


Article Figures & Data
Figures
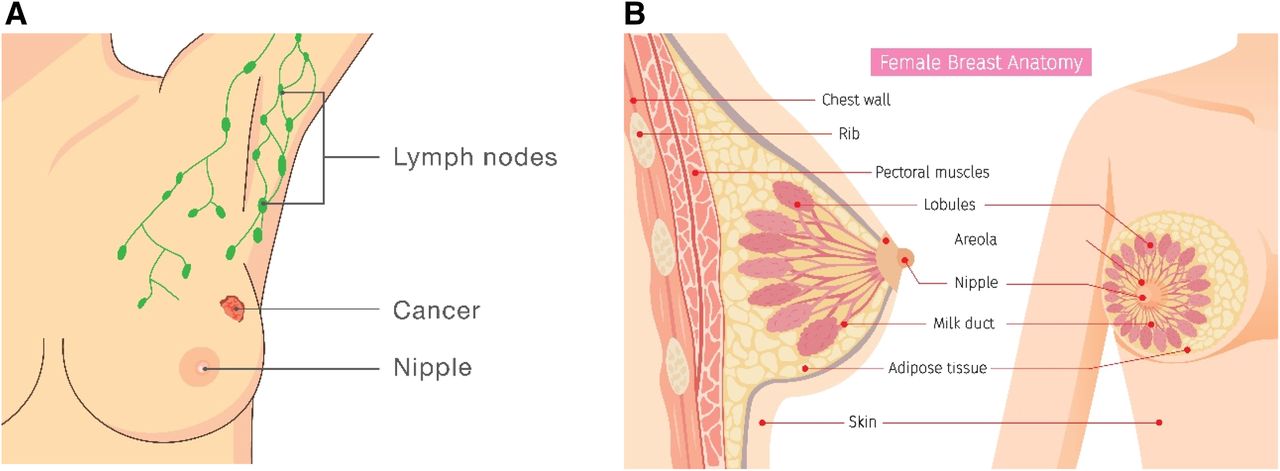
- FIGURE 1.
Illustrations of breast anatomy and lymphatic system. (A) Frontal view showing lymph nodes, cancer, and nipple. (B) Sagittal and frontal views showing additional anatomy. Critical structures when dealing with breast cancer are milk ducts, lobules, and nipple.
