


Abstract
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than September 2023. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
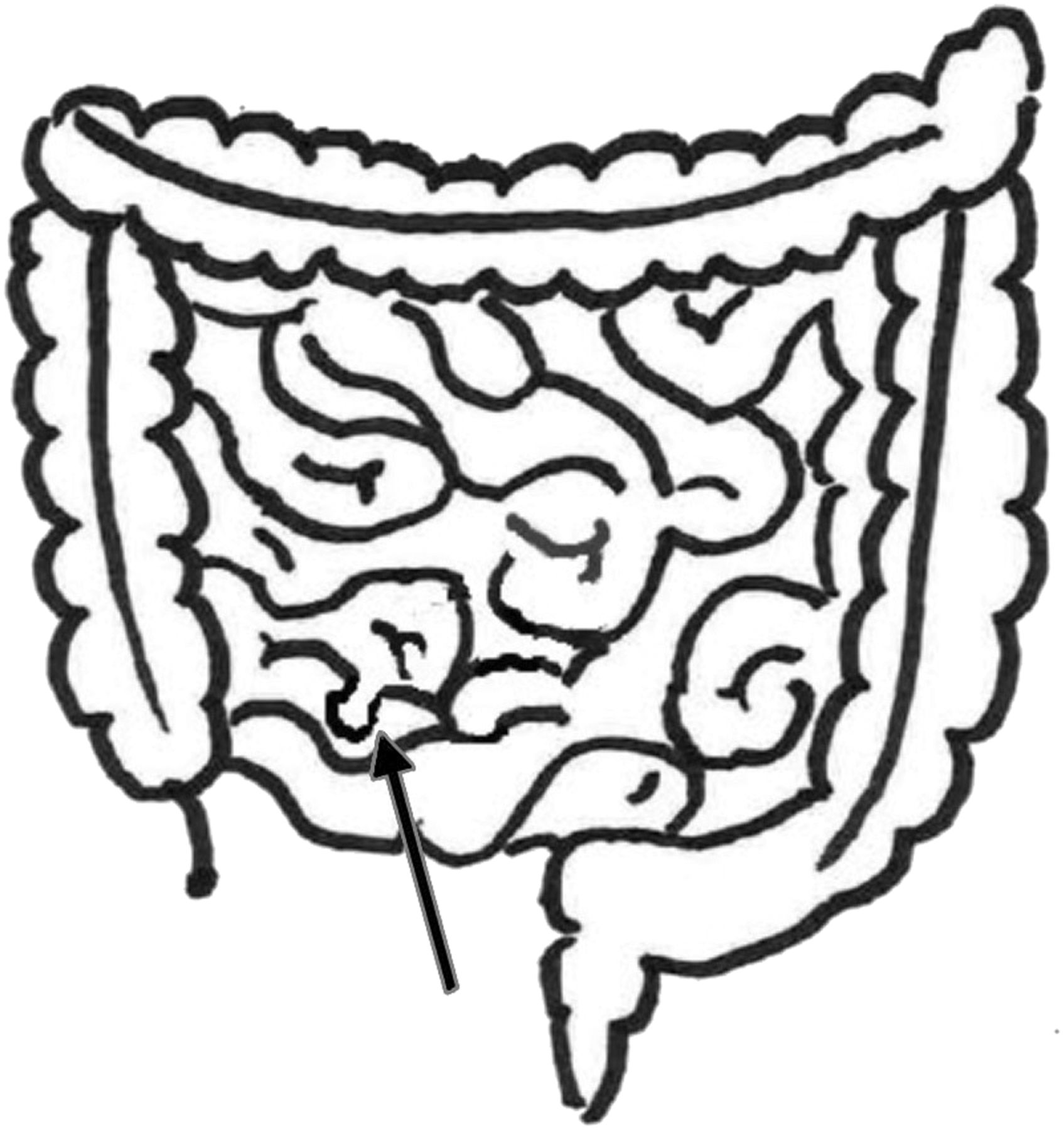
Meckel’s diverticulum is a congenital malformation in the lower part of the ileum (Figure 1). It is the most common congenital abnormality of the gastrointestinal tract, occurring in 1% to 3% of the population. The condition is named after German anatomist Johann Friedrich Meckel, who first described the condition in 1809. Meckel described it as an omphalomesenteric duct remnant. In 1598 Fabricius Hildanmas also described the abnormality, as did Lavater in 1671; however, Meckel is given credit as he was the first to recognize the embryologic origin.
