


Abstract
We describe the case of a patient who had suspected myocardial ischemia, showed normal findings on multiple perfusion scans, and showed isolated cardiac sarcoidosis on 18F-FDG-PET. Also discussed are the diagnosis and the monitoring of disease response using imaging follow-up.
Sarcoidosis is a multisystem, granulomatous disease of unknown etiology, and noncaseating granulomas are the histopathologic hallmark (1). Cardiac sarcoidosis can lead to advanced heart block, arrhythmias, cardiomyopathy, and sudden cardiac death. Reported rates of isolated cardiac sarcoidosis among patients with cardiac sarcoidosis vary widely, ranging from 27% to 54%. Diagnosis is challenging and not well defined in the literature (2).
CASE REPORT
A 69-y-old African American man with a history of atrial fibrillation, high-grade atrioventricular block with a dual-chamber pacemaker, nonsustained ventricular tachycardia, multiple prior negative perfusion studies (Fig. 1), and end-stage renal disease requiring hemodialysis presented with chest pain and exertional dyspnea.
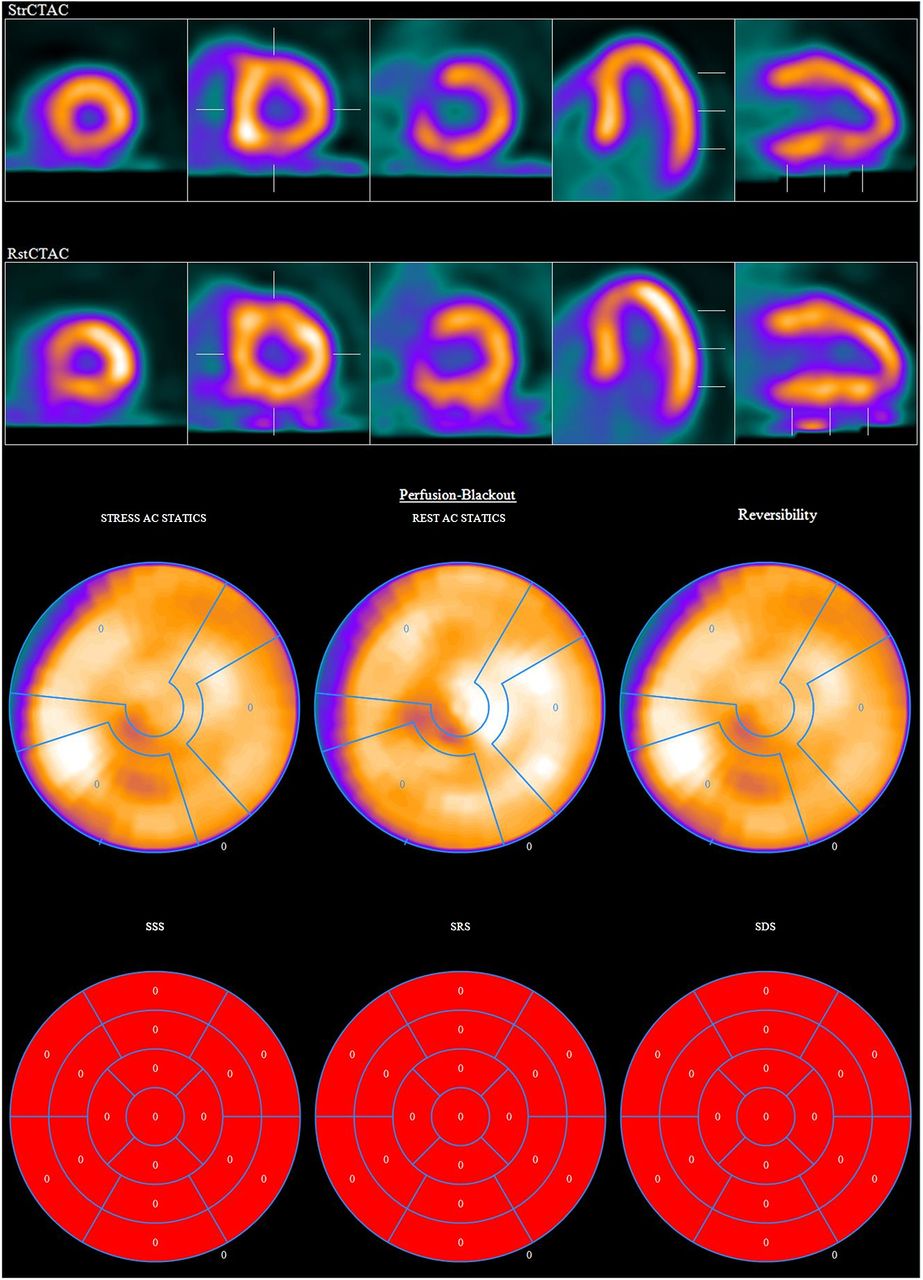
Myocardial perfusion scan with normal findings. AC = attenuation-corrected; SDS = summed difference score; SRS = summed rest score; SSS = summed stress score.
