


Abstract
We report a case of concurrent nodular fasciitis and incidental giant intraperitoneal lipoma diagnosed on whole-body 18F-FDG PET/CT, an imaging modality that has the advantage of being able to detect unsuspected lesions.
Nodular fasciitis is a benign reactive proliferation of fibroblasts sometimes misdiagnosed as sarcoma on the basis of cellularity and rapid growth. Giant intraperitoneal lipomas are quite rare, and most are reported as liposarcoma because of their large size. Although liposarcomas make up only 0.1% of all human neoplasms, they are the most common histologic subtype of retroperitoneal soft-tissue sarcoma. This paper reports a case in which nodular fasciitis and incidental giant intraperitoneal lipoma concurred in a patient who underwent whole-body 18F-FDG PET/CT. 18F-FDG PET/CT plays a fundamental role in the differentiation of benign and malignant lesions and in the detection of unsuspected lesions.
CASE REPORT
We present a 33-y-old woman with no relevant medical or surgical history in whom a tumor in the right axillary area had been evolving for several months. Right axillary sonography, which was performed first, showed a heterogeneous solid mass measuring approximately 2 × 2.5 cm in the external region of the right axilla. The mass had no Doppler flow and was located between muscle masses. Because these findings might be compatible with intramuscular hematoma but cannot exclude underlying tumor, MRI was performed. It showed a nodular, lobulated, well-defined lesion in the right quadrilateral space, compatible with a neural tumor or paralabral cyst.
