


Dramatic changes have transformed the landscape of nuclear medicine instrumentation over the last 50 y. Since the 1970s, diagnosing and treating diseases have evolved from a best-guess and treatment method to a more science-based test, prove-and-treat method. γ-cameras have evolved from stationary planar imaging to multihead tomographic systems and organ-specific cameras. PET systems have become a clinical reality, and use has exploded. PET has gone from 2D to 3D with time-of-flight, and we are now seeing whole-body imaging systems. New scintillation crystals have been introduced as well as solid-state detectors. Hybrid systems that incorporate CT or MRI are now commonplace. Reconstruction has moved from 2D slice-by-slice filtered backprojection to fully 3D iterative reconstruction that incorporates system modeling and often other prior information or time-of-flight data. Radioisotope therapy has expanded from 131I treatment of the thyroid to receptor-targeted agents and α-particle emitters. The changes are too numerous to detail in a single short article, and so I will focus instead on a few highlights that have affected my own career as a technologist.
In 1971, the Society of Nuclear Medicine created the Technologist Section. Technologists play a crucial role in the advancement of nuclear medicine. They are the front line in the clinical implementation and delivery of new technology, diagnostic tests, and treatments. The continuing advancements in nuclear medicine rely heavily on the technical excellence of technologists. As such, technologists in our era must not only be masters at technical and anatomic knowledge but also continue to learn and advance themselves through continuing education and self-study. Over the past decade, I have seen several new imaging procedures that did not exist when I was in school, not to mention an abundance of new radiopharmaceuticals that are released almost daily. The biggest change, however, in the last 50 y has been with PET.
PET
In the early to mid-1990s PET transitioned from a research tool to a reimbursed clinical reality, which subsequently led to an explosive growth in PET imaging and applications. At the heart of this was a simple radiopharmaceutical produced with the addition of an 18F isotope to a deoxyglucose molecule: FDG. FDG allows visualization of cellular metabolism and is particularly adept in the detection of cancer. In the beginning, these scans were very lengthy and required an emission and transmission scan. Nevertheless, PET represented a major leap in our ability to detect, diagnose, stage, and restage malignancies.
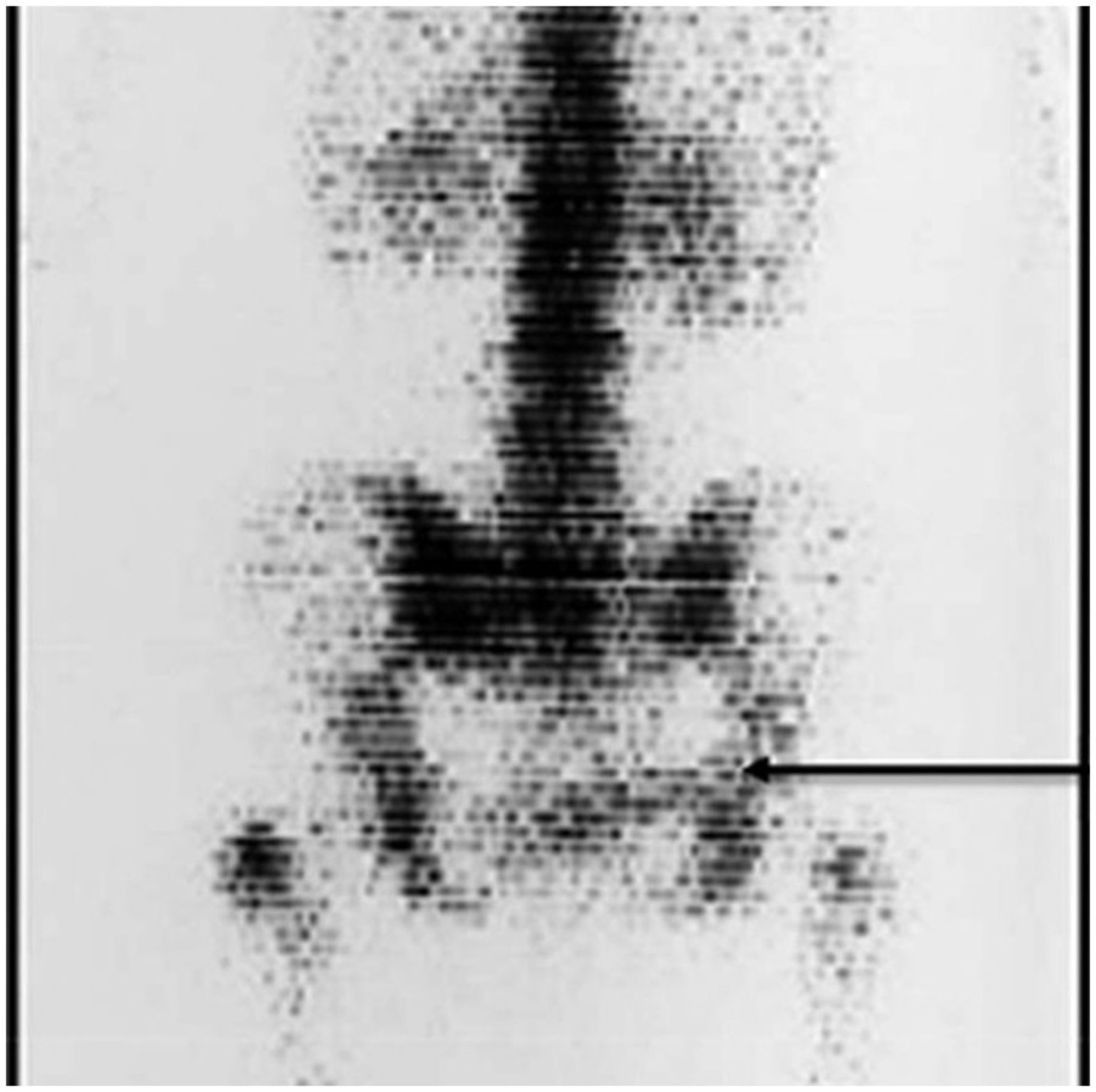
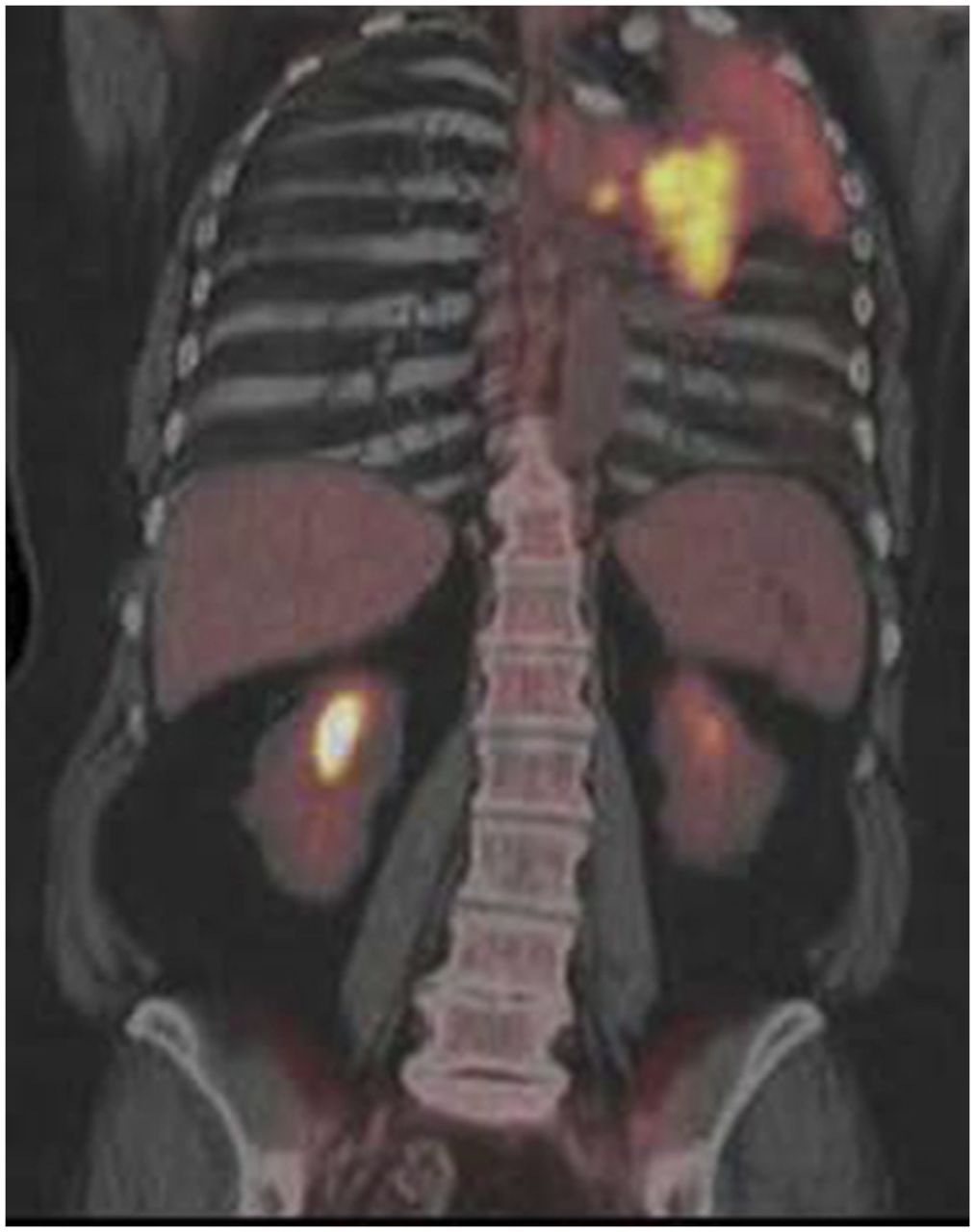