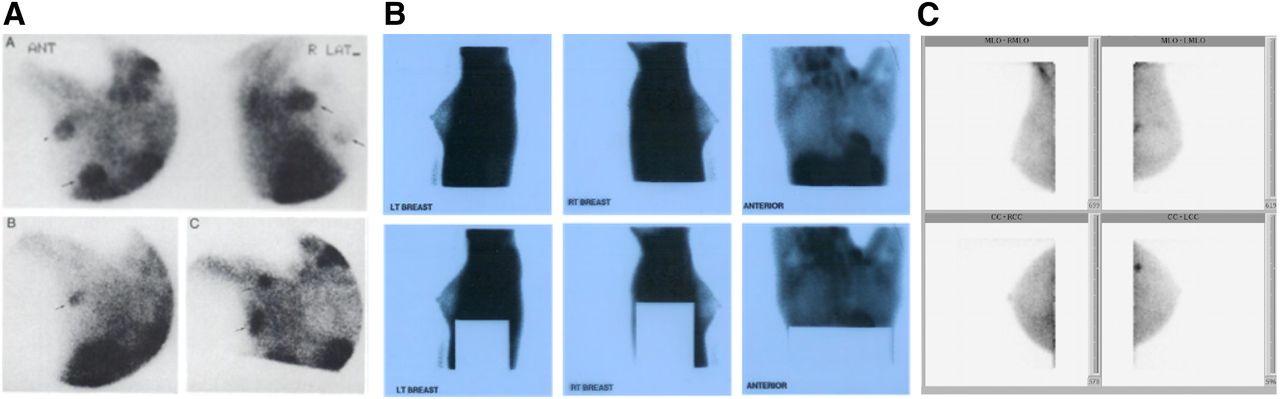
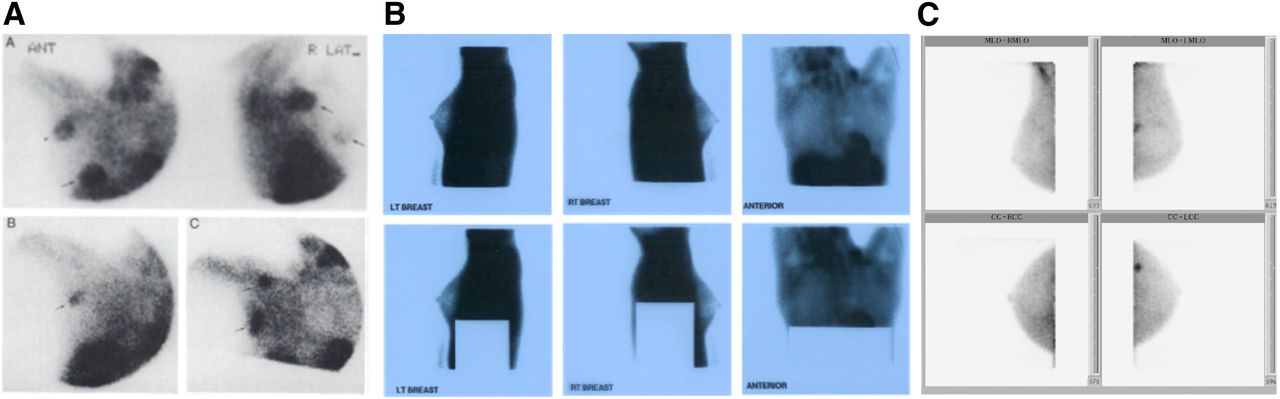
- FIGURE 2.
(A) Thallium images of breast from early 1990s (45). (B) Scintimammography images from 1998. (Courtesy of Union Hospital, Elkton, MD.) (C) 99mTc-sestamibi molecular breast images from 2012 (46).
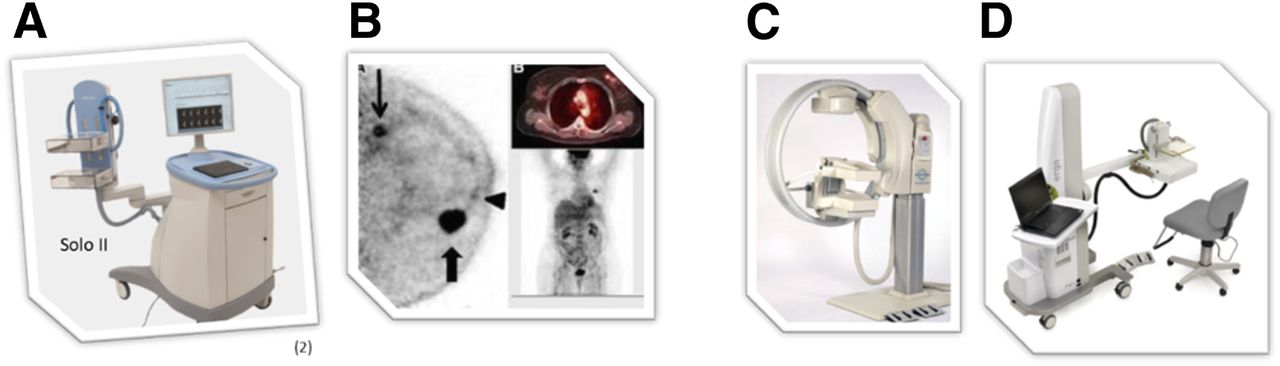
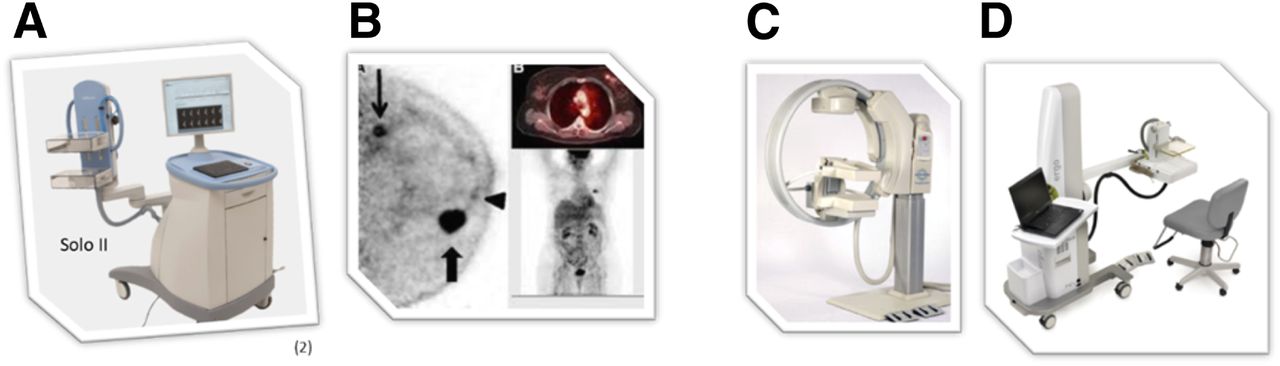
- FIGURE 3.