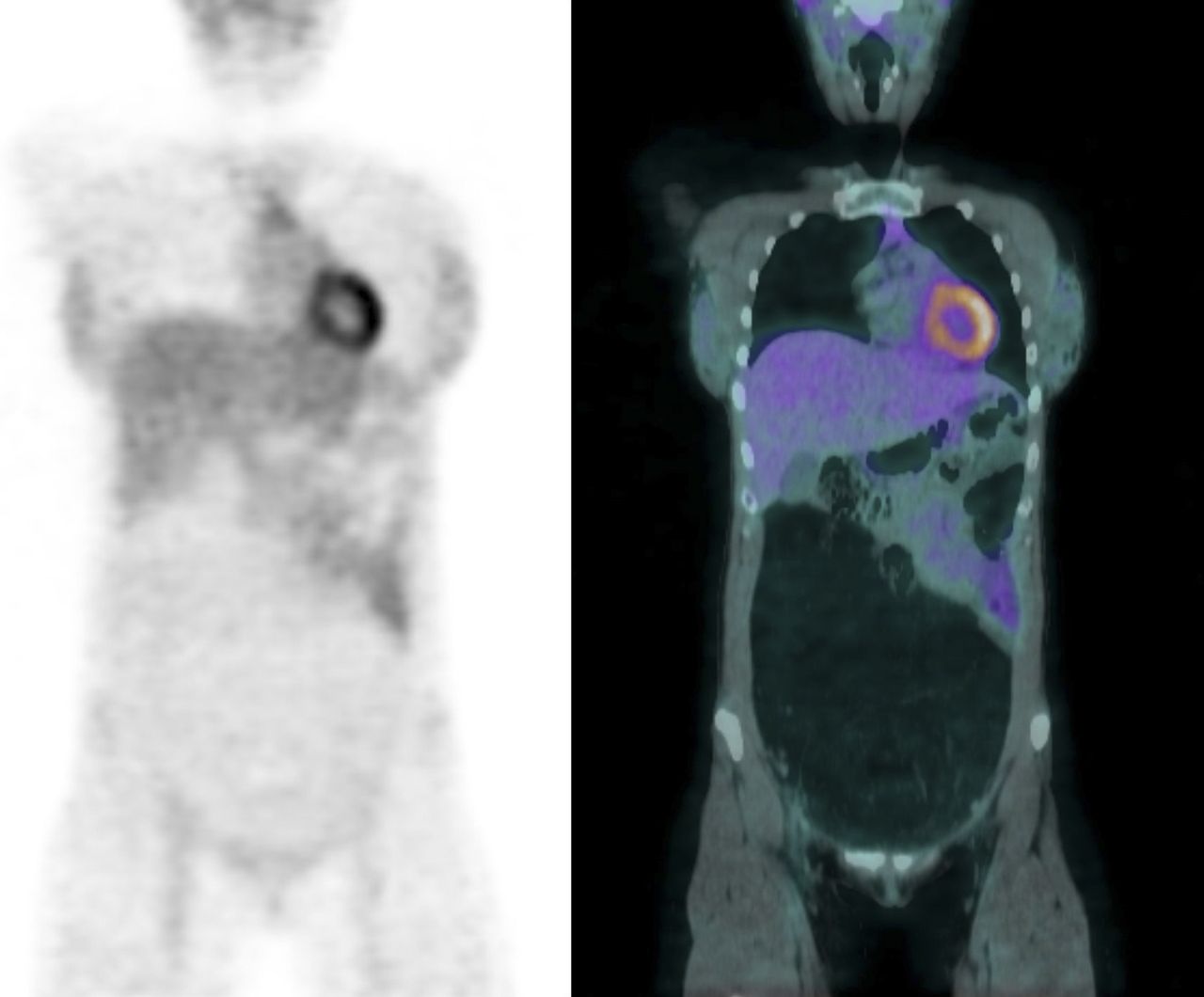
It was decided to perform sonography and fine-needle aspiration of the lesion, which showed a mesenchymal proliferation with scarce-to-moderate cellularity and a myxoid stroma, potentially compatible with myxoid sarcoma. Surgical exeresis was planned, and 18F-FDG PET/CT was requested to determine the extent of the lesion before surgery. PET/CT images taken 60 min after the intravenous administration of 370 MBq of 18F-FDG showed a slight metabolic increase (SUVmax of 1.9) in the right brachial lesion, suggesting a benign lesion but not being able to totally dismiss the possibility of a malignant lesion of low histologic grade and low affinity for 18F-FDG (Fig. 1). Likewise, as an incidental finding on the PET/CT images, a giant abdominopelvic mass of fat density and more than 30 cm in craniocaudal length was observed displacing the abdominal contents toward the left hypochondrium and flank; this mass did not present a metabolic increase (Figs. 2 and 3).

Right brachial nodular fasciitis on axial PET (top), CT (middle), and PET/CT (bottom). Slight focal metabolic increase, with SUVmax of 1.9, is seen in posterior region of right shoulder.
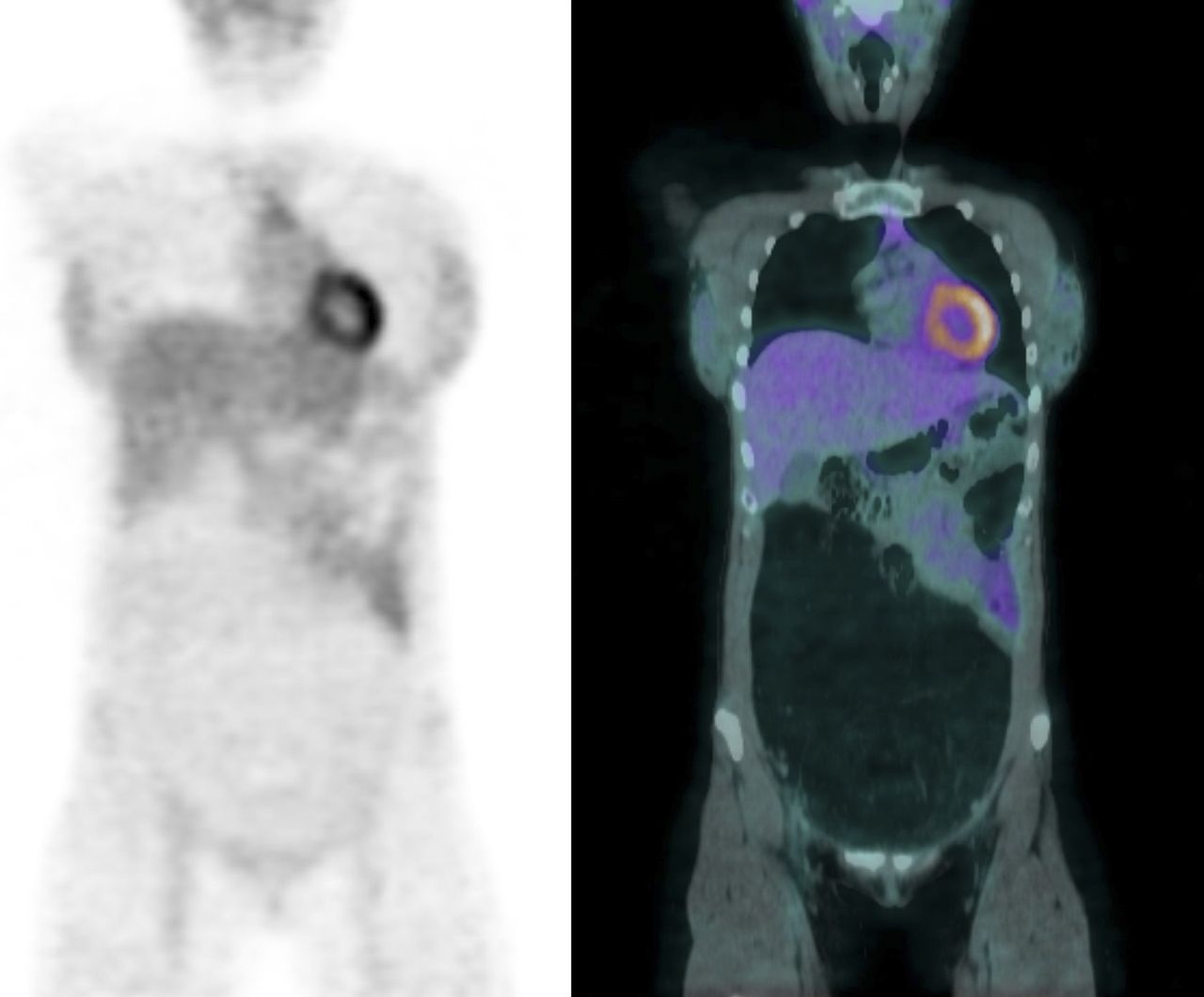
Giant intraperitoneal lipoma on coronal PET (left) and PET/CT (right). Giant intraabdominal mass of fat density is seen displacing abdominal content toward left hypochondrium and flank, without uptake on PET.
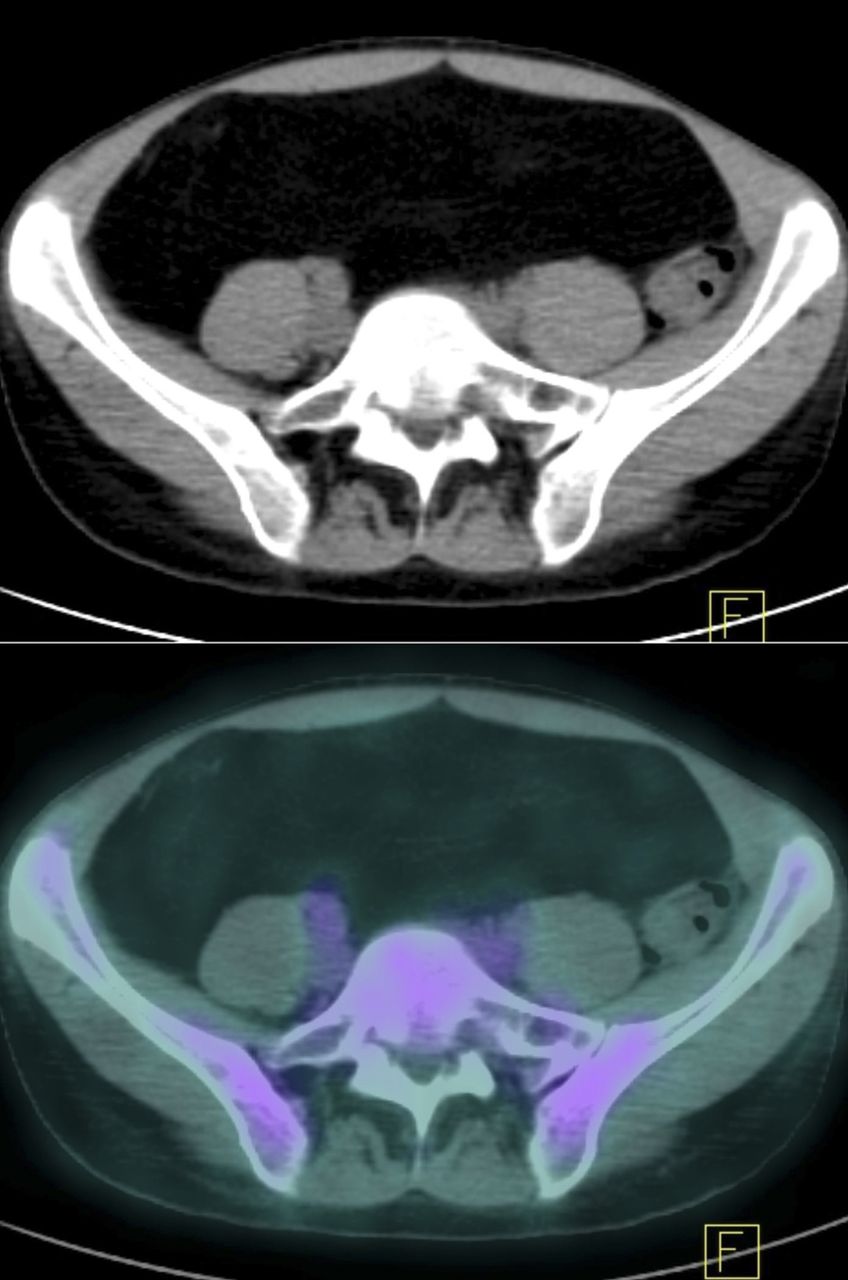
