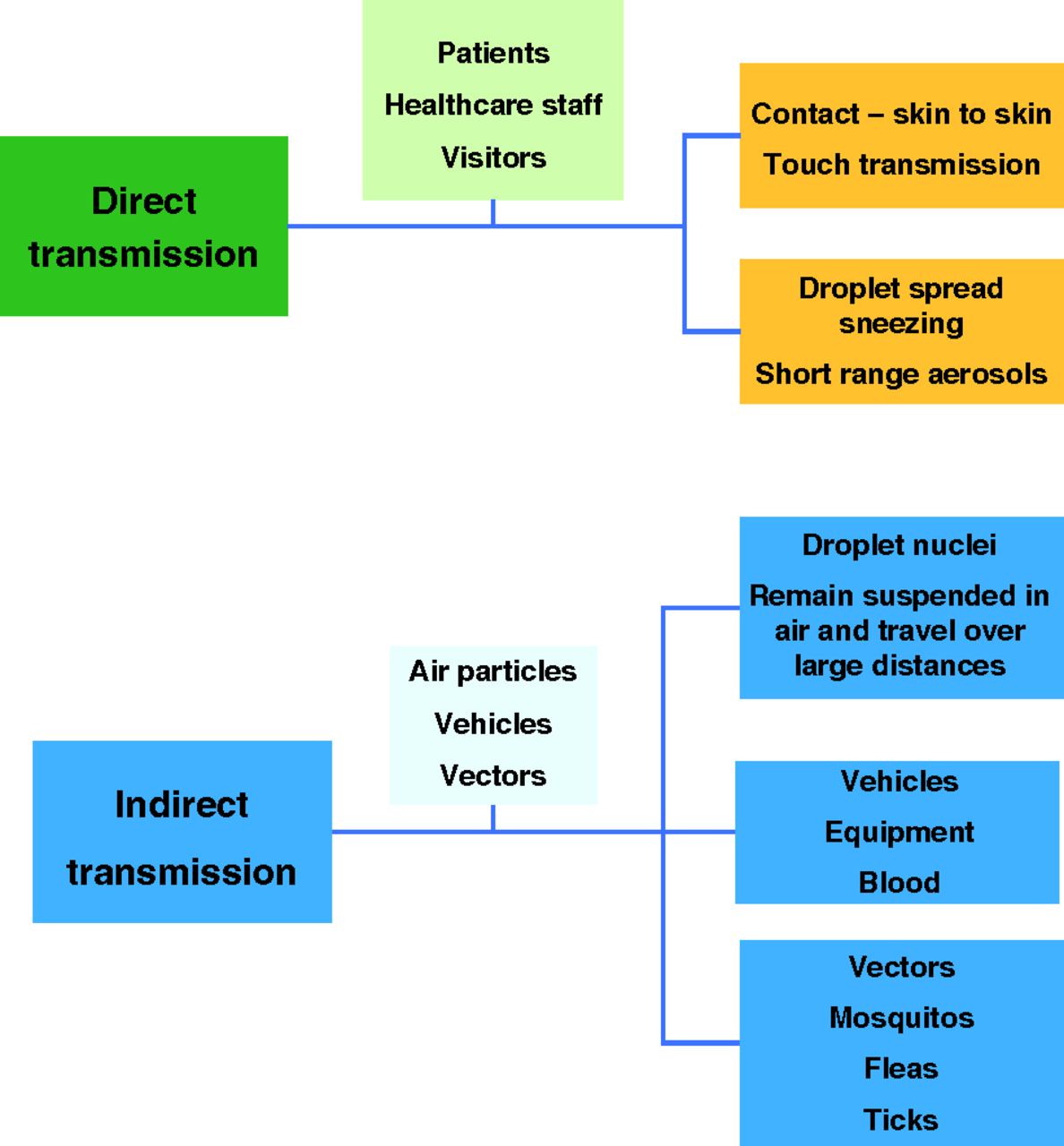
Modes of pathogen transmission. Microbe transmission occurs via 2 primary pathways: direct and indirect.
