


Abstract
99mTc-tagged red blood cell scintigraphy is the imaging modality of choice in the diagnosis of active gastrointestinal bleeding. Continuous-flow left ventricular assist devices are the state-of-the-art treatment for advanced heart failure, with gastrointestinal bleeding as the most common complication. Recognition of the distinctive imaging feature of continuous-flow left ventricular assist devices on scintigraphic images can aid diagnosis of gastrointestinal bleeding.
About 5 million patients have heart failure in the United States (1). In the past decade, continuous-flow left ventricular (LV) assist devices have replaced their pulsatile-flow predecessors and become the mainstay of treatment in patients with end-stage heart failure, as either the bridge to heart transplantation or the destination therapy. However, there is an increased incidence of gastrointestinal bleeding after placement of continuous-flow LV assist devices, which could be as high as 23% and with a recurrent gastrointestinal bleeding rate of 9.3% (2,3). Endoscopy has been the first choice in evaluation and treatment of this iatrogenic complication. 99mTc-tagged red blood cell scintigraphy is the most sensitive imaging tool in localization of active gastrointestinal bleeding. In this report, we present scintigraphy images of active gastrointestinal bleeding in the recipient of a continuous-flow LV assist device and aim to familiarize the readers with the unique imaging features of the device.
CASE REPORT
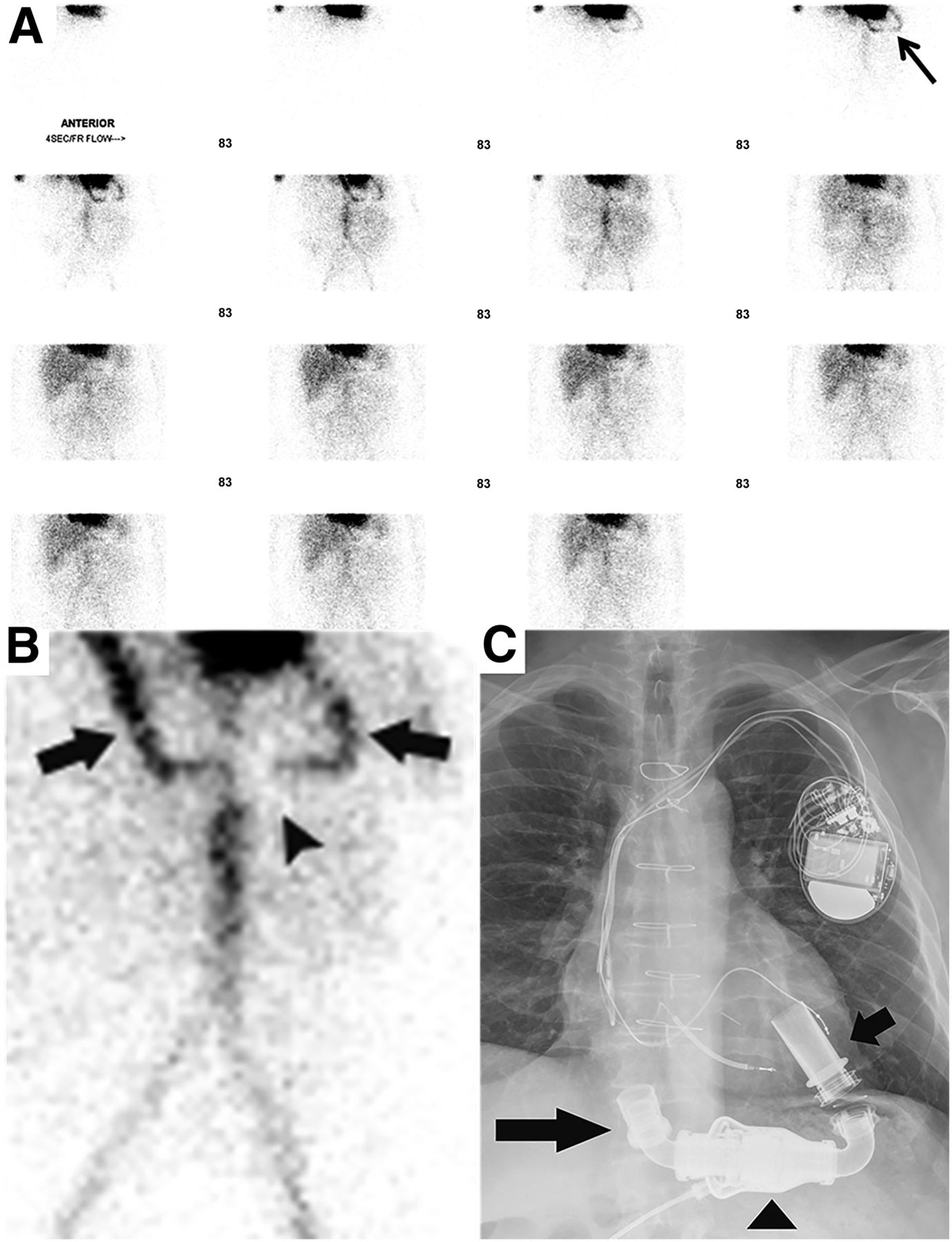
A 74-y-old man with a history of end-stage heart failure received a HeartMate II (Thoratec Corp.) continuous-flow LV assist device as destination therapy. Two months after its implantation, the patient was hospitalized for recurrent episodes of melena and anemia. 99mTc-tagged red blood cell scintigraphy was performed to confirm and localize the ongoing gastrointestinal bleeding. On the first-minute flow images, there was an overlooked continuous-flow LV assist device artifact overlying the partially visualized cardiac chambers (Fig. 1). The artifact was persistent throughout the remaining 60-min dynamic images, along with proximal small-bowel bleeding (Fig. 2). Immediate upper endoscopy confirmed focal mucosal angiodysplasia in the jejunum. Hemostasis was achieved after thermal therapy.
