


Abstract
PET and SUV depend on reliable pharmacokinetic modeling, part of which is predictable dose delivery. Partial extravasation of the intravenous dose administered undermines the predictability of dose delivery and, potentially, the accuracy of the SUV calculation. Use of the Lara device with topical sensors is a simple, noninvasive way to determine partial dose extravasation. As part of routine monitoring of 18F-FDG PET administrations, an interesting case was identified that mimicked extravasation but represented dose leakage during infusion via an automatic injector. The Lara device provided a useful tool for more timely critical evaluation and problem solving, extending advantages to the patient and practice.
PET and quantitative values such as the SUV depend on reliable pharmacokinetic modeling, part of which is predictable dose delivery. Partial extravasation of the intravenous dose administration undermines the predictability of dose delivery and, potentially, the accuracy of SUV calculations (1). Visually reviewing images after a PET procedure is perhaps the most common way to identify extravasation; however, because the injection site may be outside the field of view for whole-body PET, which is typically performed with the patient’s arms hyperextended above the head (Fig. 1), this method is not always accurate (2). A simple tool for detecting extravasation is the Lara (Lucerno Dynamics) device, which uses topically applied scintillation sensors to monitor activity migration inward from the injection site during the uptake phase. Data from the United States using this device suggests that as many as 23% of doses are partially extravasated and go undetected (3).

Partial extravasation (arrow) of 18F-FDG in patient in whom reconstructed study excluded injection site from field of view.
CASE REPORT
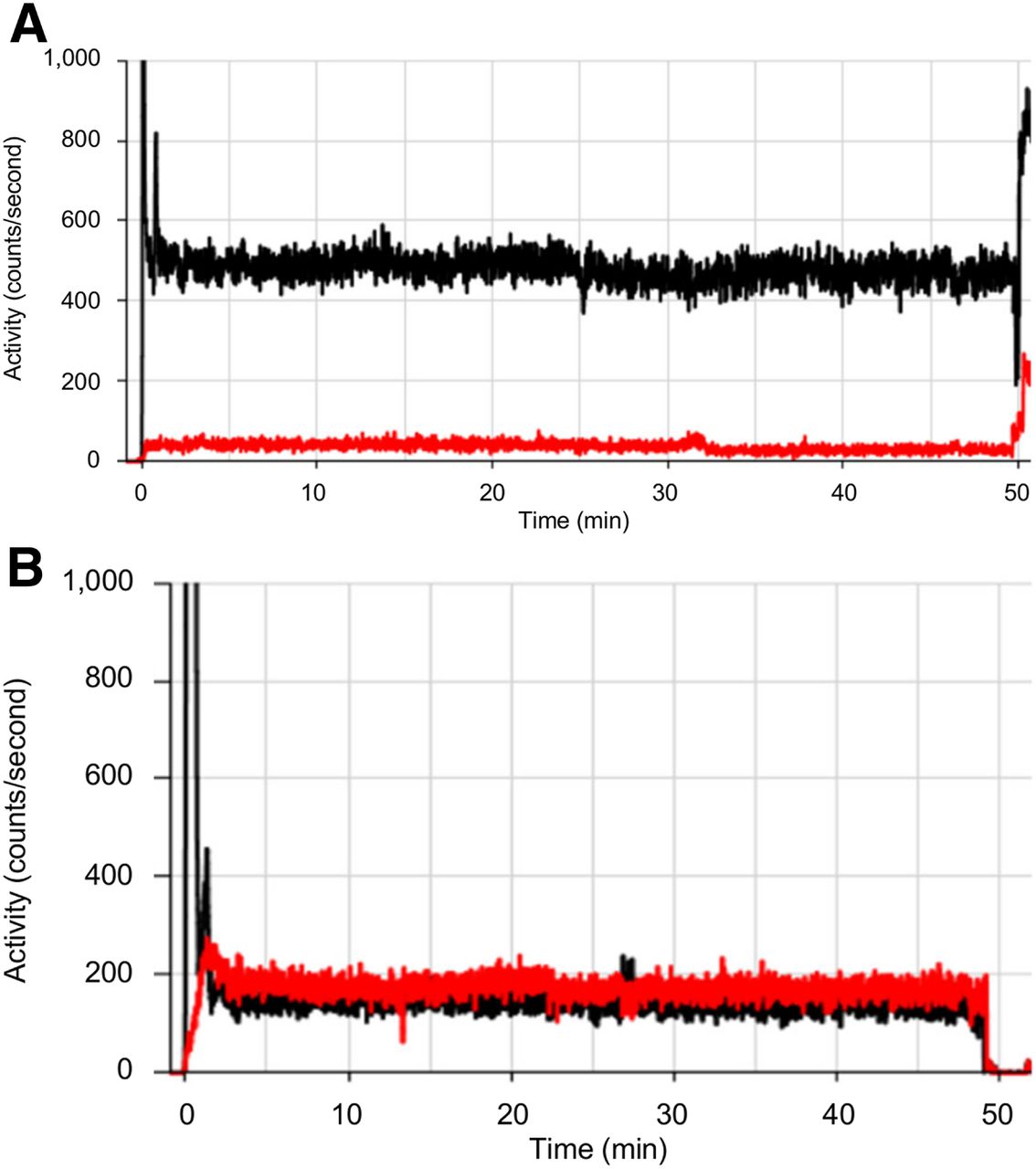
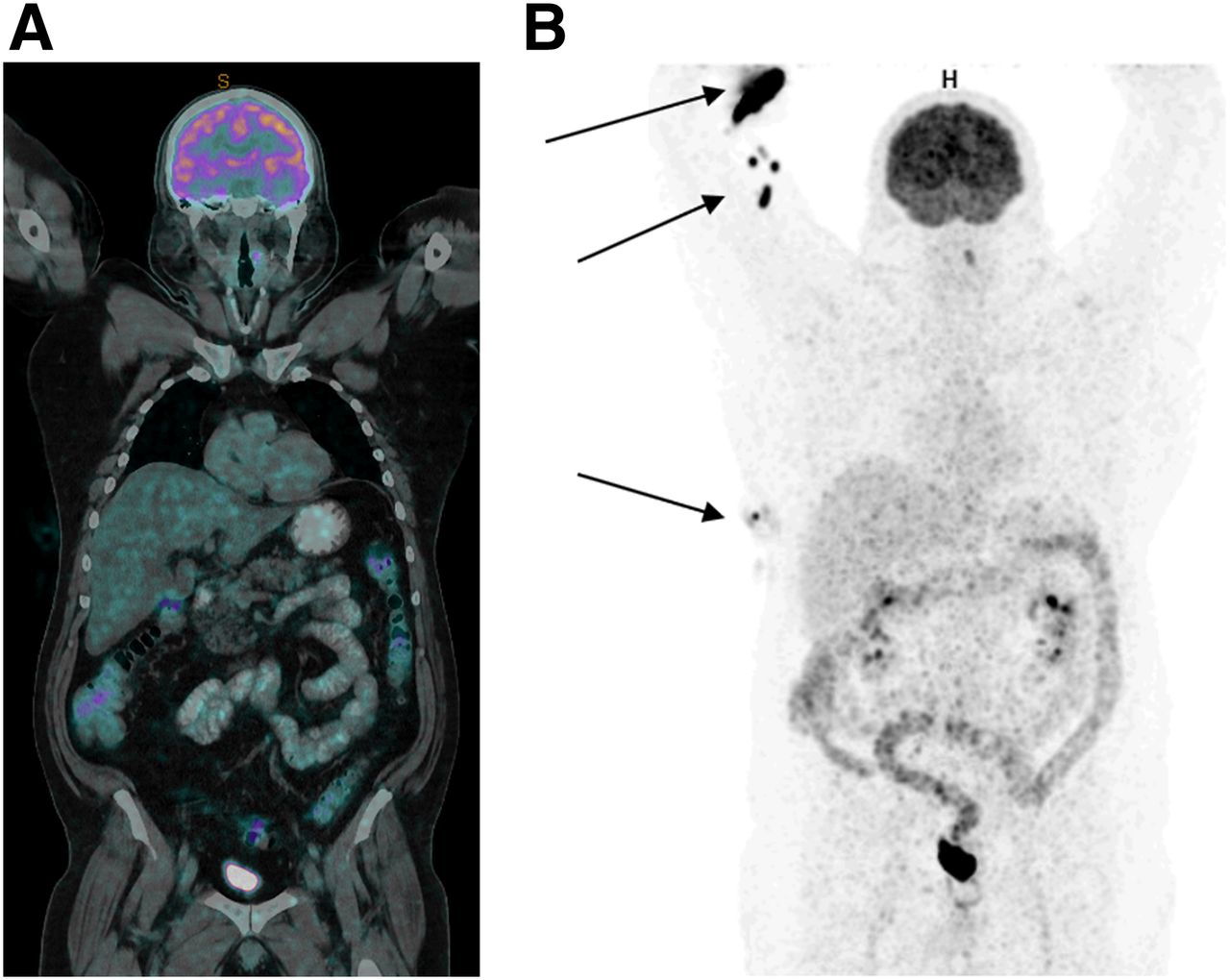
A 58-y-old man with a history of follicular lymphoma presented for whole-body 18F-FDG PET for follow-up evaluation 2 mo after chemotherapy. The patient was administered 331 MBq of 18F-FDG via a 20-gauge cannula in the right cubital fossa. As part of standard care, Lara sensors were applied to the patient using adhesive pads 7 cm proximal to the injection site and the same site on the contralateral arm (control arm). The automatic injector (KARL100; Tema Sinergie) was connected to the cannula to begin the injection, and Lara monitoring continued through the uptake phase as standard protocol. The automatic injector administers the correct dose via a Rad-Inject pump (Imaxeon). The information gathered from the Lara device was entered into the software platform, and a time–activity curve was produced for the injection arm and the control arm (Fig. 2A). Under normal circumstances (Fig. 2B), the injection-arm curve is expected to peak early and then drop rapidly to approximately the level of the control arm as the bolus moves away from the point of injection. In this patient (Fig. 2A), the injection arm activity peaked and then reduced rapidly but remained significantly higher than, and did not converge with, the control arm. This finding is consistent with retention of the 18F-FDG at the injection site. The patient was prepared for scanning, and whole-body imaging was performed (Fig. 3A). On examination of the time–activity curve (Fig. 2A), closer attention was paid to the whole-body PET scan, which was noted to be of low count and poor quality (Fig. 3A) and to show evidence of skin contamination by 18F-FDG (Fig. 3B). Further investigation revealed that a large portion of the intended 18F-FDG dose was resident in the pillow on which the patient’s arm had rested during the injection and uptake phase. In this case, the dose had not extravasated; rather, a leaking connector had caused part of the dose to reach the patient’s systemic circulation and the remainder to be shunted outside the injection apparatus and absorbed into the pillow (with some skin contamination on the arm and flank). The patient was rescheduled, and the subsequent 18F-FDG PET scan was performed without incident (Fig. 4).
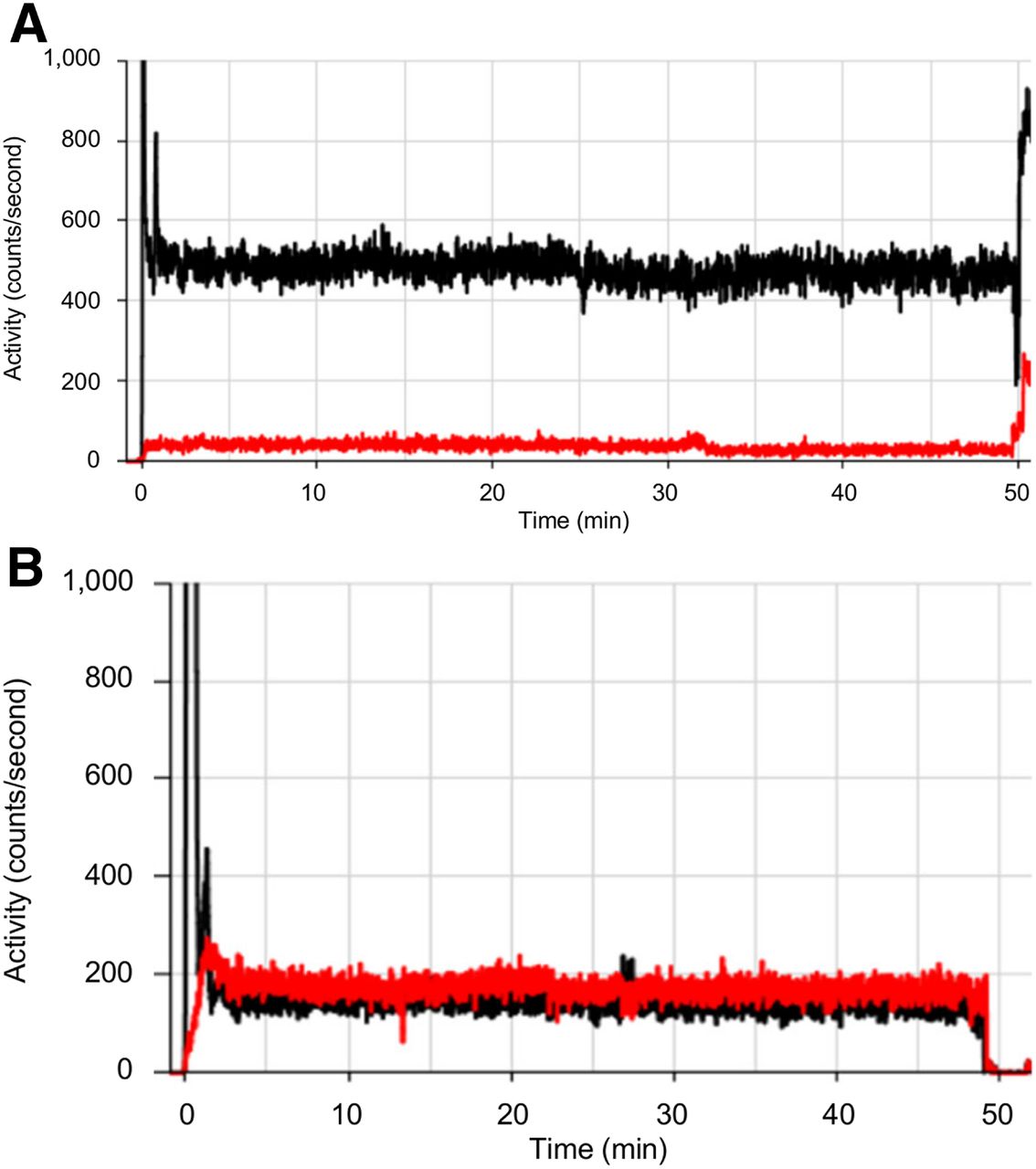
Time–activity curves for injection site (black) and control arm (red) showing rapid peak of injection bolus followed by static residual activity in injection arm, suggestive of extravasation (A), and normalization to control arm, suggestive of no extravasation (B).
