


One of the strengths that has made the Nuclear Medicine Technology Certification Board (NMTCB) so successful for the past 43 years is the voluntary dedication of the technologists, physicians, and scientists who have served as members of the board of directors. Since the establishment of the NMTCB in 1977, at least 200 individuals have served as elected members of the NMTCB board. Each of NMTCB’s board members has made significant contributions to the development and advancement of NMTCB’s certification programs. It is also due to the support from our professional organizations, hundreds of item writers, professional staff, and, most of all, the 23,000-plus technologists who are certified by the NMTCB that the NMTCB has been able to enjoy the successes of the past 4 decades. Most technologists look to the NMTCB for their professional entry-level credential and postprimary nuclear medicine credentials, and this enthusiastic acceptance is a tribute to the high professional esteem in which each of these individuals is held.

To understand how the NMTCB has become the recognized professional certification board that it is today, we must look back at the historical events that led to its formation. From a nuclear medicine perspective, it was in the early 1960s that the γ-camera and technetium generator first became commercially available, eventually replacing the use of rectilinear scanners. The γ-camera and the availability of technetium dramatically changed the number and types of procedures that could be performed in nuclear medicine. A more defined role for the nuclear medicine technologist (NMT) began to gradually take shape at around this time as well, with many of the early NMTs coming from a background of radiology or the medical laboratory. Many of the early technologists had college degrees in a science field, but most were trained on the job to perform imaging studies. Credentialing during this period had been offered by 2 different organizations, the American Registry of Radiologic Technologists and the American Society for Clinical Pathology. Each of these organizations served a large group of stakeholders: radiographers and medical technologists, respectively.
By the 1970s, the SNM-TS recognized that the knowledge and skills needed to be an NMT were very different from those of an x-ray or medical technologist. SNM and the professional community believed it was important to have a credentialing body specific to and for the NMT, especially to make sure credentialing would keep pace with the scope of practice and the evolving field. At the SNM-TS annual meeting in June 1976, a motion was passed to appoint an NMT certification task force to explore the implementation of an independent board for nuclear medicine technology. Not much data had existed about what specific job functions an NMT performed; a task analysis would therefore be needed to determine the complete list of skills and base of knowledge required for a technologist to capably perform nuclear medicine procedures. These job performance data were gathered and analyzed by SNM’s task force members.
In January 1977, the task force recommended that an independent board for nuclear medicine technology be created as soon as possible. On June 17, 1977, just 1 y and 7 d after the SNM resolution, the NMTCB was officially granted its charter and was established as a credentialing body that would be specific to nuclear medicine. The very first NMTCB board of directors was constructed from the 11 members of the SNM’s task force, along with 1 physician who was appointed by the SNM. Soon afterward, the examination content was determined, and the group was hard at work writing and developing appropriate examination items for the first exam.
NMTCB’s first nuclear medicine examination was delivered on September 15, 1978, to 652 examinees at 22 different test sites across the United States. Since the beginning, the credential awarded to successful examinees has been named certified nuclear medicine technologist (CNMT). The NMTCB continued to offer the paper-and-pencil exam just once a year until 1985, when the board voted to offer the examination twice per year. During that period, the American Society for Clinical Pathology nuclear medicine technology examination was discontinued and individuals who had been actively certified by the American Society for Clinical Pathology were granted the CNMT credential. Since then, the number of certificants has continued to increase, and more than 40,000 people have sat for the entry-level nuclear medicine technology examination since its initial delivery. The NMTCB became the examination of choice for the NMT, a status that the NMTCB continues to enjoy, with over 23,000 technologists holding the CNMT credential. The NMTCB’s tagline, “Certification of Nuclear Medicine Technologists by Nuclear Medicine Technologists,” was true then and remains true today (Fig. 1).
NMTCB board of directors in 1992. NMTCB was founded in 1977 through efforts and funding of SNM, SNM-TS, American College of Nuclear Physicians, and American Society of Clinical Pathologists (board of registry). NMTCB is incorporated as nonprofit organization in state of Delaware.
In the early 1990s, the NMTCB began to investigate computerized testing options as a new delivery format. Paper-and-pencil tests were the standard for most medical professions at the time, but the NMTCB quickly realized the potential advantages of computerized testing, which included not only swift turnaround times on reporting of outcomes to examinees but also the ability to gather statistically relevant information about the test form and question performance. Candidates today receive an immediate pass or fail notification on the completion of their CNMT exam; however, such an instant outcome was not always a reality. In the early days, candidates had to wait weeks to receive notification by postal mail, and a small envelope in the mailbox potentially meant an unfortunate outcome whereas a large one meant that the candidate had been successful and the packet included a passing certificate.