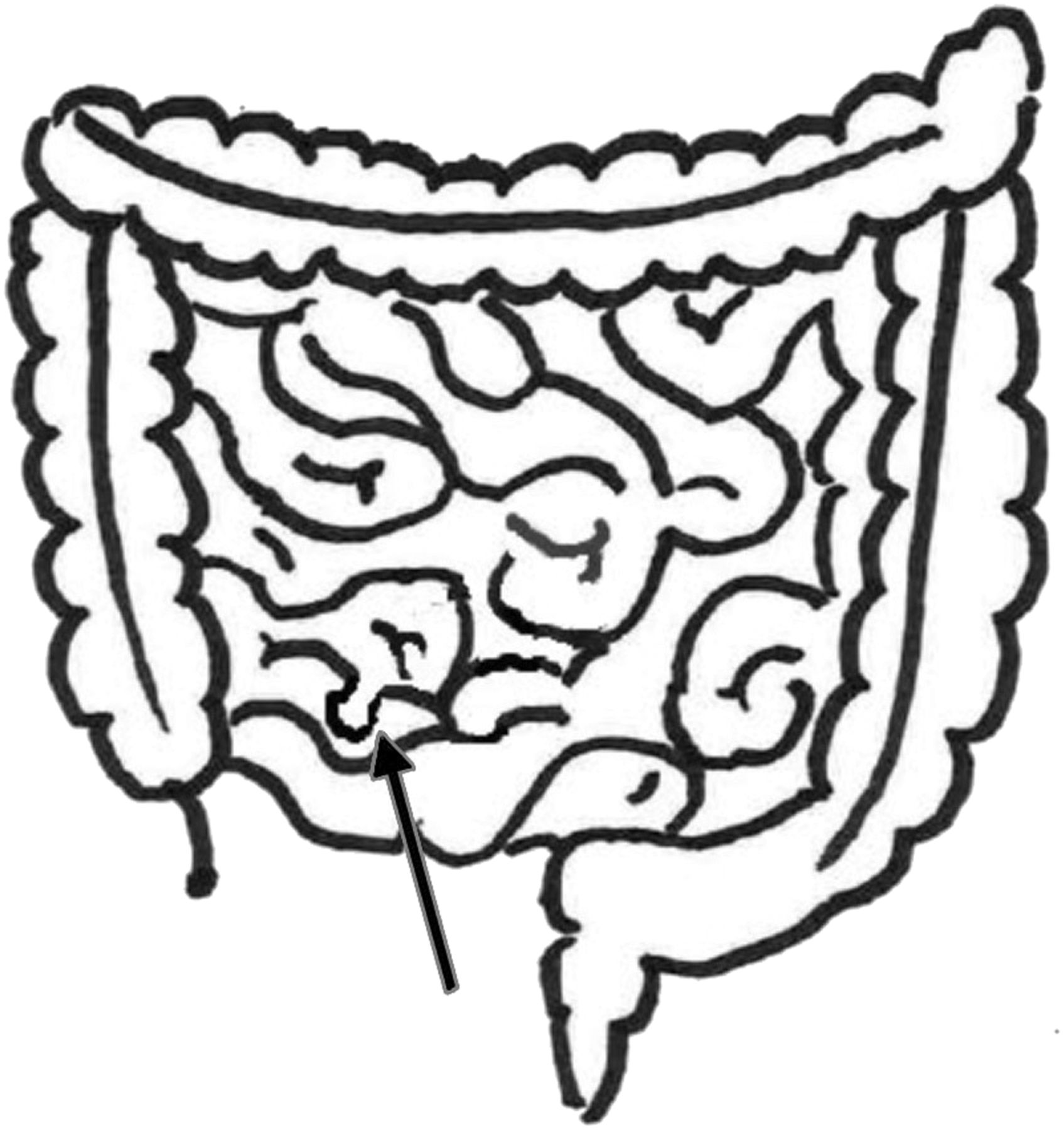
Diagram of the small and large intestine demonstrating an outpouching of the ileum as seen in Meckel’s diverticulum (arrow).