Standard Precautions
Universal precautions were introduced to health-care workers in 1985 in response to the widespread growth of HIV and the risk of transmission posed by exposure to infected blood from needle sticks. In the 1990s, experts recognized that body fluids also presented a risk for transmission of infectious disease. In response, practices to isolate body substances were proposed. Because a period of confusion followed, enhanced precautions, termed standard precautions, were introduced to reduce the risk of transmission of blood-borne and other pathogens in health-care facilities (5). Standard precautions assume that all blood and body fluids from any patient could be infectious. Standard precautions include use of hand hygiene along with gloves, gowns, masks, eye protection, and face shields.
Hand Hygiene
It is now common knowledge that hand hygiene is a critical component for reducing the spread of pathogens, as hands can be a primary vector for contact transmission of infections. Good hand hygiene practice includes washing with soap and water for 20 s when hands are visibly soiled, before eating, after using the restroom, and after sneezing. Alcohol-based hand rubs, which have greatly improved hand hygiene compliance, containing 60%–95% alcohol are preferred when hands are not visibly soiled. The recommended procedure suggests using a dime-sized drop of alcohol-based hand rub placed in the palm of one hand and then rubbed between both hands, covering the entire surface of the hands and fingers until the hands are dry. Usually, the process takes about 15 s. Alcohol-based sanitizer can inactivate COVID-19 (6).
PPE
The degree of PPE required is determined by the level of clinical interaction with the patient and the risk of transmission (7). Several methods for properly donning and doffing equipment are acceptable; health-care workers should follow their facility’s requirements (Table 1). Health-care workers must don PPE before entering a patient’s room or interacting with a patient to provide care or diagnostic services.
CDC’s PPE Donning and Doffing Recommendations ( 12 )
FACE MASKS
Face Masks Versus N95 FFRs
Health-care workers should understand the difference between a face mask and an N95 FFR. A facemask fits loosely on the face, protecting against large airborne particles, splashes, or sprays of body fluids. It protects the patient from the wearer’s respiratory emissions. It does not provide the same level of protection from inhaling small airborne particles as N95 FFRs. According to title 42 of the Code of Federal Regulations, part 84, N95 FFRs must be compliant with the National Institute for Occupational Safety and Health standards and capable of filtering 95% of large and small airborne particles to reduce exposure to both aerosols and droplets (8). They cover the face and require prefitting to ensure a tight seal around the nose, mouth, and chin. Usually, face masks and N95 FFRs are discarded after one use. However, the COVID-19 virus significantly strained PPE supplies, especially face masks and N95 FFRs. The CDC, National Institutes of Health, and several academic institutions developed processes and guidelines for reuse and decontamination of N95 FFRs.
Mask Reuse
During the intense periods of infection during the COVID-19 pandemic, health-care institutions faced severe equipment shortages and were forced to conserve PPE. In fact, most were at the contingency (expected shortages) and crisis (known shortages) capacities (8). In response, contingency strategies based on the current calculated PPE consumption rate, or burn rate, were developed.
N95 FFR reuse depends on a facility’s supply and surge capacity status. Limited reuse is the practice of using the same N95 FFR for multiple encounters with patients, but it is removed (doffed) after each encounter. Extended reuse is when the same FFR is worn continuously for encounters with multiple patients. The number of times an N95 FFR can be reused depends on the fit, elastic strap integrity, filtration performance, contamination, and damage. The CDC recommends 5 uses per mask as long as the mask fits tightly, ensuring proper performance. Health-care workers should follow their facility’s policy regarding mask reuse.
Decontamination of N95 FFRs
On March 29, 2020, the U.S. Food and Drug Administration issued the first emergency-use authorization for a procedure to decontaminate N95 FFRs. Several subsequent emergency-use authorizations have since been published. Effective decontamination of N95 FFRs reduces the pathogen burden, does not alter the fit or filtration performance, and presents no residual chemical hazard. As of April 2020, ultraviolet germicidal irradiation, vaporous hydrogen peroxide, and moist heat have shown the most promise as potential methods to decontaminate N95 FFRs (9). Many of the decontamination processes developed, tested, and validated are specific for the brand of N95 FFR.
Specific to COVID-19, the National Institutes of Health scientists investigated decontamination procedures for small sections of N95 filter fabric exposed to severe acute respiratory syndrome coronavirus 2, the virus that causes COVID-19. They used vaporous hydrogen peroxide, ultraviolet light, 70°C dry heat, and 70% ethanol spray (10,11). The scientists concluded that all methods successfully eliminated detectable viable virus. However, the ethanol spray damaged the FFR’s fit and seal after 2 decontamination cycles and is therefore not recommended.
The investigators also concluded that the vaporous hydrogen peroxide decontamination process was very effective, as no virus was detected after only a 10-min treatment. The fit integrity was maintained, and the N95 FFR could be decontaminated and reused up to 3 times. Ultraviolet germicidal irradiation and dry heat were acceptable decontamination procedures but required at least 60 min. They are recommended for 2 reuse and decontamination cycles (11). All decontamination treatments must be conducted for a sufficient time to ensure adequate reduction of the virus concentration. The degree of required reduction depends on the degree of initial virus contamination. According to the Food and Drug Administration, CDC, and Occupational Safety and Health Administration FFR guidelines, the fit, seal, and functional integrity of decontaminated N95 FFRs should be evaluated.
GLOVES
Hand hygiene with soap and water for 20 s or 60%–95% alcohol-based hand rub should be performed before donning and after removal of gloves. Disposable gloves should always be discarded after a single task or patient encounter. The correct method requires removing the gloves carefully by grasping the cuff and gently pulling the glove inside itself as it slides off the hand. The process is repeated for the other hand, and both gloves are discarded.
The CDC does not recommend disinfection of disposable medical gloves as a standard practice, but in an extreme shortage of disposable gloves, this option may be considered to extend glove use (12). In the event of a glove supply crisis, gloves must be sanitized between patients within a cohort (a group of individuals with a common disease, treatment, or other similar traits) to prevent cross-contamination of microbes from patient to patient (Table 2). In the event of a glove shortage, gloves should always be discarded when visibly soiled, damaged, or after 4 h of continuous use.
Glove reuse and sanitation should be initiated only at the directive of the health-care facility administration and performed in accordance with the established policies and procedures. Sanitized gloves should be evaluated for signs of damage such as tears, holes, and rips (12). Material degradation assessments of whether gloves are brittle, stiff, or tacky should be performed, and if damage or degradation is noted, the gloves must be discarded. Glove reuse and sanitization should be terminated immediately when an adequate glove supply materializes.
CLEANING AND DISINFECTING
The policies, procedures, and practice of cleaning and disinfecting health-care facilities are complicated because of the diverse nature of care procedures. For example, surgical suite cleaning and disinfection procedures are very different from those for an imaging department, yet both require proper performance to protect patients and staff from pathogens.
Scientific evidence consistently demonstrates that contaminated environmental surfaces and noncritical items for patient care play a critical role in HAI transmission (13). Noncritical items are objects that come into contact with intact skin when the sterility of the skin contact is not critical. For example, bed rails, tray tables, blood pressure cuffs, infusion pumps, and exam tables are common noncritical items that potentially contribute to secondary transmission by contaminating health-care workers’ hands and other medical equipment. According to Spaulding’s classification scheme, noncritical equipment requires low-level disinfection (14).
All health-care facilities must use disinfectants registered with the U.S. Environmental Protection Agency. The label on these disinfectants and the material safety data sheet specify the length of contact time (kill time) necessary to inactivate one or more microorganisms completely. Cleaning and disinfecting with 1-step agents containing detergent-disinfection components require no precleaning unless significant contamination or a spill exists.
Currently, Environmental Protection Agency–registered disinfectants are available with contact times of 1–4 min. Rapid kill times increase confidence in the complete killing of the most common HAI pathogens before the disinfecting solution dries or is removed and before patients or staff retouch the surface (15). The efficacy of wipes, sprays, and solution dilution recommendations are determined according to methods developed by the Association of Official Analytic Chemists.