(A and B) Solo II (CMR Naviscan) PET-specific breast scanner (A) and PET mammography images obtained with it (B). (C and D) Two breast-specific γ-cameras: LumaGEM (CMR Naviscan) (C) and Ergo (Digirad) (D) (All images courtesy of the manufacturers.)
- FIGURE 4.
18F-fluoroestradiol case review 1. (A) Second 18F-FDG PET/CT study, 8 mo after treatment switch (from original treatment to new treatment), showing uptake in right ovary (arrow). (B) 18F-fluoroestradiol PET/CT 15 d after second 18F-FDG PET/CT study, showing expression of ERs by all lesions as indicated by 18F-fluoroestradiol uptake in chest and abdomen (arrows). (C) 18F-FDG PET/CT study 4 mo after initiation of fulvestrant hormone therapy (selective ER degrader that blocks and damages ERs), showing increase in ovarian uptake and emergence of bone uptake. Findings on second 18F-FDG scan (A) prompted question of whether ovarian primary cancer was present and whether hormone therapy would help. Biopsy of bone (yellow arrow) and ovarian (blue arrow) lesions was difficult. Bone lesion biopsy was noncontributory. (Courtesy of Zionexa.)
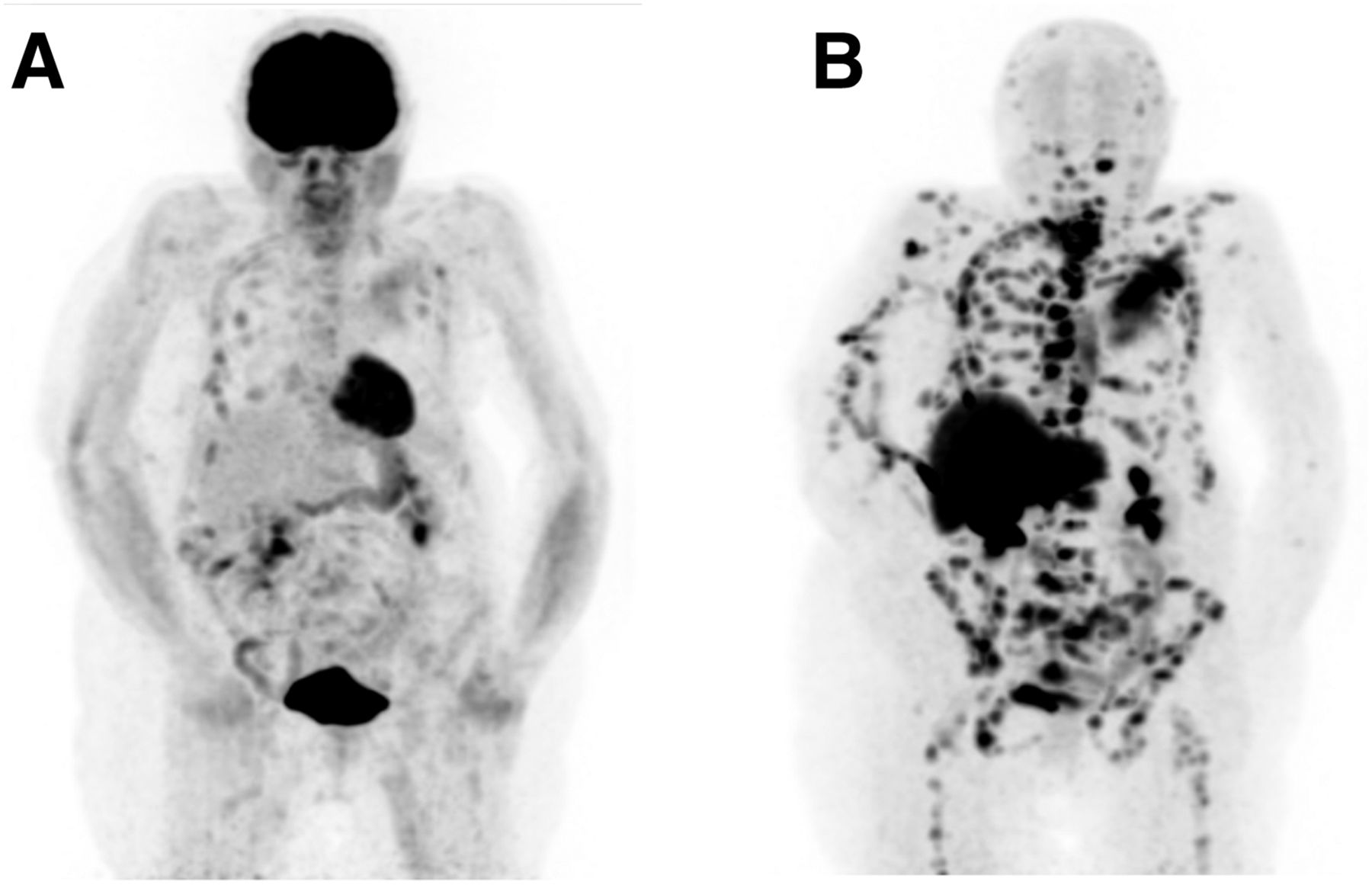
- FIGURE 5.
