


Abstract
Many variables can influence the results of gastric emptying scintigraphy (GES). A lack of methodologic standardization may cause variability, limit comparisons, and decrease the credibility of the test. To address this, in 2009, the Society of Nuclear Medicine and Molecular Imaging (SNMMI) published a procedure guideline describing a standardized, validated GES protocol for adults. Laboratories must closely follow the consensus protocol to provide valid and standardized results and improve patient care. The Intersocietal Accreditation Commission (IAC) evaluates compliance with guidelines as part of the accreditation process. The rate of compliance with the GES guideline at a national level has not been assessed. The aim of this study was to quantify compliance with the standardized protocol in a large cohort of laboratories from different institutions and practice settings across the United States. Methods: The IAC Nuclear/PET database was used to extract GES protocols from all laboratories applying for accreditation from 2013 to 2015. Each protocol was assessed for compliance with the methods described in the SNMMI GES procedure guidelines. Fourteen binary variables were assessed: patient preparation (4 variables), meal content (5 variables), acquisition (2 variables), and processing (3 variables). Results: Protocols from 127 labs demonstrated that patient preparation was the category with which the laboratories were least compliant. Instructions for blood glucose monitoring and withholding of medications were problematic. Overall, 69.3% of protocols were not compliant with the content or preparation of the consensus meal: 47.3% used whole eggs instead of egg whites, and additional ingredients not recommended in the guidelines were also frequently used. Only 3.1% of laboratories were fully compliant with all 14 variables. Over half the laboratories were compliant with only 5 variables or less. Conclusion: Almost 8 y after the publication of the SNMMI GES guidelines, there is low protocol adherence among laboratories applying for IAC Nuclear/PET accreditation. This substantial degree of guideline noncompliance is concerning. The variability in GES protocols may have a significant effect on patient management, as results may be inaccurate. Consistent use of the standardized GES protocol permits interpretation of results in a standardized manner that allows interlaboratory comparisons and fosters acceptance of the test validity by referring clinicians.
Gastric-emptying scintigraphy (GES) is considered the reference standard for measuring gastric motility in patients with symptoms suggesting altered gastric emptying. Many variables can influence the results of the test, such as patient factors (e.g., test preparation or blood glucose level), meal composition and amount, acquisition parameters (e.g., camera position or duration of measurement), and method of analysis (1,2). A lack of methodologic standardization may cause variability in the results and in the reporting of GES, limit comparisons between institutions, and decrease confidence in and the credibility of the test (1,3). To address this issue, members of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine and Molecular Imaging (SNMMI) published a consensus statement in 2008 (1). The key points of these recommendations were published by SNMMI in 2009 as Procedure Guideline for Adult Solid-Meal Gastric-Emptying Study 3.0, which describes a standardized, validated GES protocol to guide nuclear medicine practitioners in performing and interpreting GES studies in a reproducible manner (4). Laboratories must closely follow the consensus protocol to provide valid and standardized results and improve patient care.
Accreditation is often viewed as a gatekeeper of quality. The Intersocietal Accreditation Commission (IAC) determines quality by evaluating laboratory staff qualifications, imaging protocols, image quality, and reporting. A laboratory must be in compliance with the IAC Standards and Guidelines for Nuclear/PET Accreditation to be accredited (5). Specifically, the standards require that facility-written protocols and procedure performance must follow accepted practices such as those published in professional society guidelines.
The rate of compliance with the GES guideline at a national level has not been assessed. The aim of this study was to quantify compliance with the standardized protocol in a large cohort of laboratories from different institutions and practice settings across the United States.
MATERIALS AND METHODS
The IAC database, consisting of facility demographic, staff qualification, protocol, case study, and report information, was used to extract GES protocols from all laboratories applying for general nuclear medicine accreditation from January 1, 2013, to December 31, 2015. Approval from an Institutional Review Board was not required as no patient data or private or identifiable facility information was collected, and the results were reported in aggregate.
Nine demographic variables were recorded, including facility type (hospital vs. nonhospital practice setting), accreditation cycle (first time vs. reaccreditation), accreditation decision (accredited vs. delayed), general nuclear medicine annual study volume (excluding nuclear cardiology and PET), number of physicians and technologists, American Board of Nuclear Medicine (ABNM)–certified medical director, any ABNM-certified physicians on staff, and number of γ-cameras.
We assessed each GES protocol for compliance with the methods described in the SNMMI GES procedure guideline (4). Fourteen binary variables considered the most important for the performance of GES were selected and grouped into 4 categories: patient preparation (4 variables), meal content (5 variables), image acquisition (2 variables), and processing (3 variables) (Table 1). Meal content was further categorized into 8 subgroups depending on the ingredients used (Table 2). The total number of compliant variables per laboratory was calculated. Laboratories with an overall score of 14 were compliant with all designated variables in the standardized protocol. Conversely, laboratories with a score of 0 were compliant with none.
Standard Protocol Variables
Meal Content Subgroups
The 14 compliance variables and the demographic variables were compared to ascertain any trends or associations. We also analyzed for correlations between the total number of compliant variables and the demographic variables.
We analyzed the data using SPSS for Windows (version 22.0; IBM). The data were cleaned and examined for outliers, normality of distribution, and correlations. The frequency and percentage compliance was reported for the 14 variables, meal subgroup, and categoric demographic variables. Mean, median, and range were reported for the continuous demographic variables, which were also categorized by quartile. The compliance and demographic variables were compared using χ2 statistics for categoric variables and ANOVA for continuous measures. Pearson correlation was used to determine trends related to the number of correct variables. For all tests, a P value of less than 0.05 was considered significant.