Disinfectant Wipes
The CDC recommends applying a low-level agent (i.e., quaternary ammonium compounds, alcohols, or chlorine) to disinfect noncritical surfaces and equipment and allowing the agent to dry for 1 min (16). Several scientific studies evaluating microbial reduction based on wet time, contact time, and dry time demonstrated significant microbial reduction with contact times of 30–60 s (13,15,17). Disposable wipes should stay sufficiently wet for 1–2 min to achieve the Environmental Protection Agency–required contact time of at least 1 min (Table 3). Wipe size and surface coverage depend on the size of the area to be disinfected. When the wipe is visibly soiled or no longer wets the surface, the wipe must be discarded and replaced. Never redip a wipe into the container of presaturated wipes, and always close the container top to prevent wipes from drying out (14). Facilities mandate which disinfectant products to use and the frequency of product rotation to maintain efficacy. If the facility uses spray bottle solutions, the bottle must be dated and replaced every 6 mo.
Cleaning and Disinfection Importance
Infection control and prevention are ever changing, as are the pathogens that health-care facilities face daily. It is well documented in the scientific literature that microbial pathogens survive on objects and surfaces for varying times (Table 4).
Survival Times for Some of the Most Common HAIs, Viruses, and COVID-19
Although cleaning and disinfecting are mandatory and effective in reducing HAIs, many environmental surfaces and objects in patient rooms are often inadequately cleaned and decontaminated (18). C. difficile, methicillin-resistant S. aureus, and vancomycin-resistant enterococci are common pathogens causing transmission concerns in hospitals. Thus, patient-care areas require enhanced disinfection after discharge of a patient.
Effective surface disinfection has 2 components: the disinfectant and the way the procedure is performed. Together, they are commonly referred to as the practice and include thorough application of disinfectant to all touchable surfaces (15). The practice should be mastered and become second nature as an integral step in daily patient-care duties. Standardization and proper training by an environmental services department or infection prevention and control personnel should focus on product selection and contact time.
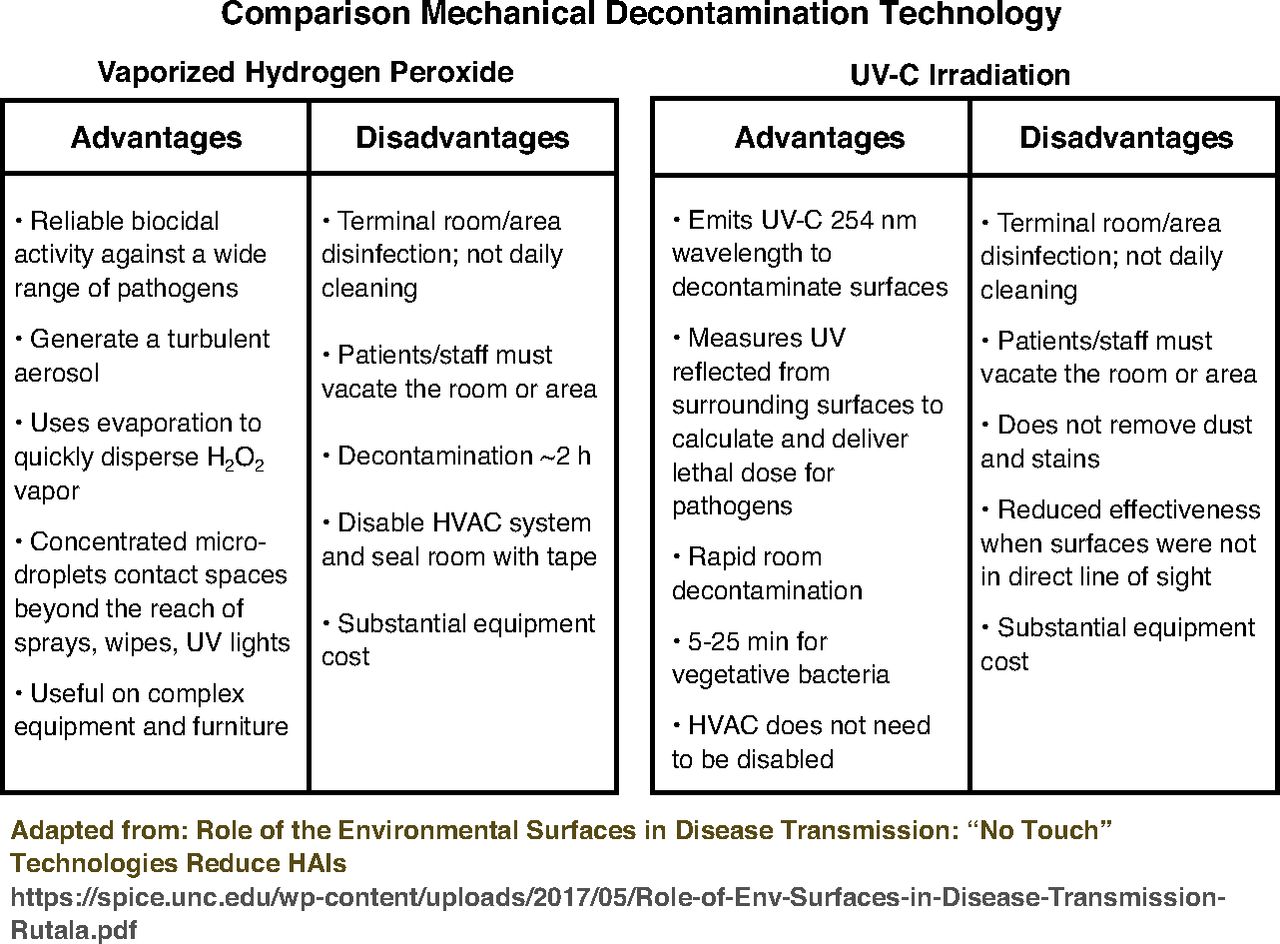
Novel no-touch or mechanical room decontamination methods represent new technology in the battle against HAIs. Data on the previously discussed vaporous hydrogen peroxide and ultraviolet germicidal irradiation systems show that they help reduce the incidence of HAIs (Fig. 2). They are recommended for room decontamination after discharge of a patient when there are contact precautions (18).