18F-fluoroestradiol case review 2. Patient had ER+, HER2−, T2N0M0 lobular carcinoma of left breast, which was treated with neoadjuvant chemotherapy, surgery, adjuvant chemotherapy, radiation therapy, and (for 5 y) tamoxifen hormone therapy. Eight years after total treatment completion (chemotherapy, surgery, radiation, and tamoxifen), vertebral fractures of T10 and T12 emerged, and cancer antigen 15-3 level was 3,500 U/mL (reference value, <25 U/mL). (A) 18F-FDG PET/CT study showing that some lesions were barely seen with 18F-FDG. (B) 18F-fluoroestradiol PET/CT study 1 d after 18F-FDG PET/CT study, showing that all lesions expressed ERs and that accumulation of 18F-fluoroestradiol was higher than that of 18F-FDG, probably because of lobular histology. Patient was subsequently treated with aromatase inhibitor (exemestane), resulting in lesion stabilization and cancer antigen 15-3 reduction to 150 U/mL 2 y after beginning treatment. (Courtesy of Zionexa.)
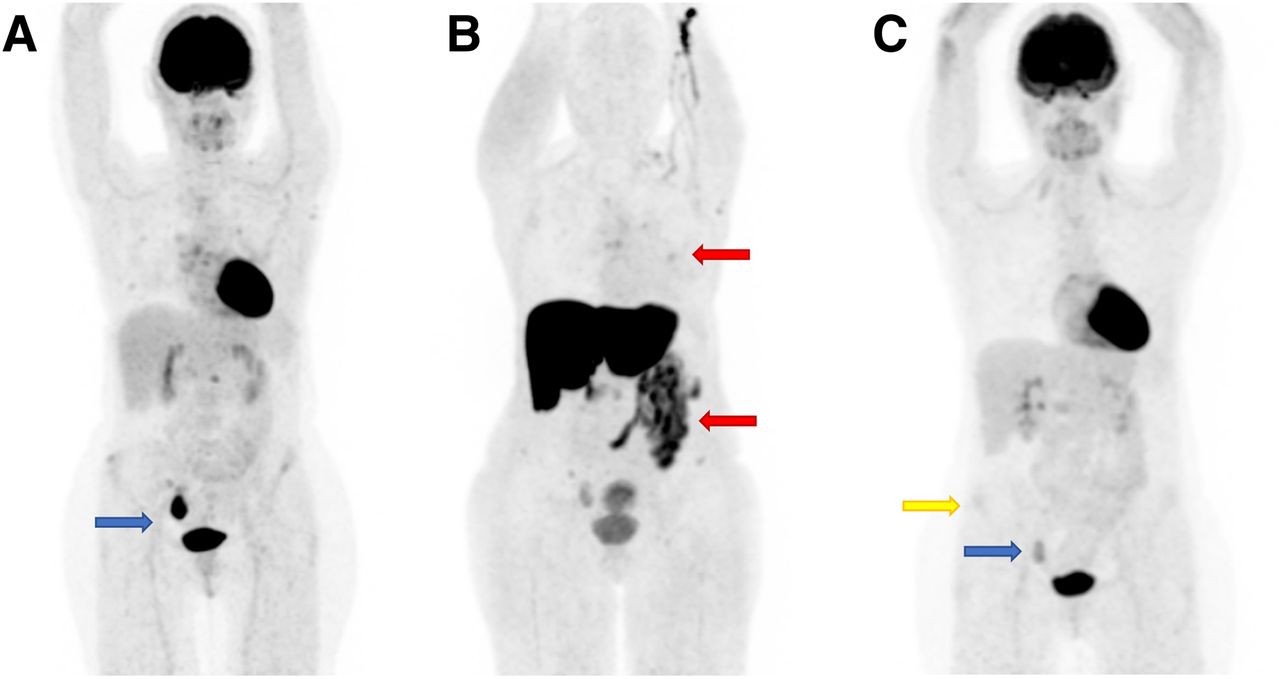
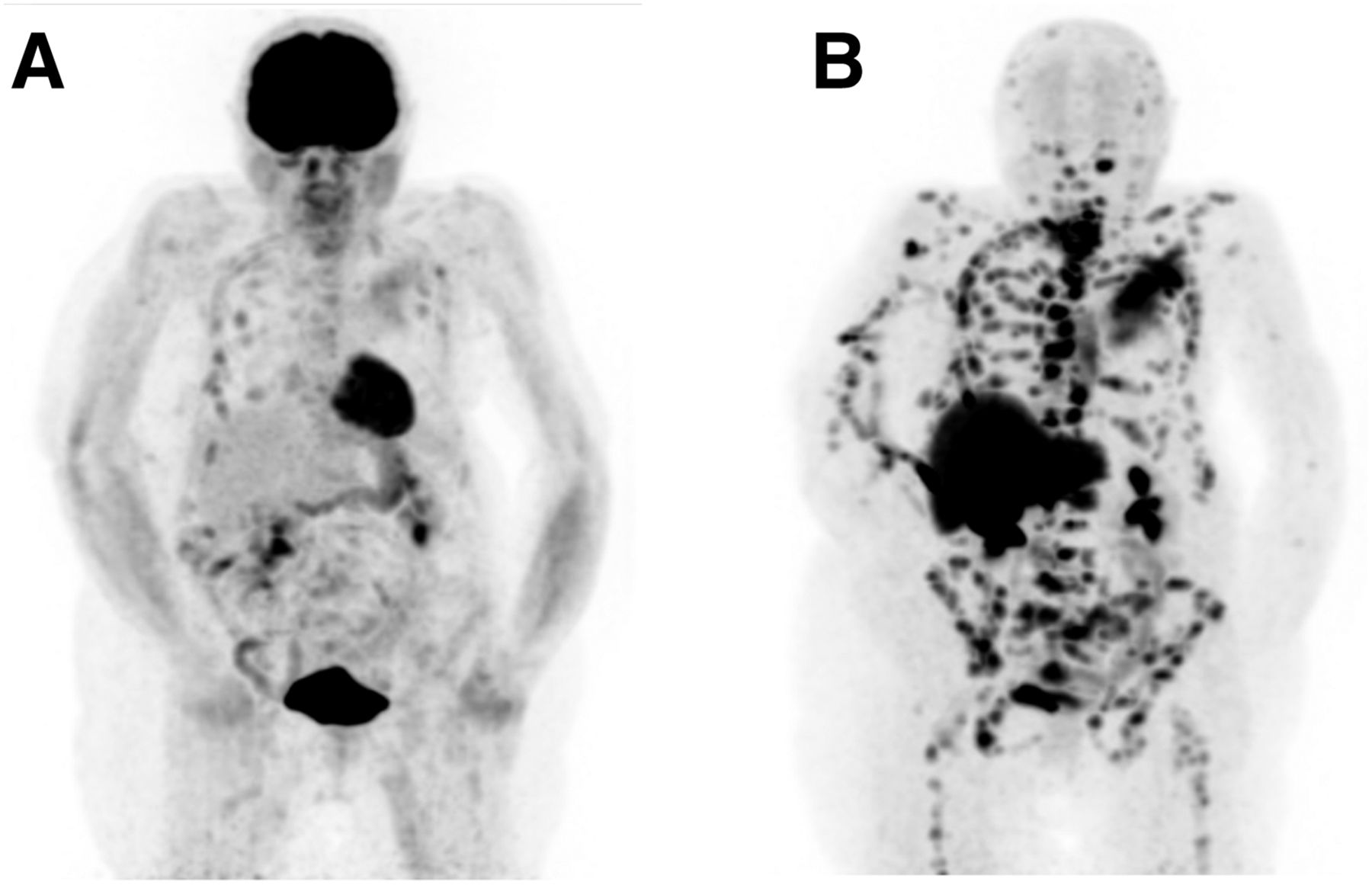
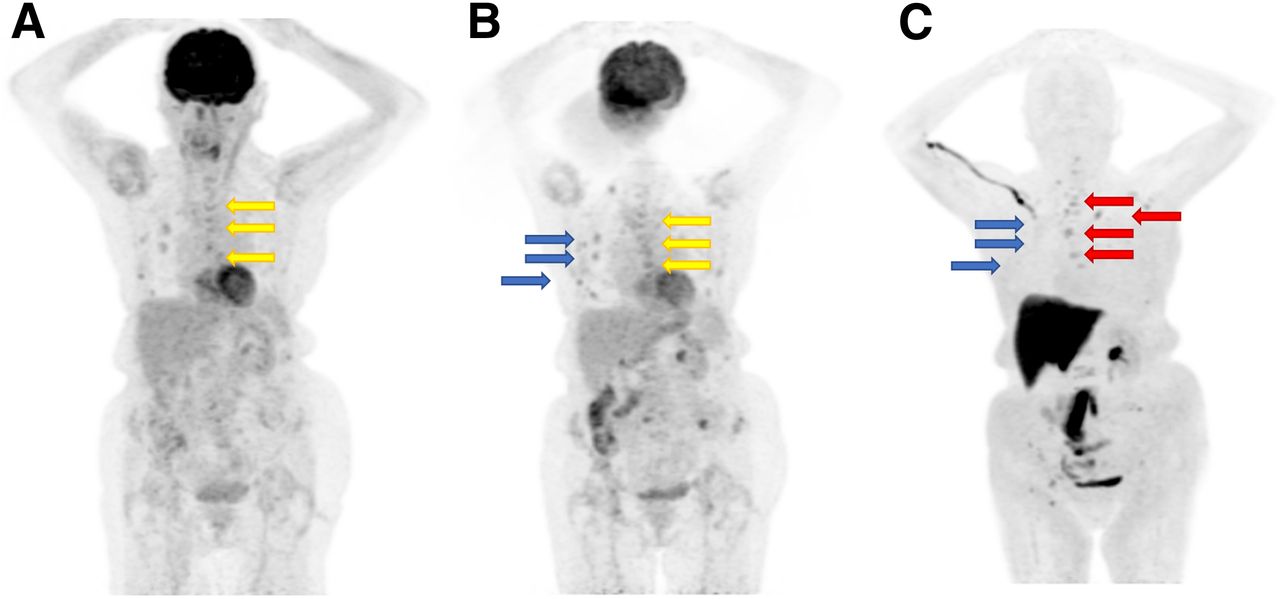
- FIGURE 6.
18F-fluoroestradiol case review 3. Patient had ER+, PR−, HER2− lobular carcinoma with initial bone metastases. (A) First 18F-FDG PET/CT study, showing lesions (arrows) that later showed progression. (B) Second 18F-FDG PET/CT study, showing progression of previously seen lesions (yellow arrows) and uptake in lesions that were subsequently negative for 18F-fluoroestradiol (blue arrows). (C) 18F-fluoroestradiol PET/CT study 1 mo after second 18F-FDG PET/CT study, showing 18F-fluoroestradiol–positive lesions (red arrows) corresponding to progressive lesions seen with 18F-FDG, but no uptake (blue arrows) where uptake was seen on second 18F-FDG PET/CT study. 18F-fluoroestradiol–positive lesions correspond to progressive lesions seen with 18F-FDG (yellow arrows). Treatment with aromatase inhibitor (which blocks ERs) resulted in reduction or disappearance of 18F-fluoroestradiol tracer uptake. Radiation therapy was performed on T9 and left iliac bone. Exemestane treatment resulted in bone progression in L5 and left iliac bone. (Courtesy of Zionexa.)