In the late 1990s and early 2000s, the radioisotope transmission scan was replaced by a CT, creating a new hybrid modality called PET/CT. The low noise and rapid acquisition of CT improved PET image quality and decreased scan times. The excellent spatial resolution of CT allowed precise localization of sites of tracer uptake. Other advances in PET technology are 3D acquisition, the progression toward smaller crystal sizes evolving from ∼6 mm in the 1990s to ∼3 mm in top systems now. Also, the advent of Silicon Photomultiplier tubes, which make for faster time of flight, individual crystal read-out (digital PET), more compact light sensors, and MR-compliant machines. These and more have led to a continuous improvement in sensitivity and image quality. Figure 1 (1) presents a PET-only scan done in the 1990s, showing multiple osseous lesions along with a presumed lung mass, and Figure 2 (2) shows a hybrid PET/CT, demonstrating a squamous cell carcinoma in the left upper lobe with associated atelectasis.


Coronal PET imaging 1 h after injection of 10 mCi FDG to a patient with small cell lung cancer. (Reprinted from (1).)
Bulk Processes to Receptor Imaging
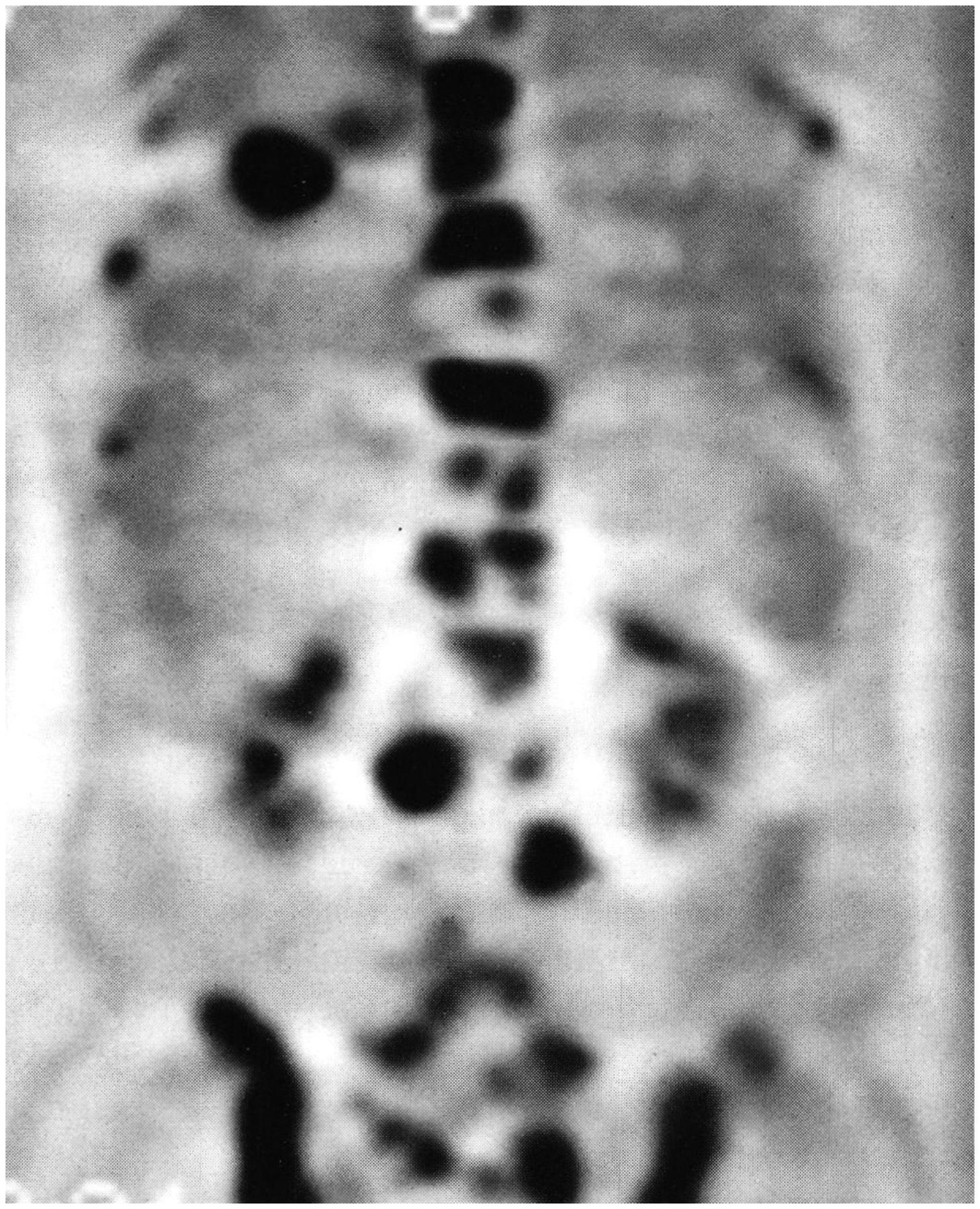
Since the beginning, nuclear medicine and oncology have been intimately connected. In 1937, the first clinical applications used 32P for the treatment of leukemia. In the 1950s, 131I was used to treat thyroid cancer (3). The imaging for these treatments was mostly done using rectilinear scanners seen in Figure 3 (4). In 1970, 99mTc generators had just become readily available. 99mTc-methylene diphosphate (MDP) imaging of the bones in 1973 (Fig. 4) (5) was a large element in any nuclear medicine department along with 99mTc-sulfur colloid imaging of the liver. “In the nuclear medicine clinic at the University of Washington, liver scanning accounted for 30% of total procedures. At M.D. Anderson Hospital in Houston, a more focused cancer center was posted to remind the technologists, do not schedule more than 40 liver scans per day” (3).

Coronal PET/CT imaging 1 h after injection on 10 mCi FDG in a non–small cell lung cancer patient. (Reprinted from (2).)

Image is a rectilinear scanner used in the 1970s. (Reprinted from (4).)
Phosphate-Labeled Skeletal Imaging
Also, in the 1970s, 99mTc-labeled phosphate, most commonly used as MDP, became a game changer with oncologists in evaluating primary and metastatic bone cancer. With this tracer, we moved to the imaging of metabolism. Tc-labeled phosphonates became one of the most popular imaging procedures for surveillance of bone disease. Part of its success was due to the improved image quality available from the γ-camera, which by 1972 was being widely used by the nuclear medicine community (6). 99mTc-labeled phosphate increased from approximately 10% of the total department volume to 35%–45% (1).