INFECTION-PREVENTION PRACTICES AND GUIDELINES FOR SAFE ROUTINE IMAGING CARE
Radiation workers are very familiar with the concept of time, distance, and shielding. These terms are also applicable in infection prevention. In response to COVID-19, the dynamics of patient flow and procedure time have changed to allow social distancing throughout a facility and the imaging lab.
Patients are now prescreened for COVID-19 risk when the appointment is scheduled and when they arrive at the facility for the procedure. Asking questions, checking body temperature, and looking for symptoms are now standard procedures. Facilities use prioritization schemes based on a patient’s clinical risk and prognostic outcome to determine the urgency of the procedure. Facilities are continuously updating policies based on the current pandemic numbers and federal and state guidelines to accommodate the diagnostic needs of the patient and to coordinate care with referring physicians.
The American College of Radiology, the Society of Nuclear Medicine and Molecular Imaging, and the American Society of Nuclear Cardiology published consensus guidelines and best practices to assist facilities in developing a care plan for patients who require imaging (24,25).
CONCLUSION
Today, the world has a heightened awareness regarding infection prevention, and everyone is making an effort to contain the spread and transmission of COVID-19. Infection prevention and control practices have been evaluated, upgraded, and standardized to ensure that health-care workers know how to protect themselves, other staff members, and patients. Every health-care institution and provider must have policies and procedures for rendering care and services to asymptomatic, suspected, and confirmed COVID-19 patients.
Time to disinfect imaging rooms and noncritical equipment must now be recognized as an essential component of the patient imaging procedure. Donning and doffing PPE, disinfecting the care area, and complying with robust hand hygiene all take time and training.
The infection prevention and control skills we learn and practice are dynamic and will continue to change to address microbe mutations and emerging pathogens such as COVID-19. Health-care workers must master infection prevention procedures, which must be an integral part of the patient-care routine.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than June 2024. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication March 10, 2021.
- Accepted for publication April 15, 2021.





{kind=link}
{kind=link}