The findings on physical examination were unremarkable. Laboratory values demonstrated mildly elevated but flat troponin T, serially 0.12 ng/mL. Electrocardiography showed a ventricle-paced rhythm. Echocardiography showed normal biventricular systolic function.
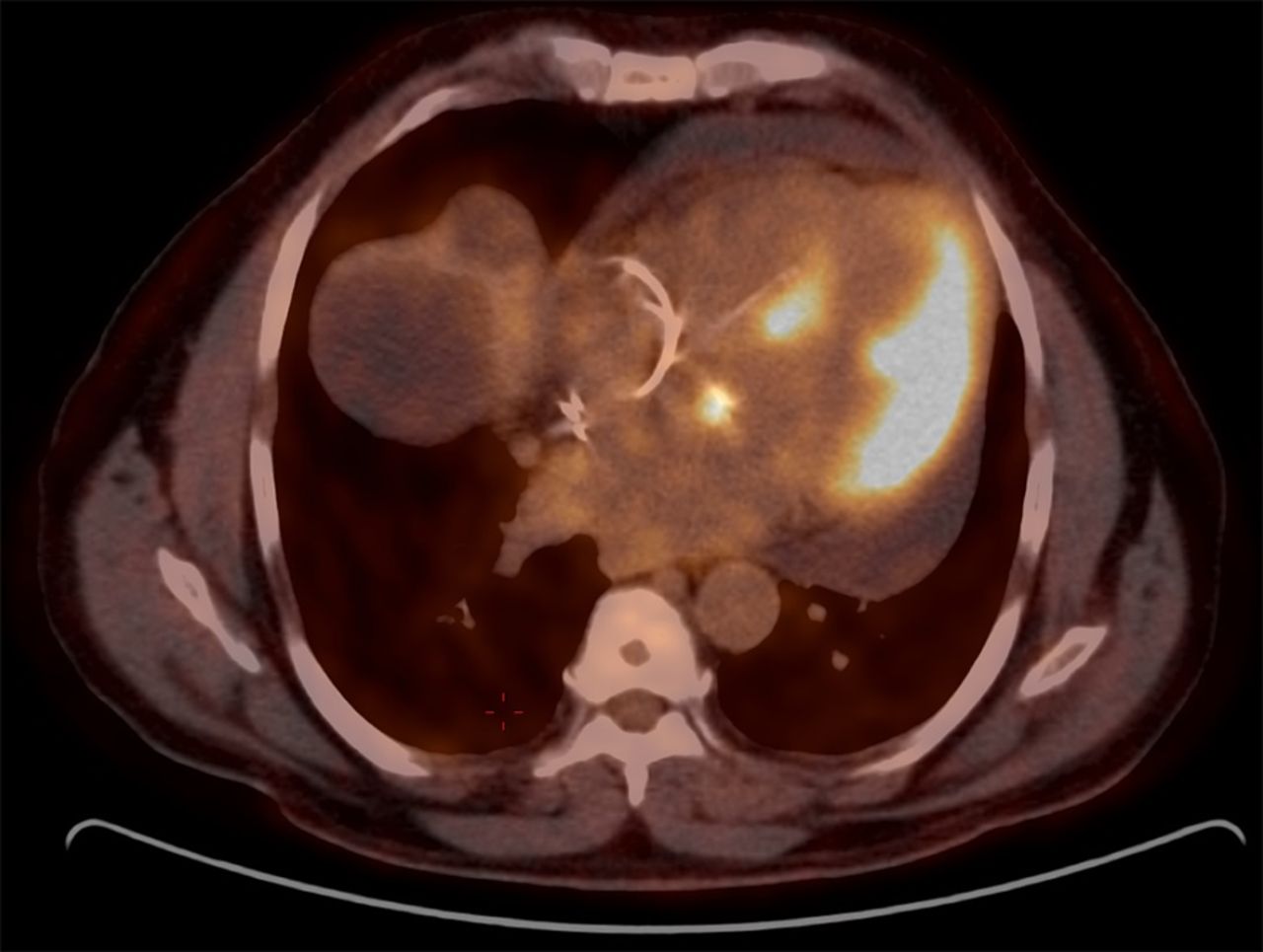
Given the patient’s race (African Americans are more prone to sarcoidosis), unexplained symptoms, heart block, and nonsustained ventricular tachycardia, 18F-FDG PET was performed. The initial 18F-FDG PET study demonstrated lateral left ventricular wall uptake (Figs. 2, 3A, and 4A) suggestive of cardiac sarcoidosis. No extracardiac sarcoidosis was found on workup. Left ventricular endomyocardial biopsy was not performed because it was likely to have a low yield and present an elevated risk. Contrast-enhanced MRI was also contraindicated because of the patient’s end-stage renal disease. The patient began taking 40 mg of prednisone daily for 5 mo, and his pacemaker was upgraded to a defibrillator. After 3 mo of treatment, a repeat 18F-FDG PET examination showed a partial response, with a significant reduction in uptake in the lateral left ventricular wall but new uptake in the septal wall (Figs. 3B and 4B).
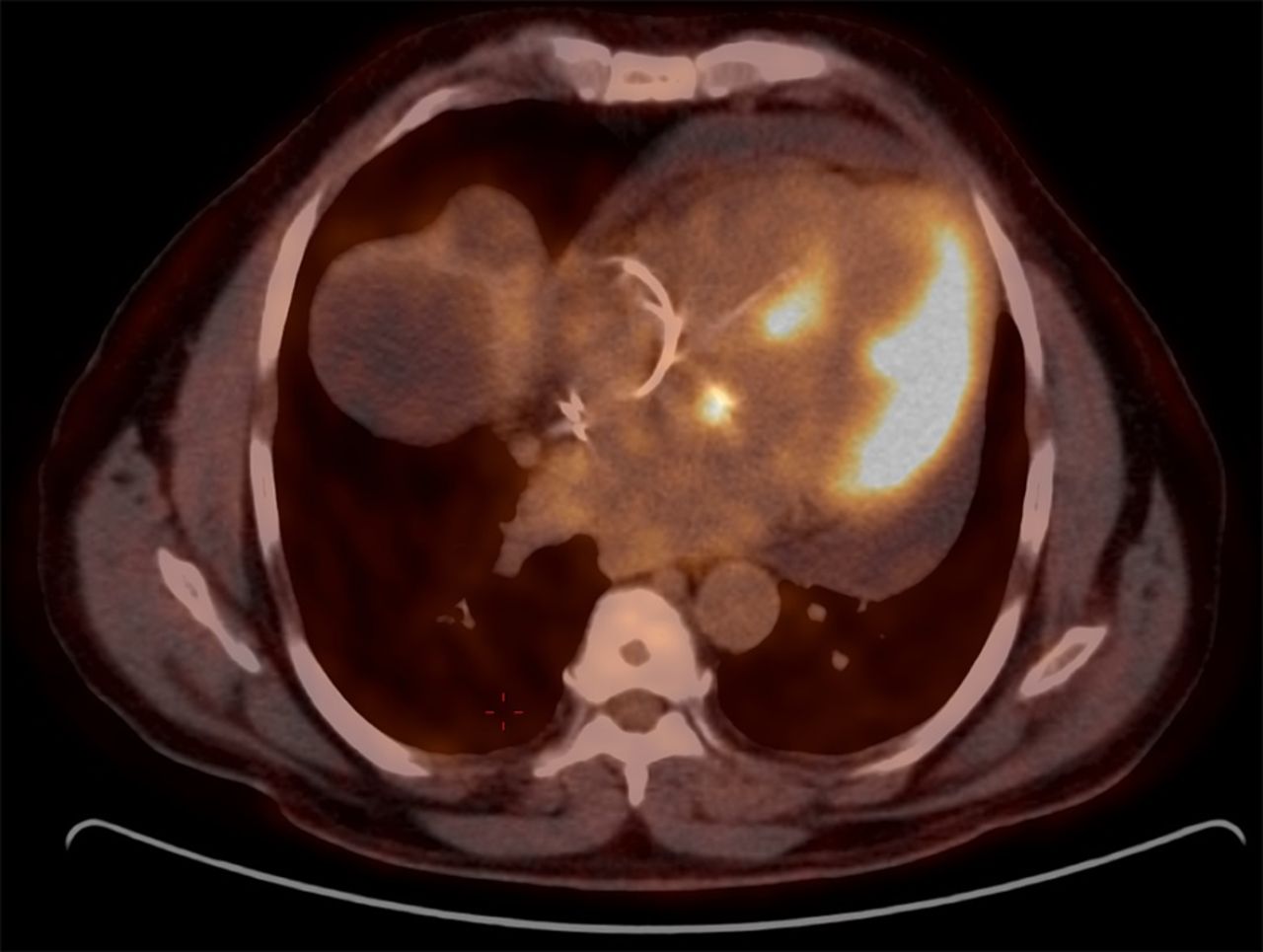
Axial 18F-FDG PET/CT image showing intense uptake in left ventricular lateral wall and lesser septal uptake.
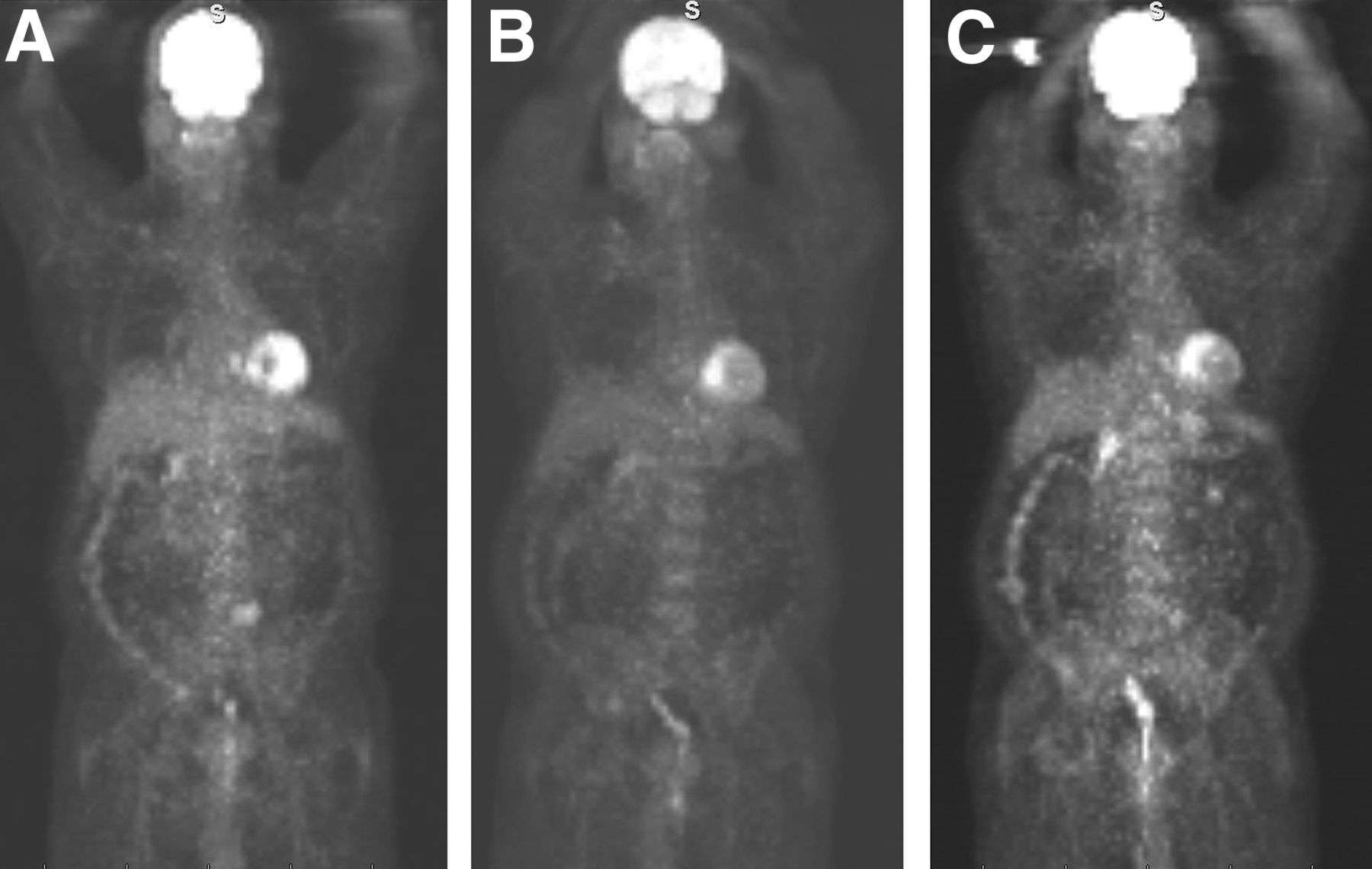
Whole-body 18F-FDG PET images obtained at 3-mo intervals, showing no extracardiac uptake. (A) Initial examination, with intense lateral wall uptake. (B) Improved findings in lateral wall but new basal–to–mid-septal uptake while patients was taking 40 mg of prednisone daily. (C) Persistent uptake in septal wall and new uptake in basal–to–mid-anterior wall while patient was taking 20 mg of prednisone daily.