Tables
Type Characteristics Ductal carcinoma in situ Noninvasive BC that starts inside milk ducts, is not life-threatening, and increases risk that invasive BC will develop Invasive ductal carcinoma Most common type of BC (80% of all cases); more common in women over 55 y old Tubular carcinoma of breast Small tumors (∼≤1 cm); low-grade and slow-growing Medullary carcinoma of breast Rare; soft, fleshy mass, affecting women in their late 40s to early 50s; high-grade in appearance, low-grade in behavior; slow-growing; usually does not spread outside breast Mucinous carcinoma of breast (also called colloid carcinoma) Rare, usually occurring in postmenopausal women; abnormal cells that appear to float in pools of mucin (a key ingredient in mucus) Papillary carcinoma of breast Rare, usually occurring in older postmenopausal women; well-defined border; small, fingerlike projections; often classified as grade 2 Cribriform carcinoma of breast Invasion of breast connective tissues by cancer cells in nestlike formations between ducts and lobules, creating distinctive holes with Swiss cheese appearance; usually low-grade Invasive lobular carcinoma (also called infiltrating lobular carcinoma) Second most common type of BC (10% of all cases of invasive BC); becomes more common as women grow older (two thirds of cases are in women 55 y or older) Inflammatory BC Rare (1% of all cases of invasive BC) and aggressive; starts with reddening and swelling of breast instead of distinct lump; grows and spreads quickly; is more common in black women and can also affect men Lobular carcinoma in situ Lobules of abnormal cell growth that increase risk that invasive BC will develop later in life; occurs in premenopausal women (40–50 y old) and is extremely uncommon in men Male BC Rare (<1% of all cases of BC; in 2019, ∼2,670 men were expected to be diagnosed with BC) Molecular subtypes of BC, based on the genes expressed Luminal A, luminal B, triple-negative, and HER2-enriched (Table 2) Paget disease of nipple Rare (<5% of all BC cases in United States); cells collect in or around nipple; 97% of patients also have cancer elsewhere in breast (ductal carcinoma in situ or invasive cancer); unusual changes in nipple and areola are often first indication that BC is present Phyllodes tumors of breast Rare (<1% of all breast tumors); called phyllodes (“leaflike,” in Greek) because tumor cells grow in leaflike pattern; tends to grow quickly; rarely spreads outside breast Metastatic (stage IV) BC Spread of cancer to liver, brain, bones, or lungs; will occur in 30% of women diagnosed with early-stage BC (if in bone, metastatic tumor comprises BC cells, not bone cells) Type Expression Characteristics Prognosis Therapy Luminal A HR+/HER2− Slow-growing, less aggressive than other subtypes Favorable prognosis, particularly in short term Antihormone therapy Luminal B HR+/HER2+ Highly positive for Ki-67 (indicator of large proportion of actively dividing cells) or HER2; tends to be higher-grade Poorer survival than for luminal A cancers Chemotherapy, hormone therapy, and treatments targeting HER2 receptor Triple-negative HR−/HER2− (ER−, PR−, and HER2−) Twice as common in black women as in white women in United States; more common in premenopausal women and those with BRCA1 gene mutation Poorer short-term prognosis than for other subtypes No current targeted therapy HER2-enriched HR−/HER2+ Grows and spreads more aggressively than other subtypes Poorer short-term prognosis than for HR+ breast cancers; recent widespread use of targeted therapies for HER2+ cancers has improved outcomes Combination of surgery, radiation therapy, chemotherapy, or targeted therapy such as the immune monoclonal antibody trastuzumab *The different subtypes differ in risk factors, presentation, response to treatment, and outcome. Techniques to profile tumor gene expression allow better understanding of subtypes but are costly and complex. Subtypes are approximated using biologic markers, including presence or absence of ER or PR and excess levels of HER2 or extra copies of HER2 gene (HER2+/HER2−) (5,48).
Parameter Description Characteristic Tubule formation Amount of tumor tissue with normal breast (milk) duct structures Nuclear grade Size and shape of nucleus in tumor cells Mitotic rate Number of dividing cells (measure of how fast tumor cells grow and divide) Points* 1 Cells and tumor tissue look most normal 3 Cells and tumor tissue look most abnormal Grade 1 (3–5 total points) Low (well differentiated; slower growing, less likely to spread) 2 (6–7 total points) Intermediate (moderately differentiated) 3 (8–9 total points) High (poorly differentiated; faster growing, more likely to spread) *Points are assigned to tumor for the 3 characteristics. Total score ranges from 3 to 9, corresponding to grade 1, 2, or 3 (11,49).
