


Abstract
Postsurgical anatomic alterations and placement of prosthetic materials may cause misdiagnosis, leading to unnecessary patient work-up. Reading physicians must be aware of common and uncommon postoperative imaging appearances and their pitfalls. In this case report, we present the appearance of a postsurgical hernia repair plug on PET/CT, also called plugoma or meshoma.
A large number of hernia-related surgeries are conducted every year, with many involving the use of prosthetic plugs and mesh. The changes may be visible or seldom hardly discernible on CT imaging depending on their density, structure, and thickness. These prosthetic materials may cause variable degree of inflammatory reaction, giving them the appearance of a soft-tissue mass. Knowledge of such prosthetic implants is important to decrease the chances of misdiagnosis.
CASE REPORT
A 65-y-old man presented with history of cough. His recent CT scan demonstrated bilateral lung nodules and enlarged mediastinal lymph nodes. 18F-FDG PET/CT was performed to evaluate the metabolic activity of the lung nodules for presurgical planning. The standard method of 18F-FDG PET/CT acquisition was followed (18F-FDG was injected after determining the patient’s blood sugar level, and whole-body PET/CT was performed after 60 min on a Philips TOF PET/CT scanner).
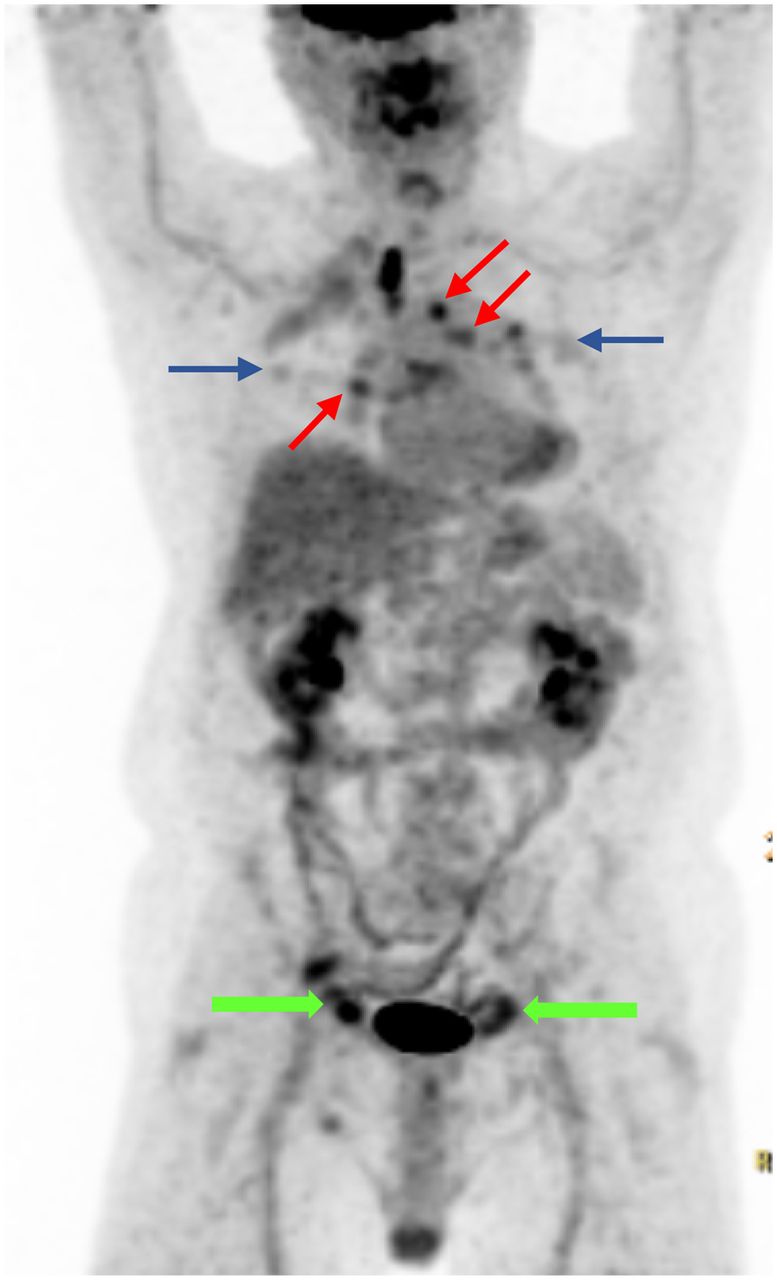
The PET scan demonstrated multiple 18F-FDG avid bilateral lung nodules and mildly avid mediastinal lymph nodes (Fig. 1). An incidental finding of hypermetabolic soft-tissue density was noted bilaterally in the inguinal region, with adjacent stranding (Fig. 2). A further search into the patient’s history revealed remote hernia repair surgery, performed nearly 12–14 years ago. The patient was otherwise asymptomatic from abdominal point of view.

18F-FDG PET maximum-intensity projection (MIP image) demonstrating FDG avid bilateral lung nodules (blue arrow), mediastinal lymph nodes (red arrow), and soft-tissue nodules in bilateral inguinal canal (green arrow).

18F-FDG PET transaxial image (A), fused PET/CT transaxial image (B), and fused PET/CT coronal image (D) demonstrate focal to linear moderately intense FDG avid soft tissue (white arrow) in bilateral inguinal canal. Noncontrast CT transaxial image (C) shows nodular soft-tissue density in bilateral inguinal canal with surrounding mild fat stranding. In context of prior history of bilateral inguinal hernia repair, findings are most consistent with presence of ‘plugoma.’
Histopathologic examination of the lung nodules was suggestive of granulomatous disease.
DISCUSSION
Hernia mesh or plugs are usually impregnated with a protective membrane or film to minimize any possible host reaction and to decrease the dreaded complications of adhesion, bowel erosion, or fistula formation (1). Even with use of the protective film, a multitude of host reactions occur at the surface of the mesh, causing varying degrees of inflammation and matrix deposition. Finally, there is formation of connective tissue, which, over time, forms into a thick, rigid scar called a meshoma or plugoma (2). Its characteristics depend on the specific properties of the prosthetic material (light-weight to extremely heavy-weight mesh) (3). Plugomas may show hypermetabolism on 18F-FDG PET/CT scans, with the metabolic activity directly proportional to the severity of the inflammatory reaction. 18F-FDG uptake related to such inflammatory processes can be seen for many years, even after the wound is clinically healed and stable. In this patient, moderately intense 18F-FDG uptake was noted bilaterally in the inguinal canals, correlating with the history of bilateral inguinal hernia repair. These findings may mimic metastases on 18F-FDG PET/CT scans. A thorough look into the patient’s history is required for complete evaluation.
CONCLUSION
Recognition of the 18F-FDG PET/CT appearance of plugoma is important to avoid misdiagnosis and unnecessary further patient work-up.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 28, 2020.
- Received for publication July 31, 2019.
- Accepted for publication January 3, 2020.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.