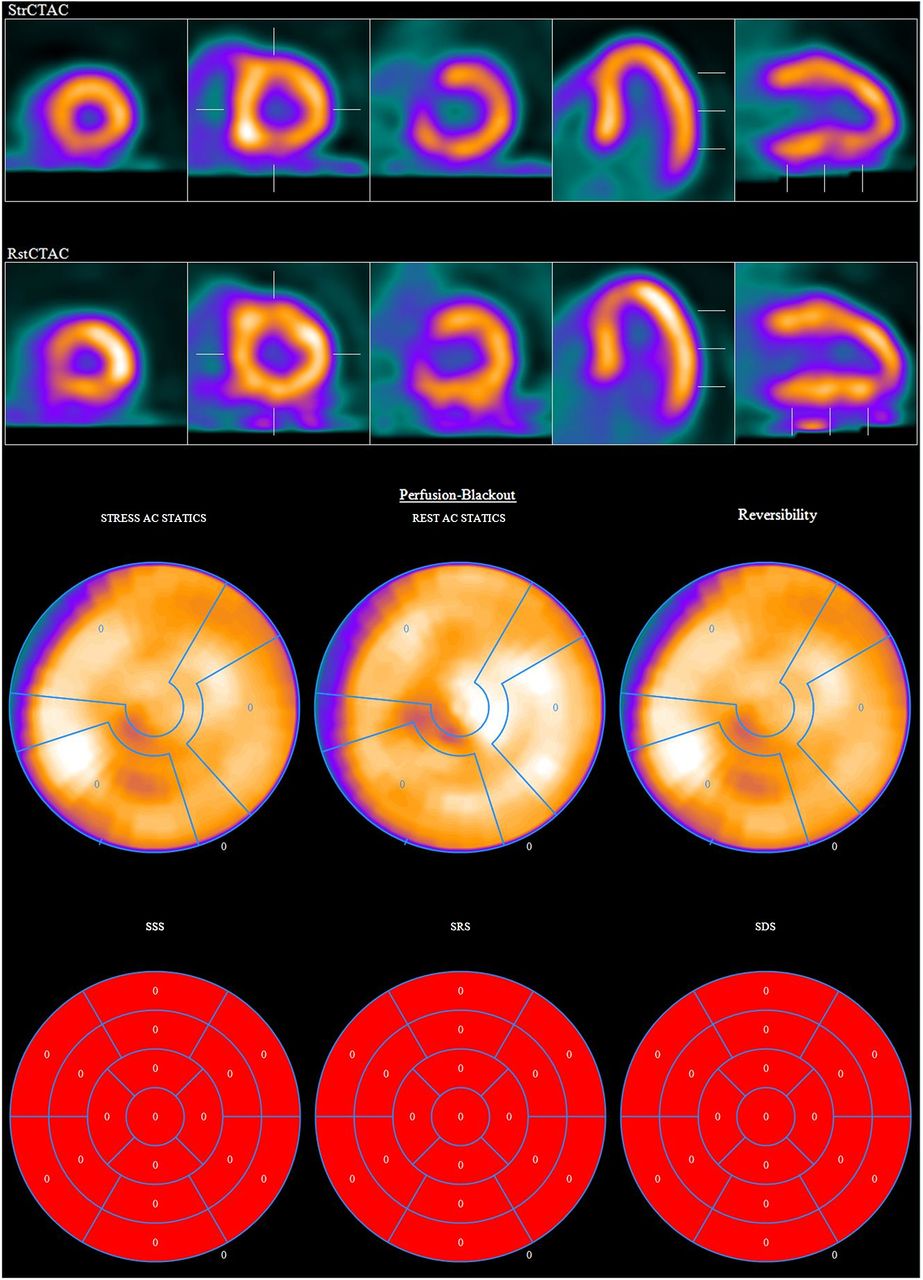
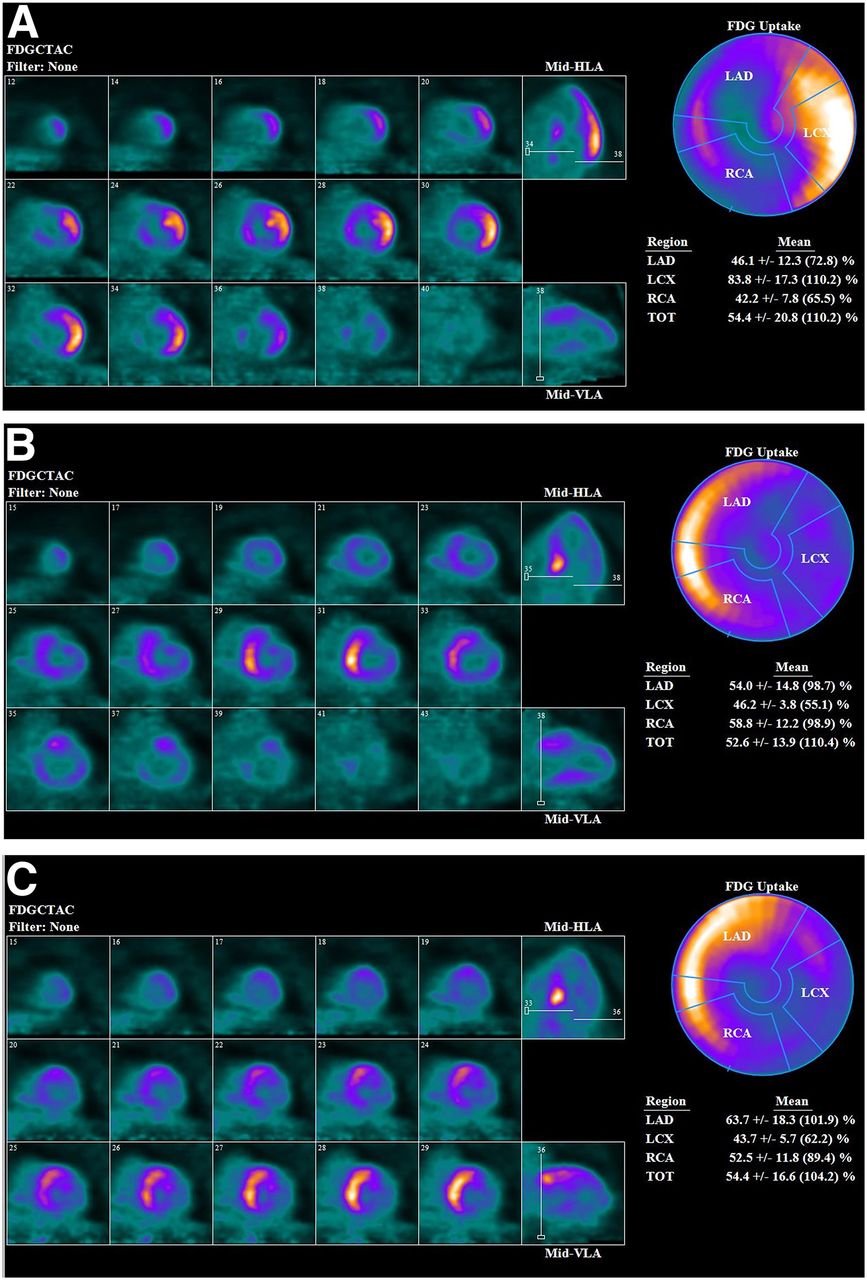
Cardiac 18F-FDG PET metabolism at 3-mo intervals, including axial, horizontal long-axis, vertical long-axis, and bull’s-eye views that again show uptake pattern seen in Figure 3. FDGCTAC = CT attenuation-corrected 18F-FDG images; HLA = horizontal long axis; LAD = left anterior descending coronary artery; LCX = left circumflex coronary artery; RCA = right coronary artery; TOT = total; VLA = vertical long axis.
The patient began taking mycophenolate mofetil, but this was stopped after 1 mo because of oral sores related to herpes virus. His prednisone dose was decreased to 20 mg per day. Repeat 18F-FDG PET after 3 mo revealed a continued response to treatment