


Abstract
We report a case of rare incidental initial detection of unsuspected arterial supply compromise to the right lower extremity on a bone scan obtained to rule out fracture in a patient with right hip pain after a fall. Follow-up CT angiogram confirmed near-complete occlusion of right lower extremity arteries for which patient underwent above-knee amputation.
Three-phase bone scintigraphy is a useful tool to assess arterial flow, relative soft-tissue perfusion, and variations in bone turnover. Systematic evaluation of all 3 phases is crucial to detect skeletal and unsuspected extraskeletal abnormalities.
CASE REPORT
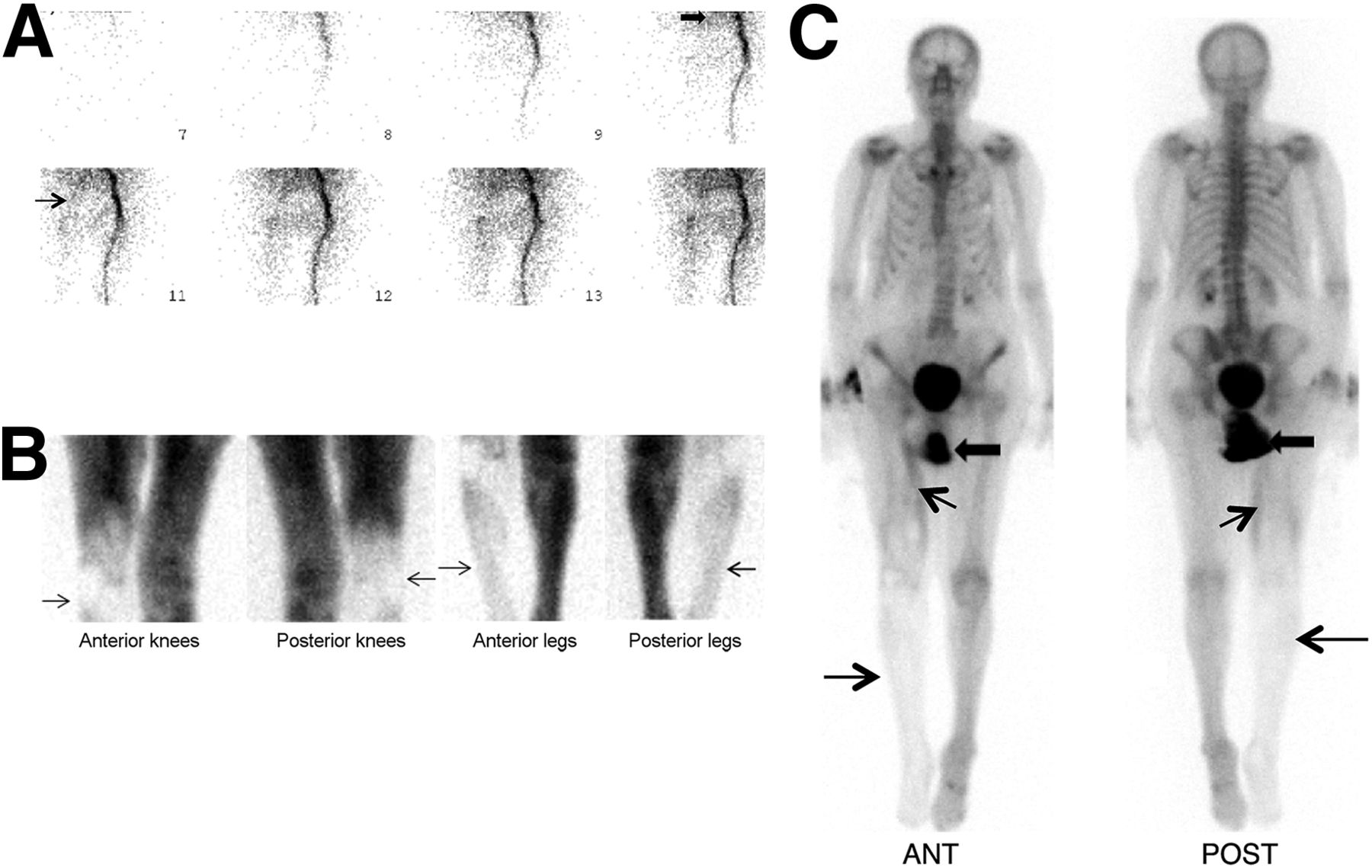
A 101-y-old patient with a history of atrial fibrillation presented to our hospital with right hip pain and difficulty walking after a fall. A plain CT scan of the bony pelvis and 3-phase 99mTc-methylene diphosphonate bone scintigraphy performed to rule out clinically suspected occult hip bone injury were negative for fracture. However, scintigraphy showed near-absent radiotracer activity within the right lower limb arteries on the flow phase (Fig. 1A), decreased soft-tissue uptake around the right knee and lower leg on the blood-pool phase (Fig. 1B), and decreased radiotracer uptake in the right femur, especially distally, and the lower leg bones on the delayed skeletal phase (Fig. 1C). Follow-up urgent CT angiogram on the same day demonstrated extensive thromboembolism of right lower limb arteries (Fig. 2). The right leg turned extremely painful and cold after a day. On physical examination, there was no palpable or audible right femoral, popliteal, and pedal flow. The patient had limited right knee flexion and limited sensation from the knee downward and could not move the right foot, and underwent right transfemoral above-knee amputation.

(A) Blood-flow images of 3-phase bone scintigraphy of thighs in anterior projection shows near-absent radiotracer uptake within right common iliac, external iliac (thick arrow), and proximal superficial femoral arteries (thin arrow). (B) Blood-pool images at knee/leg level in anterior and posterior projections show decreased soft-tissue uptake in right knee and leg (arrows). (C) Delayed whole-body bone scan in anterior and posterior projections show decreased radiotracer uptake in right femur, especially distally, and bones of right lower leg (thin transverse arrows). Increased linear uptake at medial right thigh (oblique arrows) possibly represents muscle injury. Note urinary activity in diaper (thick arrows).

CT angiogram of pelvis/lower limbs demonstrates extensive thromboembolism of right common iliac, external iliac, common femoral, popliteal, anterior, and posterior tibial arteries (white arrows).
DISCUSSION
Major factors determining radiotracer uptake in 3-phase bone scintigraphy are local blood flow, extraction efficiency, and osteoblastic activity. Impaired circulation, hydration level, renal function, and age also influence uptake (1,2). A bone scan is a useful adjunct to choose appropriate amputation level by aiding in distinguishing viable from nonviable tissue (3).
Assessing symmetry of radiotracer distribution is crucial. Venous or lymphatic obstruction and inflammation can cause asymmetrically increased tracer uptake. Unilateral paralysis can reduce ipsilateral uptake with increased contralateral activity from compensatory overuse. Decreased radiotracer activity can be seen in compromised arterial flow.
The functional status of the limbs could be improved with adequate collateral flow (4). However, because of minimal time available for collateral development in cases of acute thromboembolism, chances for above-knee amputation are doubled compared with chronic ischemia (5).
CONCLUSION
While interpreting bone scans, it is important not to confine our attention only to the detection of skeletal abnormalities. In our case, bone scan led to the initial diagnosis of critical ischemia of lower limb and apparent necrosis of thigh muscles, which led to further investigations, definitive diagnosis, and treatment. Any asymmetry in radiotracer uptake pattern in all phases on a 3-phase bone scan should not be overlooked.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 10, 2017.
REFERENCES
- Received for publication August 10, 2017.
- Accepted for publication August 28, 2017.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.