Somatostatin Receptors
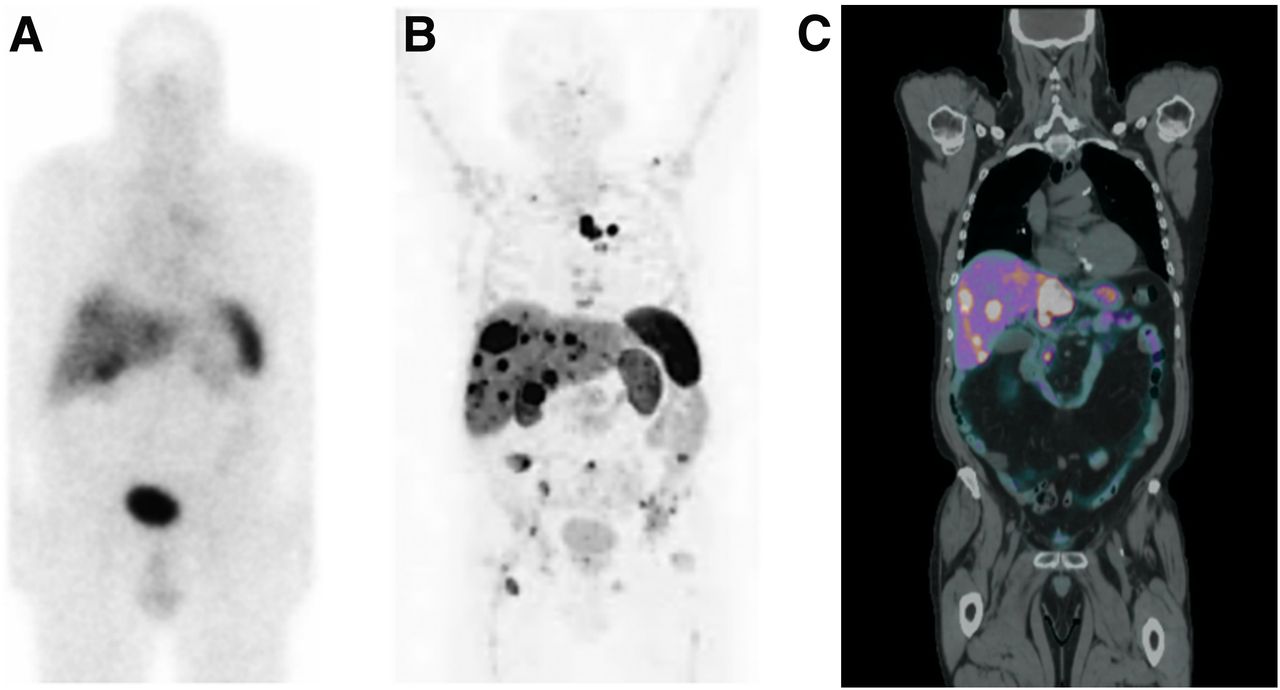
A promising advancement is the radiopharmaceutical 111In-octreotide. This radiopeptide bonds to somatostatin receptors all over the body. Neuroendocrine, carcinoid, gastrinoma, insulinoma, neuroblastoma, and medullary thyroid carcinomas have a very high concentration of these receptors, allowing visualization and localization of these cell types. The use of the new γ-camera allowed for faster imaging along with an increase in image quality (Fig. 5) (7). 111In-octreotide has nowadays been replaced by 68Ga-DOTATATE and PET imaging, which provides images with better resolution and higher contrast. The potential for new radiotracers to be developed using PET imaging will even further improve examination quality.
(Right) Rectilinear bone scan performed in 1973. (Adapted from (5).)
Expanding Roles in Therapy
Theragnostic Treatments
Like diagnostic imaging, radioisotope therapy has also been influenced by the greater availability of PET/CT. Theragnostic treatments have evolved from the original 131I and 32P to an advanced multidisciplinary treatment process. 177Lu-DOTATATE for neuroendocrine tumors is being used with success across the world currently, and 177Lu-PSMA (prostate-specific membrane antigen) for prostate tumors looks extremely promising. This has the potential to reform prostate cancer treatments and dramatically improve survival rates and quality of life.