Giant intraperitoneal lipoma as seen on axial CT (top) and PET/CT (bottom).
In view of these findings, we took a deeper medical history, and this time the patient recalled experiencing a progressive abdominal distension occurring over a span of years, which she had interpreted as digestive intolerance. Abdominal MRI was performed and showed a large fatty mass with no large vessels or infiltration into adjacent organs.
In view of the diagnostic doubt about the atypical lipomatous tumor, which because of its enormous size might have been a liposarcoma, as well as the diagnosis of a possible brachial myxoid sarcoma, the patient underwent surgery. The brachial lesion was accessed with radical excision, and in the abdomen, a supraumbilical–infraumbilical midline incision revealed a large lipomatous pedunculated mass depending from subperitoneal fatty tissue at the level of the right iliac wall.
The definitive anatomic–pathologic diagnosis was nodular fasciitis for the brachial lesion and giant intraperitoneal lipoma for the abdominal lesion, with no malignant cells found in either of the 2 tumors.
DISCUSSION
Nodular fasciitis is a benign, rapidly growing, self-limiting proliferation of fibroblasts that originates in subcutaneous tissue or skeletal muscle and frequently undergoes spontaneous regression (1). Histologically, it can simulate a sarcoma because of the irregularity of the fibroblasts, which are randomly arranged in a myxoid stroma. Regarding imaging diagnosis, the appearance on MRI and sonography is quite variable and difficult to characterize. PET shows a mild hypermetabolic focus, ovoid and well circumscribed, at the muscular level, between muscles, or adjacent to tendons. Rapid growth, high cellularity, and high mitotic activity may be responsible for the metabolic increase on PET; however, both malignant and benign masses can show hypermetabolic activity; likewise, some malignant lesions may show only slight uptake because of acellularity or avascularity (2).
In our patient, giant intraperitoneal lipoma was an incidental finding on PET/CT. Lipomas are benign mesenchymal tumors that appear similar to normal fat. They can be found at any location, although intraperitoneal, omental, and mesenteric locations are exceptional (3). In this patient, the main concern in the diagnosis was potential malignancy because the large size of the lesion did not eliminate the possibility of well-differentiated liposarcoma, which can look similar to lipomas on conventional imaging (4,5).
CONCLUSION
18F-FDG PET/CT is a useful tool for discriminating the benign nature of 2 independent lesions that are creating diagnostic doubt. When used for full-body imaging, 18F-FDG PET/CT has the advantage of being able to detect unsuspected lesions—a capability that, in this case, led to the diagnosis of a huge, asymptomatic abdominal lesion.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 24, 2019.
- Received for publication September 13, 2018.
- Accepted for publication January 7, 2019.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.