Meckel’s diverticulum is a vestigial remnant that arises from the failure of the omphalomesenteric duct to close. The omphalomesenteric duct connects the yolk sac in the embryo to the early foregut through the umbilical cord.
Meckel’s diverticulum is the most common cause of gastrointestinal tract bleeding in children and requires surgical correction. Along with bleeding, Meckel’s diverticula can cause bowel obstruction from volvulus (twisting of the intestine around itself) or intussusception (sliding of the intestine into an adjacent segment—similar to the collapsing of a telescope). Meckel’s diverticula can also cause local irritation without a perforation. Symptoms of Meckel’s diverticulum include gastrointestinal bleeding, cramping, tenderness near the navel, intestinal obstruction causing pain, bloating, diarrhea, constipation, vomiting, and diverticulitis.
Meckel’s diverticulum is described by the “Rule of Twos,” which states:
It occurs in 2% of the population.
The symptoms usually appear before the age of two or within the first two decades of life.
There are two types of ectopic tissue (gastric and pancreatic).
It is usually located within 2 ft of the small and large intestine junction (ileocecal valve).
It is approximately 2 in (5 cm) long.
It is two times more likely to be symptomatic in males than females, and
2% become symptomatic (however, most Meckel’s diverticula are clinically silent).
RATIONALE/INDICATIONS/CONTRAINDICATIONS
The detection and localization of a symptomatic Meckel’s diverticulum are based on accumulation of technetium-99m (99mTc) pertechnetate in the gastric mucosa. Pertechnetate concentrates in the gastric mucosa by active transport in the mucous cells. It is transported in a manner similar to that of halide anions (e.g., chloride and iodide). Pertechnetate can be excreted by either the gastrointestinal tract or the kidneys.
Meckel’s diverticulum is often diagnosed as an incidental finding during surgery or on autopsy. Only 2% of patients with Meckel’s diverticulum develop symptoms, and of those cases, 25% may develop complications. One of the symptoms includes hematochezia (maroon or fresh blood in the stool). Many times the bleeding diminishes and recurs intermittently. The bleeding can occasionally be excessive and life-threatening.
Symptoms of Meckel’s diverticulum can also occur as a result of intestinal obstruction. These symptoms include bloating, pain, constipation, diarrhea, and vomiting. When Meckel’s diverticulitis causes only inflammation, without perforation, the symptoms often resemble those of appendicitis.
Meckel’s diverticulum can be difficult to diagnose, as the symptoms mimic many other abdominal conditions. The clinical indication for Meckel’s scanning is unexplained gastrointestinal bleeding, especially in young children. Meckel’s scanning should not be performed if the patient is actively bleeding. If the patient is actively bleeding, a gastrointestinal bleeding scan with radiolabeled red blood cells is indicated.
PATIENT PREPARATION/EDUCATION/FOOD/MEDICATION RESTRICTIONS
Appropriate patient preparation is important in imaging Meckel’s diverticulum. Fasting for 3 or 4 hours prior to the exam helps to shrink the size of the stomach and improves the detection of ectopic gastric mucosa; however, the scan can be performed if the patient has recently eaten.
The patient should not have had any barium studies within 3 or 4 days of the scan, as the barium can cause attenuation. Also, the patient should not have had any recent (3–4 days) studies with in vivo–labeled red blood cells because the circulating stannous ion from the cold pyrophosphate may cause the pertechnetate to label the red blood cells instead of concentrating in the gastric mucosa. Stannous ions can remain in the blood for several days. Prior in vitro red blood cell labeling is not a problem. Procedures such as endoscopy or colonoscopy can irritate mucosa cells and result in uptake of the pertechnetate. Finally, enemas and cathartics (medications that irritate the gastrointestinal tract) should not be used within 2 or 3 days before the exam.
Certain medications can positively and negatively affect the results of the scan. Histamine H2 blocker and glucagon administration prior to the test improve the sensitivity of the study. Histamine H2 blockers such as cimetidine (TagametTM), ranitidine (ZantacTM), and famotidine (PepcidTM) decrease acid secretion, which also reduces secretion of pertechnetate by the gastric mucosa, thereby improving detection. The cimetidine dose is 10 to 20 mg/kg per day by mouth for neonates, 20 mg/kg per day for 2 days for infants and older children, and 300 mg by mouth 4 times per day for 2 days for adults. The ranitidine dose for children is 2 mg/kg orally, and for adults, 150 mg/kg orally. Famotidine is given orally at 0.5 mg/kg per day for children and 20 mg for adults. All three of these medications can also be administered intravenously. More information can be found in the SNMMI and EANM Practice Guideline for Meckel Diverticulum Scintigraphy 2.0. Proton pump inhibitors such as omeprazole (Prilosec®) and lansoprazole (Prevacid®) may also be helpful and are frequently used in children.
Glucagon pretreatment helps to relax smooth muscle and reduce peristalsis of the gastrointestinal tract. Slowing the transit of the secreted pertechnetate aids in detection. Glucagon is administered intravenously at 50 μg/kg to a maximum of 1 mg. It should be diluted with 10 mL of sterile water and then infused slowly over two minutes prior to administering the pertechnetate. The intravenous line must be flushed with sterile water before and after the administration of glucagon; normal saline should not be used. Side effects of glucagon include nausea and vomiting, so glucagon is given before the radiotracer to avoid vomiting and aspiration during the study. Note: Glucagon cannot be given to diabetic patients.
In the past, patients were pretreated with pentagastrin; however, pentagastrin is no longer recommended, due to side effects, and it is no longer available in the United States.
Medications that reduce the sensitivity of the test include sodium perchlorate and atropine. Sodium perchlorate decreases the uptake of pertechnetate in normal and ectopic gastric mucosa. Sodium perchlorate may be given after the completion of the test to wash out pertechnetate from the thyroid and reduce radiation exposure. The quality of the images is also reduced if the patient has been given atropine.
IMAGING PROCEDURE
The recommended dose for Meckel’s diverticulum imaging from the 2012 North American consensus guidelines for administration of pediatric radiopharmaceuticals is 1.85 MBq/kg (0.05 mCi/kg) of 99mTc-pertechnetate. The minimum administered dose is 9.25 MBq (0.25 mCi). The adult dose is 300 MBq (8 mCi), with a range of 300 to 400 MBq (8–12 mCi) 99mTc-pertechnetate intravenously.
The patient should void immediately prior to the start of the test. A large-field-of-view camera with a low-energy, all-purpose, or high-resolution collimator is centered over the right lower quadrant of the supine patient’s abdomen. The view should include both the xiphoid and pubis symphysis. The camera should be centered on the 99mTc 140 keV photopeak, and a 128 × 128 matrix is used. The camera can be zoomed appropriately for the patient’s size when imaging children. The patient is injected intravenously, and dynamic flow images are acquired at 1 second per frame for 1 minute. The flow images help to identify a focus of blood pool that could be confused with ectopic gastric mucosa. Dynamic images at 1 minute per frame are continued for at least 30 minutes. If the dynamic images are normal during the 30-minute dynamic images, a 60-minute image can be acquired; however, imaging more than 60 minutes is not helpful, because activity will begin to pass from the stomach to the intestine. SPECT imaging at 3 degrees per step for 360 degrees and 30 seconds per frame is helpful if the diverticulum is small or if there is interference from the bladder. Post-void erect, right lateral, posterior, and oblique views for 5 minutes or 500,000 counts are recommended.
Finally, if the Meckel’s diverticulum is adjacent to the bladder and the patient is unable to void, urinary catheterization is helpful.
RADIATION EXPOSURE
The ICRP 106 model estimates that IV injection of 296 MBq (8.0 mCi) 99mTc-pertechnetate for a Meckel’s diverticulum study would impart an approximate effective dose of 3.8 mSv (0.38 rem) in an adult male. The critical organ for this study is the upper large intestine, which would receive 16.9 mGy (1.69 rad). Intravenous injection for an adult female of 296 MBq (8 mCi) 99mTc-pertechnetate would impart an approximate effective dose of 5.0 mSv (0.50 rem). The critical organ for this study is the upper large intestine, which would receive 21.6 mGy (2.16 rad).
PROCESSING
The dynamic images may require motion correction to minimize the effects of patient motion during image acquisition. Dynamic images can be viewed in cine format or reformatted to longer time intervals to improve visualization of suspected sites of abnormality. The dynamic images should be summed at 5 minutes per image and displayed along with the additional static images. Scaling of the images is helpful to detect small, abnormal areas of increased uptake. SPECT processing is performed based on manufacturer’s recommendation.
IMAGE INTERPRETATION
The flow study should demonstrate normal appearance of the radiotracer in the heart, lungs, major blood vessels, liver, spleen, and kidneys. The normal biodistribution of pertechnetate includes uptake in the thyroid, salivary glands, gastric mucosa, and choroid plexus. Meckel’s diverticulum usually appears as a focus of increased tracer activity in the right lower quadrant within 5 or 10 minutes of injection (Figure 2). Ectopic gastric mucosa is visible as a focal, localized area of uptake that appears at the same time as the activity in the normal gastric mucosa. The intensity of the activity may appear to fluctuate due to intestinal secretions, increased intestinal motility that washes out the pertechnetate, or hemorrhage.

99mTc-pertechnetate dynamic imaging demonstrating the appearance of a small focus of activity (arrows) in the right lower quadrant that increases in intensity over time. The early intensity of the radiotracer coincides with the intensity of tracer in the stomach. This image was originally published in JNM. Grady E. Gastrointestinal Bleeding Scintigraphy in the Early 21st Century. J Nucl Med. 2016; 57:252–259. © by the Society of Nuclear Medicine and Molecular Imaging Inc.
Lateral, oblique, and SPECT views are useful in differentiating the diverticulum from renal or ureteral activity. The diverticulum will appear anterior to the renal or ureteral activity. Upright views help to differentiate the duodenum from the ectopic gastric mucosa. Upright positioning will also help to drain the radiotracer from the renal pelvis. Postvoid images help to distinguish diverticula adjacent to the bladder.
SENSITIVITY/SPECIFICITY/ACCURACY
Meckel’s diverticulum is often difficult to diagnose because the symptoms are nonspecific. When Meckel’s diverticulum scintigraphy is performed correctly in the appropriate clinical setting, the accuracy is 90%. Accuracy can be improved with the use of histamine H2 blockers and glucagon. The sensitivity and specificity are 85% and 95%, respectively. The sensitivity and specificity are higher in children than adults.
False negative studies can occur if the proper technique is not followed, if the amount of ectopic gastric mucosa is insufficient for detection (below the resolution of planar technetium imaging), or because of rapid washout of the pertechnetate. In addition, impaired blood flow due to volvulus or intussusception can result in false negative scans. False positives can occur for numerous reasons, including improper technique, uptake by other sites of ectopic gastric mucosa, and adjacent small bowel activity.
ARTIFACTS AND PITFALLS
The test might be falsely negative if the patient had a recent barium study where the barium attenuates activity in the diverticulum. A false negative will also occur if the patient erroneously received sodium perchlorate prior to the exam or had a previous study with in vivo labeling of the red blood cells with pyrophosphate. False-positive results can occur if there is irritation of the bowel from recent colonoscopy, endoscopy, enemas, or laxatives. False positives can occur if other anatomic variants or abnormalities mimic the appearance of Meckel’s diverticulum.
SUMMARY
Meckel’s diverticulum is a congenital malformation in which ectopic gastric mucosa is present in a slight bulge of the lower part of the ileum. It is the most common cause of gastrointestinal bleeding in children and requires surgical repair. It is characterized by the Rule of Twos in that it occurs in 2% of the population and the symptoms usually appear before the age of two. The diverticulum is usually 2 in long and located within 2 ft of the ileocecal valve. Meckel’s diverticulum is difficult to diagnose, as the symptoms are nonspecific. Meckel’s diverticulum scintigraphy with 99mTc-pertechnetate has an accuracy of 90% and is the best procedure for the diagnosis of the condition. The study requires strict patient preparation and precise technique.
Footnotes
↵* Reprinted from Bolus N, Farrell MB, Zimmerman J, eds. Abdominal Imaging 2017: Quality, Safety, and Dose Optimization. Reston, VA: Society of Nuclear Medicine and Molecular Imaging; 2017:76–83.





{kind=link}
{kind=link}