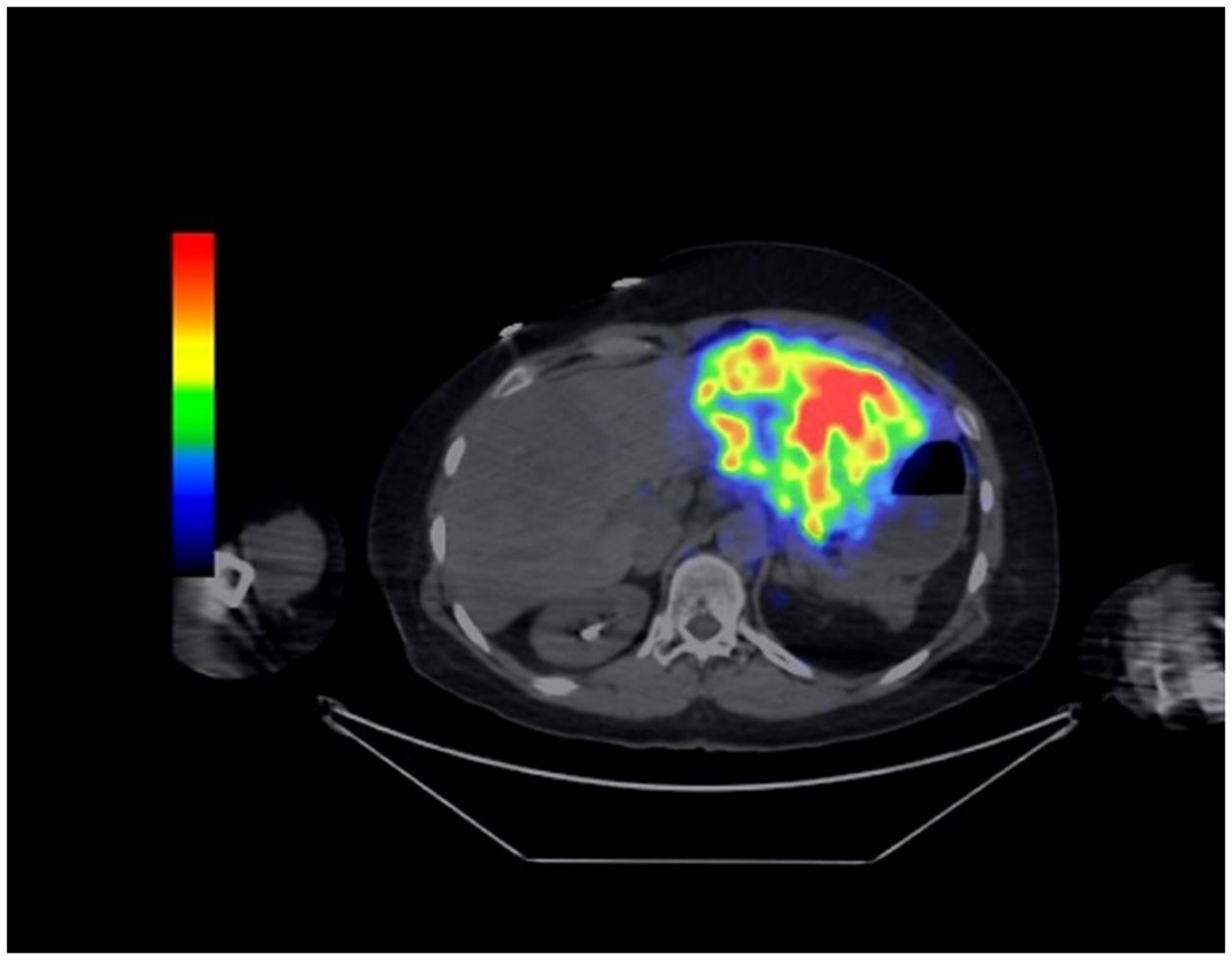
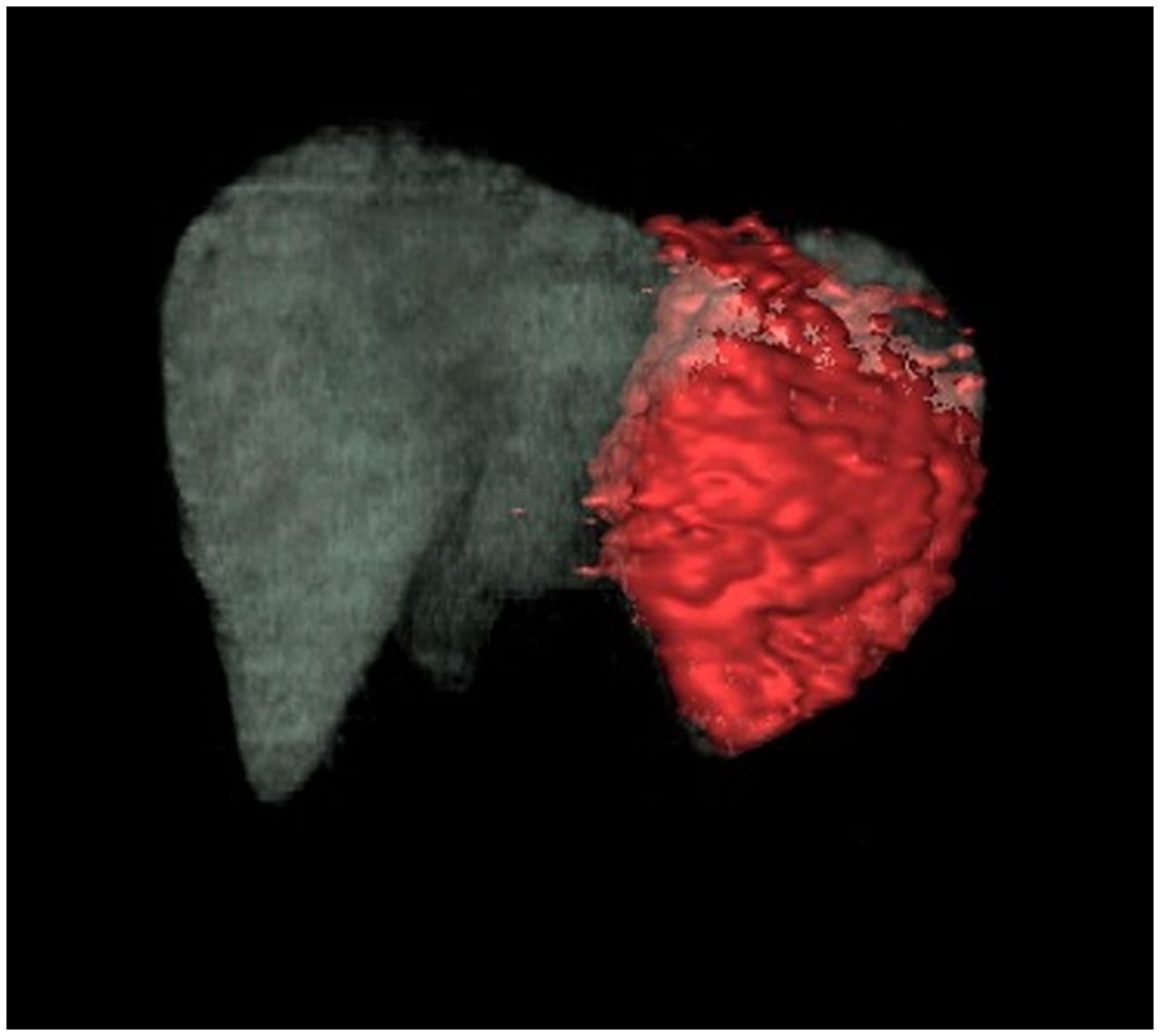
90Y selective internal radiation therapy (SIRT) radioembolization has grown in popularity over the past couple of years. The use of 90Y SIRT enables physicians to deliver a high absorbed dose directly to the tumor with a precisely placed catheter (8). This allows for selective radiation therapy. I have seen great results using this treatment that has extended lifespans, and I hope for its continued success. Figure 6 shows an axial fused 90Y PET/CT scan demonstrating left hepatic localization, and Figure 7 is a 3D volume rendering showing treated liver tissue in red (images compliments of CARTI Cancer Center in Little Rock, AR). I asked Dr. Edgar St. Amour, interventional radiologist at CARTI, why he thought CARTI Cancer Center’s 90Y program has seen such success. He said “I think we are successful for several reasons. First, we are a multidisciplinary group with medical, radiation and interventional oncology all under one roof. Therefore, our patients can be treated quickly while minimizing interruptions to treatment. Finally, we have an excellent support staff who are committed to making our 90Y program the gold standard” (Edgar St. Amour, MD, written personal interview, February 28, 2020).

(A) Planar 111In-OctreoScan. (B) 68Ga-DOTATATE PET scan; imaging in A and B was obtained 3 wk apart. (C) Coronal fused DOTATATE PET scan. (Image courtesy of CARTI Cancer Center, Little Rock, AR.)

Patients treated with 90Y resin microspheres followed by a PET/CT for coverage verification and dosimetry calculation.
WHAT IS AHEAD?
The practice of nuclear medicine has changed significantly over the past 50 y, but what will it look like in the future? The use of PET/CT, MRI, and CT will continue to be the leaders in diagnostic imaging, but the major changes, I believe, will be with the addition of artificial intelligence (AI) applications and new radiopharmaceuticals. AI will add a level of confidence by providing a more systematic approach in processing data at all levels of an examination. The ability to have computer-aided lesion detection will improve image quality and increase more detailed reporting. New PET/CT radiopharmaceuticals continue to be introduced which better differentiate disease processes and allow new theragnostic treatments. Most recently, there has been the introduction of novel tracers for detecting neurologic diseases such as Alzheimer, Parkinson, and dementia, which will further expand the field of applications. These dramatic changes will continue to take huge strides in the direction of curing diseases through clinical research. We will see substantial technologic advancements in our lifetime, and I am honored to be in the forefront of the field of nuclear medicine.