After considering multiple vendors and delivery pathways, the NMTCB ultimately chose to move toward adopting a computer-adaptive-testing mode of delivery in 1996, which soon became a popular trend for many credentialing organizations. Delivering an exam via the computer-adaptive-testing method was certainly more expensive for the NMTCB than the traditional paper-and-pencil method, but the advantages were worth it: the candidate could find out the test results quickly; the exams could be administered considerably more frequently; the exam itself could be reduced from 200 questions to 90 questions, taking advantage of the increased precision offered by the adaptive testing model; high-quality digital images could be displayed on screen; and the analysis of each examinee’s responses could become instantaneous. Moving the CNMT exam to an adaptive delivery model was a win for everyone involved.
During the 1990s and 2000s, as the role responsibilities of the NMT continued to expand and diversify, NMT education programs, in response, had to increase both the depth and the breadth of their entry-level curriculum by adding new content rapidly. Many hospital-based programs were closing and NMT programs were shifting to academic centers. Although some of the older material being taught in NMT programs was eventually dropped, there was also a great deal of the new information being added—new techniques, new procedures, new equipment, and new Food and Drug Administration–approved radiopharmaceuticals were being added to the NMT’s educational requirements on almost a yearly basis. This meant that the NMTCB exam would need updating as well. Every 3–5 y, the NMTCB board conducts job analysis surveys to determine and understand what, exactly, NMTs are asked to do in their workplaces across the country (Fig. 2). Each of NMTCB’s credentialing programs is continually reviewed to make sure it is current with today’s practice and appropriate.
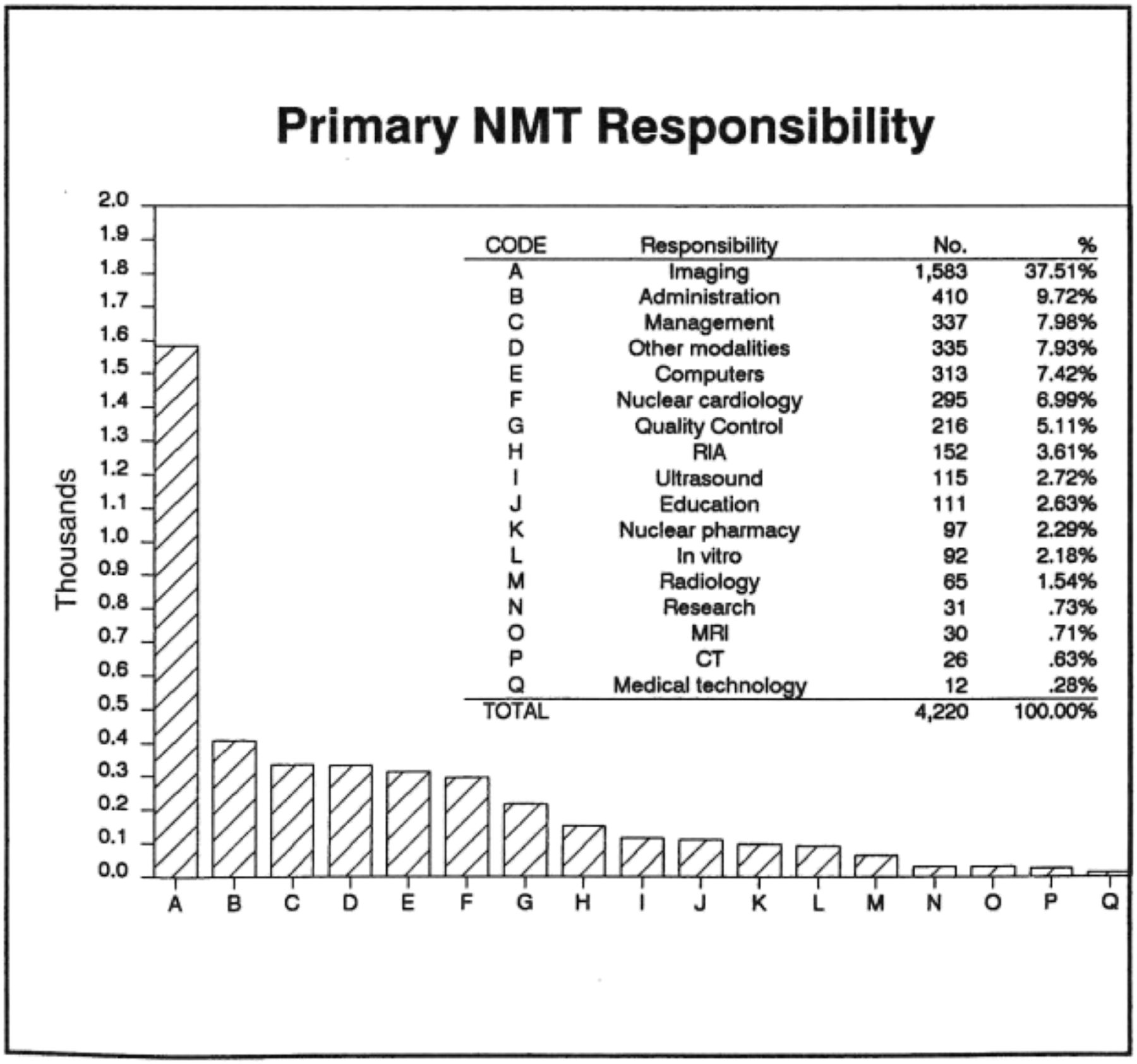
NMT’s primary job responsibilities in 1988, as reported by certified technologists practicing in clinical settings. Data on primary title/position, experience, workplace, primary responsibilities, and salary ranges have been published each time NMTCB gathers this type of information from certified technologists.


From a nuclear medicine standpoint, the field also saw an explosion of nuclear cardiology in the 1990s. In response to this movement, the NMTCB created a nuclear cardiology technologist specialty examination that was specific to the use of instrumentation, radiopharmaceuticals, and adjunct medications in the diagnosis of cardiovascular disease. Soon afterward, the field of PET took off, with imaging systems evolving and new agents coming to market. Once again, the NMTCB created a PET specialty examination for technologists that is meant to showcase their expertise and high level of knowledge in the field of PET.