Treatment options Invasive BC by stage Stage Treatment option 1. BCS alone Stages I and II BCS + RT (34%) 2. BCS + RT BCS + RT + chemo (17%) 3. BCS + RT + chemo Mastectomy alone (17%) 4. BCS + chemo Mastectomy + chemo (12%) 5. Mastectomy alone Stage III Mastectomy + RT + chemo (48%) 6. Mastectomy + RT BCS + RT + chemo (15%) 7. Mastectomy + chemo Mastectomy + chemo (13%) 8. Mastectomy + RT + chemo Mastectomy alone (7%) 9. RT or chemo Stage IV RT or chemo (48%) 10. No surgery, RT, or chemo No surgery, RT, or chemo (21%) Mastectomy + RT + chemo (7%) Mastectomy + chemo (7%) BCS = breast-conserving surgery; RT = radiation therapy; chemo = chemotherapy, including targeted therapy and immunotherapy drugs.
Source: (5).
Benefits of molecular imaging Limitations and risks of biopsy Stages cancer Is invasive Predicts response to therapy Is restricted to accessible lesions Monitors and evaluates therapeutic benefit Has limited ability to be repeated Advances personalized medicine and targeted therapy Has risk of disseminating tumor cells Images a specific biomarker (ER) Has shorter image acquisition time - TABLE 6
Diagnostic Performance of 18F-Fluoroestradiol PET Versus Immunohistochemistry in 12 Studies
Definition of ER+ Study n Sensitivity Specificity IHC PET Peterson (31) Nonbreast 10 0.99 (0.67–1) 0.96 (0.33–1) Allred score > 2 SUVmean > 1.5 Breast 4 0.98 (0.50–1) Indeterminate Allred score > 2 SUVmean > 1.5 Venema (37) 13 0.99 (0.73–1) 0.96 (0.33–1) ≥1% of cells SUVmax > 1.5 Gemignani (29) 48 0.85 (0.71–0.93) 0.74 (0.41–0.93) ≥1% of cells SUVmean > 1.5 Yang (35) 18 0.99 (0.73–1) 0.85 (0.48–0.97) ≥1% of cells SUVmax > 1.5 Peterson (38) Nonbreast 3 0.97 (0.43–1) 0.96 (0.33–1) ≥5% of cells SUVmean > 1 Breast 9 0.99 (0.69–1) 0.66 (0.21–0.93) ≥5% of cells SUVmean > 1 Gupta (39) Nonbreast 4 0.98 (0.50–1) Indeterminate All ER+ were ≥15% of cells Qualitative Breast 6 0.98 (0.60–1) Indeterminate Unclear location 2 Chae (40) 85 0.77 (0.63–0.86) 1.00 (0.90–1) Allred score ≥ 3 Qualitative Chae (30) 24 0.92 (0.75–0.98) Indeterminate Allred score ≥ 6 Qualitative Dehdashti (41) 11 0.69 (0.44–0.86) 1 (0.83–1) RBA, >3 fmol/mg or IHC* Qualitative Mintun (42) 8 0.99 (0.67–1) 0.05 (0–0.67) RBA, >3 fmol/mg Qualitative Mortimer (43) 16 0.76 (0.55–0.89) 1 (0.83–1) RBA, >3 fmol/mg or IHC* Qualitative van Kruchten (4) 22 0.95 (0.79–0.99) 0.99 (0.71–1) IHC* or clinical outcome SUVmax > 1.5 ↵* Criteria not stated.
IHC = immunohistochemistry; RBA = radioligand binding affinity (50).
Data in parentheses are 95% confidence intervals.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- BREAST CANCER FACTS AND STATISTICS
- BREAST CANCER SURVIVAL RATES AND TRENDS
- TYPES OF BREAST DISEASE AND BREAST TUMORS
- BREAST CANCER STAGING
- BREAST CANCER TREATMENT OPTIONS
- IMAGING MODALITIES FOR BREAST CANCER
- NUCLEAR MEDICINE AND MOLECULAR BREAST IMAGING…A LOOK BACK
- NUCLEAR MEDICINE AND MOLECULAR BREAST IMAGING…A LOOK AHEAD
- 18F-FLUOROESTRADIOL PET BASICS
- CURRENT TREATMENT OPTIONS FOR ER+ AND ER− PATIENTS
- POTENTIAL BENEFITS OF 18F-FLUOROESTRADIOL PET
- CONCLUSION
- DISCLOSURE
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics