


Abstract
A 56-y-old man underwent total thyroidectomy and bilateral central and right lateral neck dissection for papillary thyroid carcinoma with lymph nodes metastases. Before radioiodine ablation, a 123I scan established the diagnosis of primary nasolacrimal duct obstruction (dacryostenosis).
Patients with nasolacrimal duct obstruction can present with epiphora (excessive tear accumulation with subsequent overflow) or blurred vision (from an increased tear lake). Adult-onset nasolacrimal duct obstruction is classified as primary or secondary. The primary form is considered idiopathic, and the secondary causes are numerous, including inflammation (either endogenous or exogenous, the latter including radiation and radioiodine therapies), infection, neoplasm, surgery, and trauma (1,2).
CASE REPORT
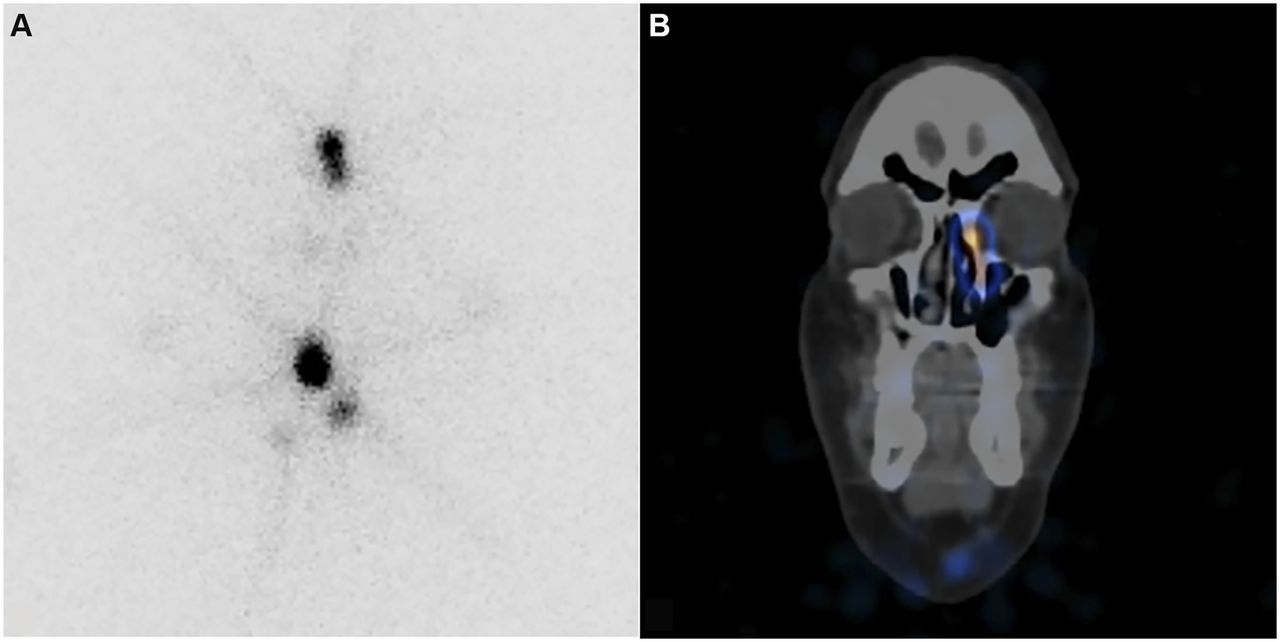
A 56-y-old man with extensive cervical lymphadenopathy due to papillary thyroid carcinoma underwent total thyroidectomy and bilateral central and right lateral neck dissection. The radioiodine ablation work-up included a pretherapy 123I scan (Fig. 1) that demonstrated left nasolacrimal duct obstruction (dacryostenosis). The nasolacrimal duct obstruction was again present on the posttherapy 131I scan (Fig. 2). On further questioning, the patient did not describe epiphora or blurred vision, suggesting that the nasolacrimal duct obstruction was incomplete. If nasolacrimal duct obstruction is present on pretherapy 123I imaging, it allows differentiation of primary nasolacrimal duct obstruction from nasolacrimal duct obstruction secondary to radioiodine iodine ablation.
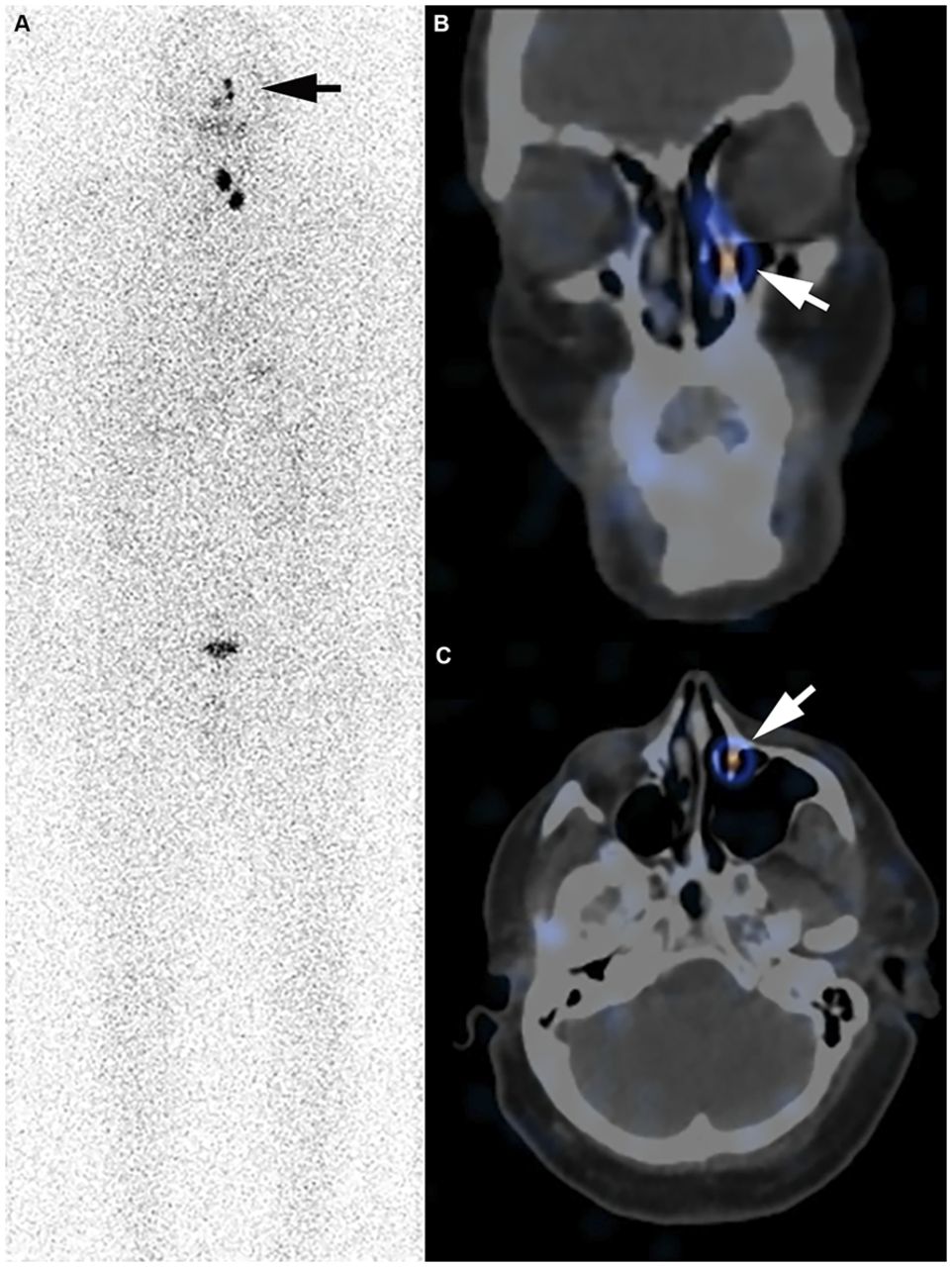
Postoperative, pretherapy 123I whole-body scan (A) and corresponding SPECT/CT of head and neck in coronal (B) and axial (C) planes demonstrate linear left nasolacrimal duct uptake (arrows) consistent with nasolacrimal duct obstruction or dacryostenosis.

Posttherapy 131I planar images of neck (A) and SPECT/CT of head and neck in coronal plane (B) reconfirm nasolacrimal duct obstruction.
DISCUSSION
Tears drain from the eyes medially via superior and inferior lacrimal canaliculi into the lacrimal sac. The lacrimal sac is seated within an osseous groove formed at the junction of the lacrimal bone and the frontal process of the maxilla. The lacrimal sac is contiguous inferiorly with the nasolacrimal duct. It functions as a reservoir for excess tears that are relayed through multiple mucous membrane folds of the nasolacrimal duct (many with eponymous names) into the inferior meatus of the nasal cavity. Nasolacrimal duct obstruction may result in epiphora or blurred vision. The incidence of nasolacrimal duct obstruction after radioiodine ablation is reported to range from 2.2% to 18% (2), but this may be an overestimation since cases without pretherapy imaging may actually be examples of primary nasolacrimal duct obstruction. Nasolacrimal duct obstruction secondary to radioiodine ablation is more likely to occur bilaterally within 6–18 mo after treatment with doses of greater than 5,550 MBq (3). The transmembrane cotransporter of sodium and iodide (sodium-iodide symporter) highly expressed by the follicular cells of the thyroid is also responsible for radioiodine secretion into the nasolacrimal drainage system, leading to localized radiotoxicity with potential for secondary nasolacrimal duct obstruction (4). Defining the etiology of nasolacrimal duct obstruction has prognostic implications, because external or endoscopic dacryocystorhinostomy (the formation of an anastomosis between the lacrimal sac and the nasal mucosa to bypass the nasolacrimal duct obstruction) is more likely to succeed in patients with primary nasolacrimal duct obstruction than in those with secondary nasolacrimal duct obstruction due to radioiodine ablation or radiotherapy (5). This case demonstrates an additional benefit of pretherapy radioiodine imaging before radioiodine ablation of differentiated thyroid cancers.
CONCLUSION
Pretherapy radioiodine imaging can differentiate primary from secondary nasolacrimal duct obstruction due to radioiodine therapy, and the primary form is more likely to improve with intervention.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 11, 2019.
REFERENCES
- Received for publication August 9, 2019.
- Accepted for publication August 29, 2019.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.