in the lateral wall but persistent uptake in the septal wall and new uptake in the basal–to–mid-anterior wall (Figs. 3C and 4C).
Currently, the patient is stable, with no cardiovascular symptoms or evidence of worsening cardiomyopathy or ventricular tachycardia. He has continued taking 20 mg of prednisone per day, with plans to restart mycophenolate at a lower dose and titrate upward as tolerated.
DISCUSSION
On the basis of available data, the approximate rate of isolated cardiac sarcoidosis among patients with cardiac sarcoidosis is 25%. There is limited sensitivity for the diagnosis of cardiac sarcoidosis, with current criteria requiring evidence of extracardiac disease or positive results on endomyocardial biopsy, which itself has limited sensitivity (20%–40%) because of the patchy nature of the disease. Diagnostic sensitivity for isolated cardiac sarcoidosis is therefore even more limited. Advanced cardiac imaging techniques using a combined approach of 18F-FDG PET and cardiac MRI could improve early detection of isolated cardiac sarcoidosis and improve the accuracy of diagnosis by providing data on both inflammation and scarring or fibrosis. Whole-body 18F-FDG PET is also useful for screening for extracardiac involvement (2). Cardiac MRI was not performed for our patient because of his history of kidney failure and the risk for nephrogenic systemic fibrosis. Endomyocardial biopsy was not performed because of its low sensitivity, pacemaker dependence, and increased risk.
Most experts agree that corticosteroids with or without immunosuppressive therapy should be used in the treatment of cardiac sarcoidosis. 18F-FDG PET reassessment of response to treatment is recommended at 3-mo intervals (1). Our patient showed a mixed response to treatment at both the 3-mo and the 6-mo intervals (Figs. 3 and 4). The data are insufficient to guide management for patients with a mixed response.
CONCLUSION
Diagnosis of isolated cardiac sarcoidosis is currently not well defined, and symptoms can overlap those of myocardial ischemia. The presence of ventricular tachycardia and a high-grade atrioventricular block should raise suspicion that cardiac sarcoidosis may be present. Given the variable response to current therapy, frequent 3-mo follow-up with cardiac imaging and monitoring of clinical response is recommended to guide treatment.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 9, 2020.
REFERENCES
- Received for publication April 3, 2020.
- Accepted for publication May 5, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}