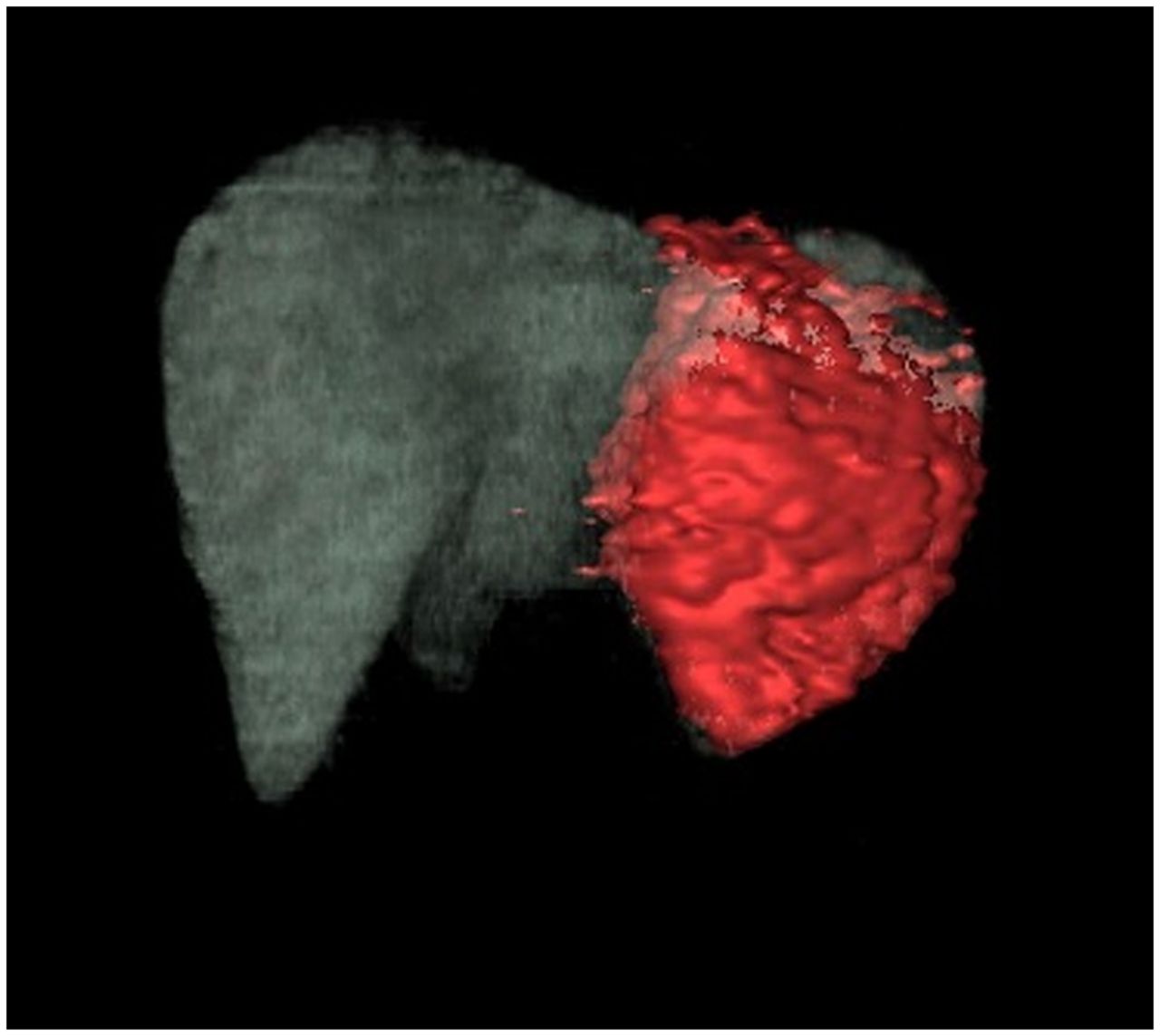
Rendered 3D volume of 90Y PET/CT in treated left hepatic lobe. Notice the red area is the treatment area. (Images in Figures 6 and 7 are compliments of CARTI Cancer Center, Little Rock, AR.)





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.