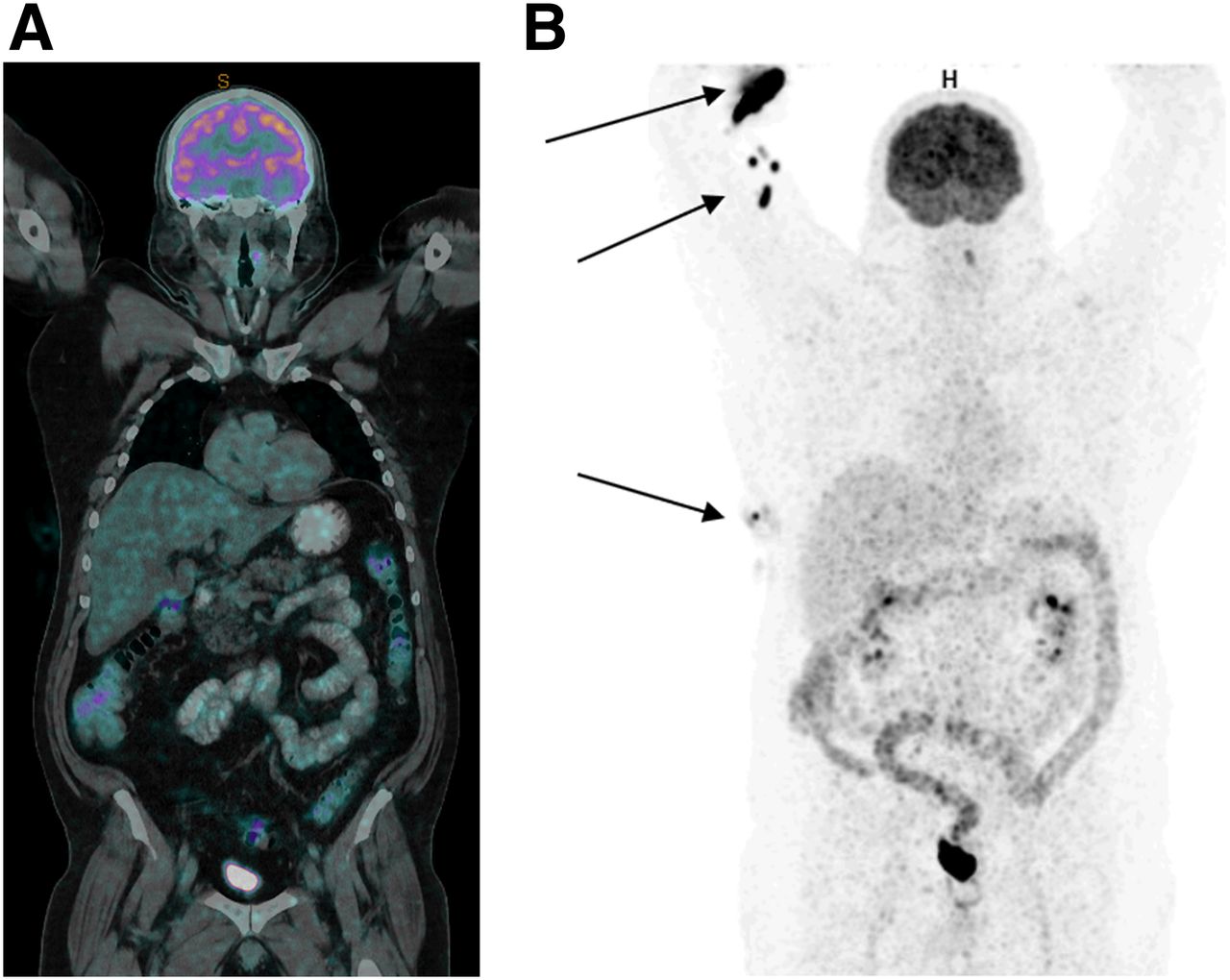
Whole-body (truncated at hips) imaging at 60 min after intravenous administration of 18F-FDG. (A) PET/CT image of low count and poor quality. (B) PET image showing skin contamination of radiopharmaceutical (arrows).

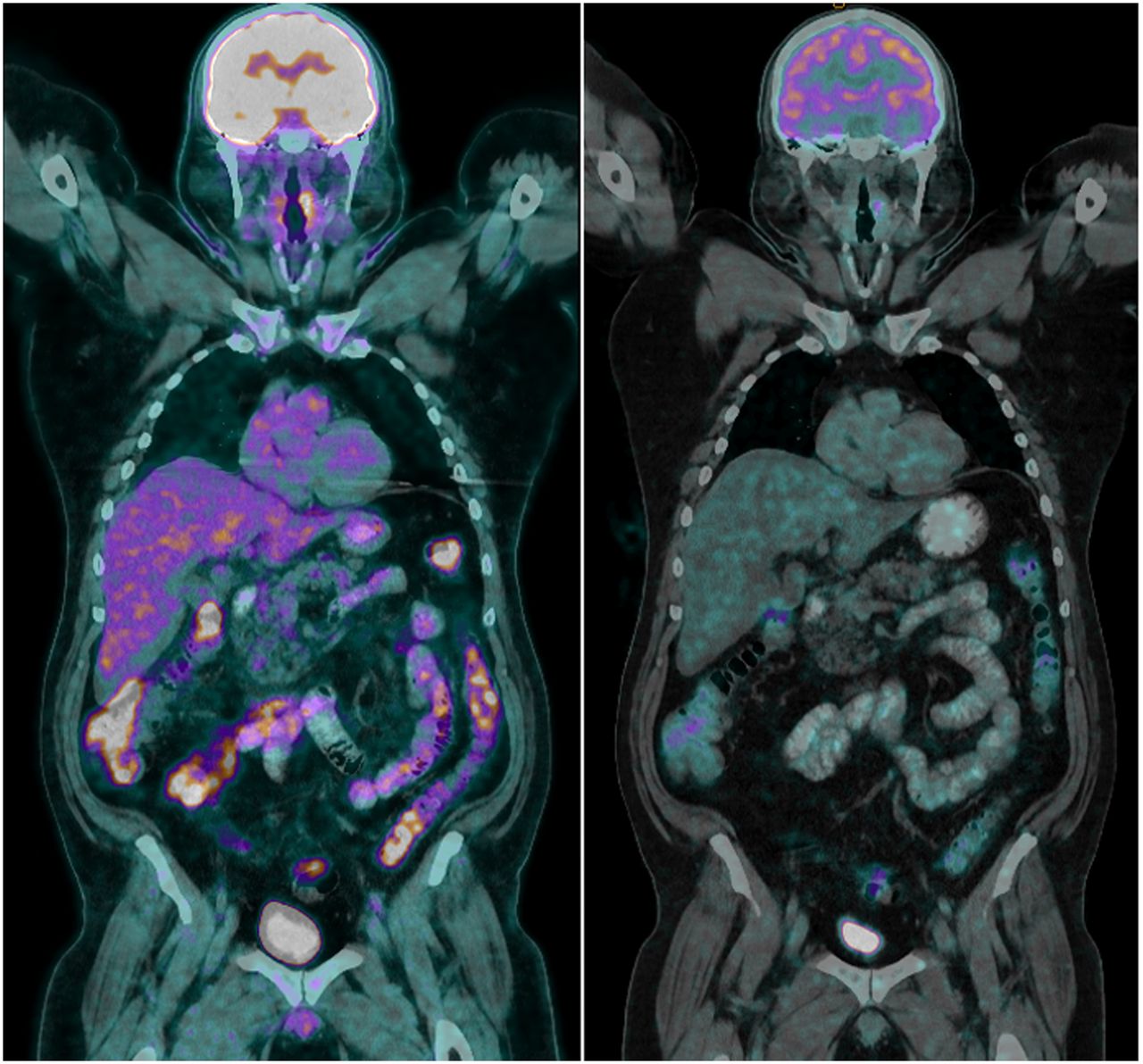
Repeated 18F-FDG PET/CT scan (left) demonstrating superior counts and quality compared with original scan (right), which had count loss associated with leaked activity.
DISCUSSION
Although the automatic injector set-up with a large-bore cannula and high-volume flush is thought to minimize partially extravasated doses compared with hand injection, hand injection in this case would have provided the opportunity to observe the leak, take corrective measures, circumvent most of the leakage, and prevent the need to repeat the study. Automatic injectors also reduce the radiation dose to the staff; therefore, the added value of using them needs to be offset by measures to ensure that unsupervised injection lines remain patent.
CONCLUSION
The Lara device provided a useful tool for more timely critical evaluation and problem solving, extending advantages to the patient and practice.
DISCLOSURE
This project was funded by an ANSTO/ANZSNM research grant. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 20, 2020.
- Received for publication December 6, 2019.
- Accepted for publication March 5, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.