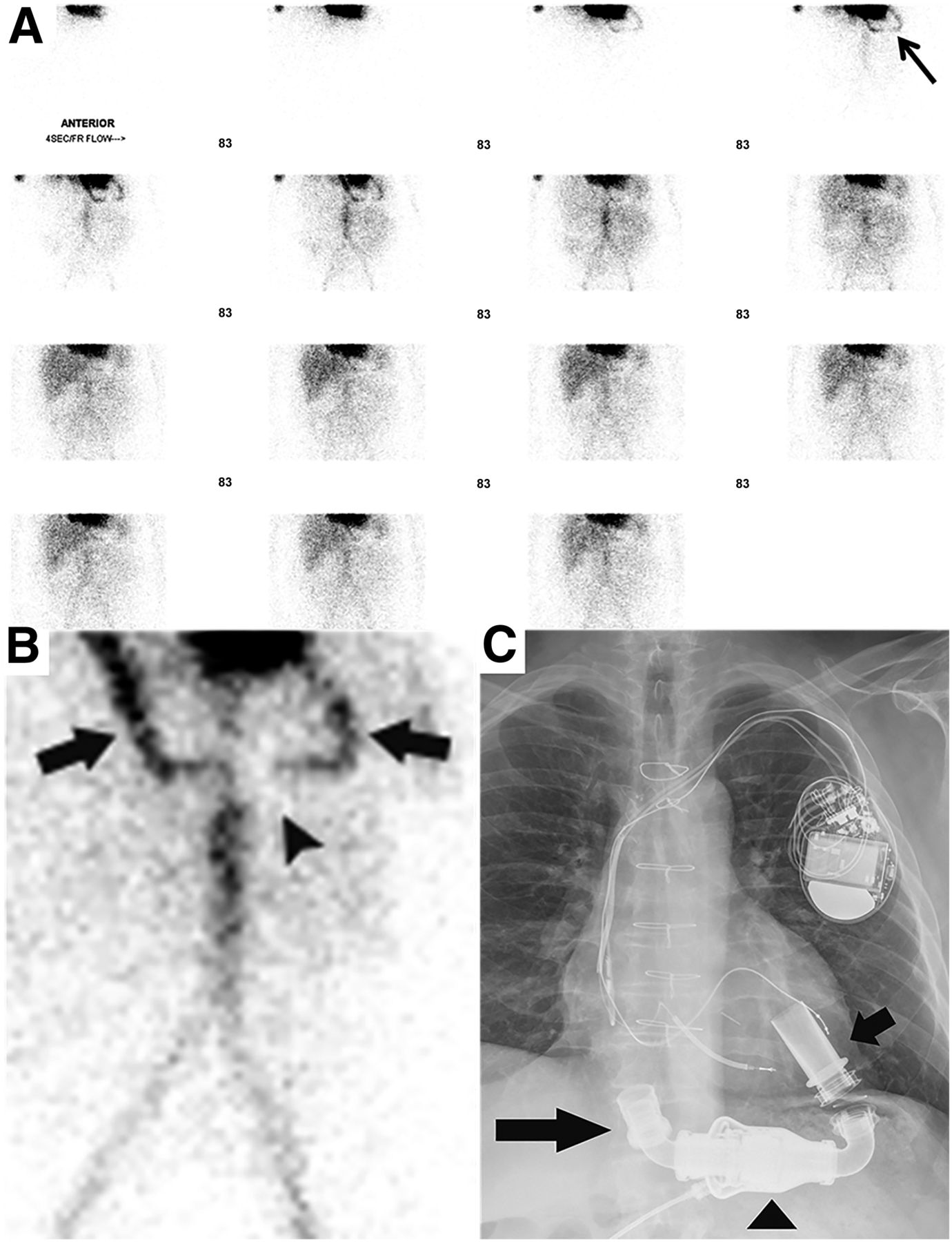
First-minute flow images (4 s/frame). (A and B) U-shaped flow artifact was overlying partially visualized cardiac chambers (arrow in A) and was more conspicuous on magnified 16-s image (arrows and arrowhead in B). (C) Findings corresponded with inflow and outflow conduits (arrows) and pump (arrowhead) of implanted continuous-flow left ventricle assist device demonstrated by chest radiography.
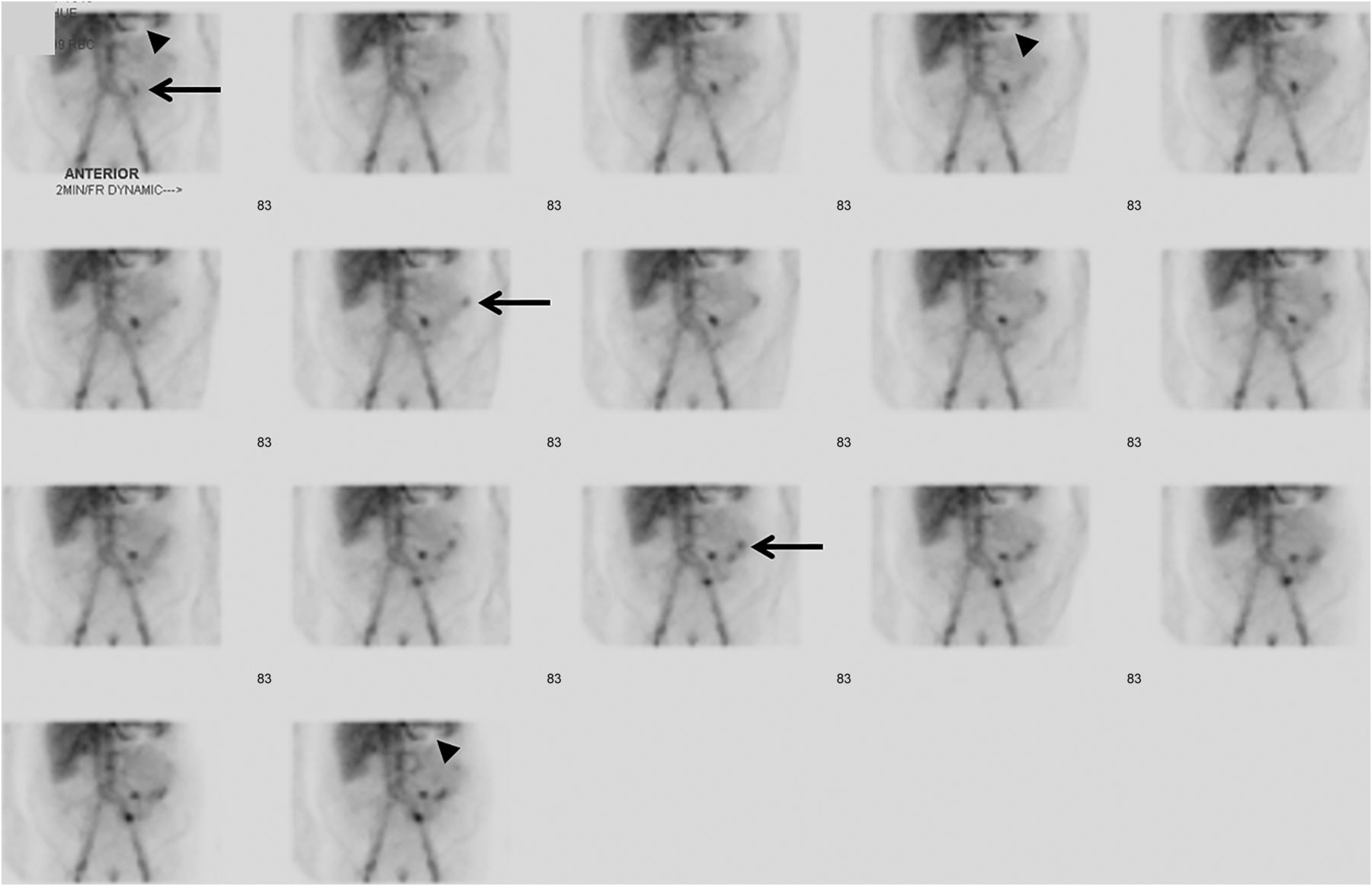
First-hour dynamic images (2 min/frame). Intraluminal tracer accumulation was immediately seen in proximal small-bowel loops (arrows), consistent with active bleeding. Visualization of continuous-flow LV assist device persists in this series (arrowheads).
DISCUSSION
Compared with pulsatile-flow LV assist devices, the continuous-flow devices are smaller and more durable. Despite the technologic advancement, there has been an increased incidence of gastrointestinal bleeding after placement of continuous-flow devices (3). The etiology of gastrointestinal bleeding appears to be multifactorial, with the two leading theories being acquired von Willebrand disease and low-pulsatile-pressure–induced arteriovenous malformation (3,4). Upper gastrointestinal bleeding is more common than lower gastrointestinal bleeding, with proximal small-bowel angiodysplasia as the bleeding source in 29% of patients with a continuous-flow device (3). 99mTc-tagged red blood cell scintigraphy is preferred to localize an active bleeding source and to guide the endoscopic procedure. On scintigraphy, the subtle artifact from the continuous-flow device is localized at the margin of the images, distinct from the prominent artifact described in the literature for the pulsatile-flow device (5).
CONCLUSION
Gastrointestinal bleeding is the most common complication after placement of a continuous-flow LV assist device. Recognition of the distinctive imaging presentation of such devices on 99mTc-red blood cell scintigraphy may raise awareness of this iatrogenic etiology and improve diagnostic confidence about gastrointestinal bleeding in nuclear medicine practice.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 29, 2019.
REFERENCES
- Received for publication September 5, 2018.
- Accepted for publication November 26, 2018.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.