Also during the 1990s, the topic of professional competency was at the forefront of many of the NMTCB’s discussions. There was an increasing desire by the public for assurance that both physicians and technologists were up to date on their current medical knowledge. The NMTCB and the American Board of Nuclear Medicine (ABNM) were part of many discussions about recertification and continuing competency. Both organizations considered several options that might be used for recertification: continuing medical education, a practice audit, an oral examination, retaking of the initial board examination, and a written objective examination. Eventually, the ABNM determined that a written objective examination would be offered to ABNM diplomates at the end of their 10-y time-limited certification.
Likewise, the NMTCB recognized that the knowledge base for nuclear medicine technology continues to change and that certified technologists need to demonstrate a continued accumulation of knowledge about the field. For many years, continuing education had been seen as an authority of the states to prescribe for licensing purposes. However, the NMTCB confirmed that the most practical, cost-effective, and fairest approach for the technologist was to implement a continuing education requirement for certificants to display their continued competence in the field. Not surprisingly, there was a heavy response from the technologist body when surveyed by the NMTCB, with most respondents stating they would be in favor of a mandatory continuing education requirement as opposed to recertifying by examination. Beginning January 1, 2006, the NMTCB board required that all certificants demonstrate involvement in educational activities by obtaining continuing education from recognized continuing education approval organizations, by successfully passing additional postprimary or specialty examinations, or by completing additional college courses related to the radiologic health sciences, patient care, business/management, technology, or education.
Although the NMTCB always strives to meet the changing needs of NMTs, for many years the organization had to grapple with changing eligibility and educational issues. For much of the 1990s and early 2000s, the NMTCB board evaluated whether the education being obtained by applicants sitting for the entry-level CNMT examination was appropriate and whether expected educational expectations were being met. By 2010, the NMTCB confirmed that most, if not all, of the candidates for the entry-level exam at that time were graduates from an NMT training program as opposed to being trained on the job. The NMTCB continued to offer the alternative eligibility route for on-the-job–trained individuals who did not complete a formal NMT training program until the end of 2015, after which time this pathway to certification was no longer available. These candidates were individuals who had worked as an NMT for at least 8,000 h during the previous 5 y and had met other didactic requirements. Many people referred to the alternate eligibility pathway as the grandfathering route; however, this pathway did not actually grant someone a certification. Instead, the alternate eligibility route was an eligibility pathway to sit for the CNMT exam.
Because of the evolving and increasingly complex educational requirements for NMTs, the NMTCB board became concerned about how an educational program could display whether it has the structured clinical training sufficient to provide a technologist with clinical competency. In 2010, the NMTCB announced that by 2017, the board would accept applications for the CNMT examination only from graduates of accredited nuclear medicine technology educational programs with specific programmatic oversight, such as the Joint Review Committee on Educational Programs in Nuclear Medicine Technology, Armed Forces Military Training Commands, Canadian Association of Medical Radiation Technologists, or Australian and New Zealand Society of Nuclear Medicine. The NMTCB found that although programs that maintained regional accreditation did demonstrate compliance with high educational standards, this type of accreditation does not look at nuclear medicine technology programs specifically. Unlike programmatic accreditation, regional accreditation does not utilize nuclear medicine professionals to evaluate the scope and quality of nuclear medicine education programs. It was and still is the position of the NMTCB that requiring programmatic accreditation will help to ensure that all educational programs are adhering to quality educational standards specific to nuclear medicine technology. This requirement also assures employers, licensing agencies, and the public that a CNMT has clearly demonstrated the knowledge and clinical competence needed to perform safe, effective nuclear medicine procedures with the level of clinical proficiency expected by the nuclear medicine profession.
In 2011, at the urging of the SNM, the NMTCB developed an examination for the nuclear medicine advanced associate (NMAA), which would be for a mid-level provider certification in molecular imaging and nuclear medicine. The SNM had developed the NMAA as a higher-level education pathway to provide a career option for advancement in the field of nuclear medicine. An NMAA has a broader scope of practice than an NMT, along with additional training similar to that of radiology residents. Recently, the SNMMI endorsed the NMAA as the recognized physician extender for nuclear medicine.
Soon after the development of the advanced NMAA credential, the NMTCB began investigating whether to offer a postprimary CT credential. The NMTCB has long recognized the critical importance of CT subject matter in the credentialing of NMTs. CT was added to the entry-level CNMT credential in 2011 but in a limited manner that addressed only minimal qualifications for a technologist to perform nondiagnostic CT procedures, such as attenuation correction and localization. In 2013, the NMTCB learned from a job analysis study of NMTs that many technologists had at least 1 hybrid system (SPECT/CT, PET/CT) in their workplace. Of the respondents who stated that they used hybrid equipment in the workplace, at least 45% stated that an NMT was responsible for operating the CT portion of the device. These factors prompted the NMTCB to develop an examination in CT to validate the professional preparation of technologists to safely and capably perform CT.
In 2015, a public survey was distributed by the NMTCB to determine whether technologists would be interested in a radiation safety credential. After 79% of respondents answered that they would be interested in such a credential, the NMTCB then developed and conducted a radiation safety officer task survey to determine the variety and frequency of radiation safety tasks being performed by radiation safety officers, as well as by NMTs who may or may not be radiation safety officers. The intent of the survey was to see what radiation safety officer responsibilities were delegated to the NMT on a daily, weekly, and monthly basis. Once the survey data were analyzed, the NMTCB board of directors agreed to endorse the plan to move forward with developing a new radiation safety credential specifically designed for NMTs. By 2017, the NMTCB had developed the NMTCB(RS) certification examination specifically for technologists who wish to lend credibility to their knowledge and experience in all aspects of radiation safety issues, to include RAM, CT, fluoroscopy, x-ray and MRI safety matters. To date, 167 technologists hold the NMTCB(RS) certification.
For the past 43 y, the NMTCB has continually provided certification excellence by offering credentials that keep pace with the scope of practice and reflect the current state of nuclear medicine technology. We have no doubt that in the coming years there will be innovations and advancements that will evolve what we know about nuclear medicine and how it will be performed. As we welcome in the newest decade of medical imaging, we know that the medical industry will continue to take on challenges to incorporate the latest technologies. We look forward to attending the SNMMI 2020 Virtual Meeting (https://am.snmmi.org/iMIS/SNMMI-AM) this year, where we will not only celebrate the SNMMI’s 50th anniversary but also hear from current industry leaders about their outlook for the nuclear medicine community.
Individuals interested in additional information on the NMTCB’s certification programs can visit the NMTCB website (https://www.nmtcb.org) or contact the NMTCB directly at board{at}nmtcb.org.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.