RESULTS
In total, 183 laboratories applied for general nuclear medicine accreditation from 2013 to 2015. Of those, 171 applied for gastrointestinal imaging accreditation, with 127 laboratories submitting GES protocols. The remaining 44 laboratories did not provide GES protocols because they either do not perform GES or submitted other types of gastrointestinal imaging protocols (e.g., hepatobiliary imaging or liver scanning) for evaluation.
Demographic Measures
Frequency distributions for the demographic variables are listed in Table 3. Most laboratories were hospital-based (63.0%). Laboratories performed a mean of 1,709.4 ± 1,805.2 (median, 1,201) general nuclear medicine studies annually. Almost all the laboratories (96.1%) had previously completed the accreditation process and had applied for reaccreditation. However, general nuclear medicine accreditation was delayed for a majority of laboratories (59.8%) pending correction of issues.
Laboratory Demographic Data (n = 127)
Compliance with GES Guideline Variables
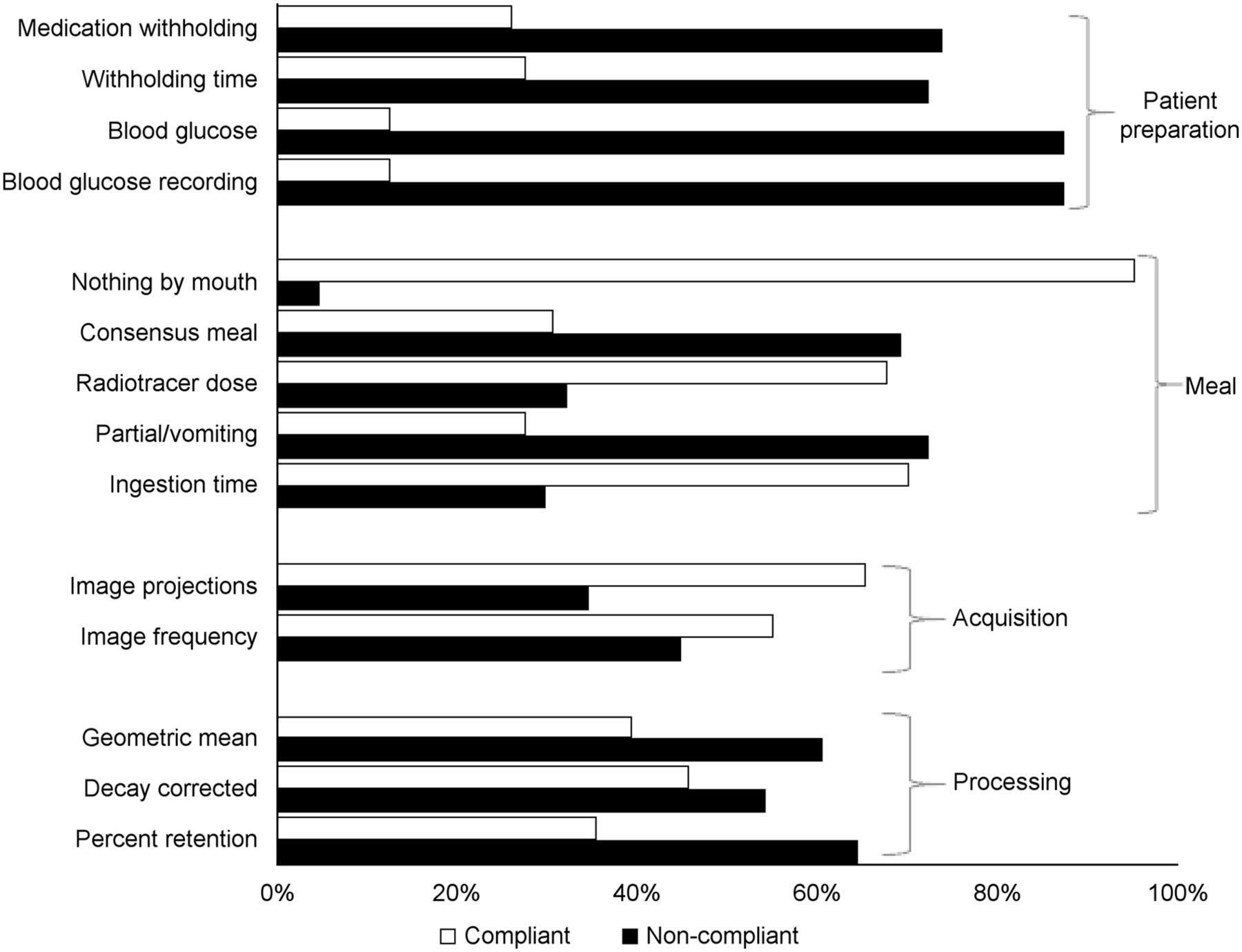
Laboratory compliance with the protocol variables grouped by category is shown in Figure 1. These ranged from a high of 95.3% of laboratories compliant with the instruction to take nothing by mouth for at least 4 h before the study to a low of 12.6% laboratories compliant with blood glucose measurement and reporting. Taken overall, the variables that were least followed were related to patient preparation. Other problematic variables in that section were instructions regarding the withholding of medications and the length of time for which medications were withheld, 74.0% and 72.4%, respectively. For most protocol variables (9/14), more than half the laboratories were noncompliant (Fig. 1).
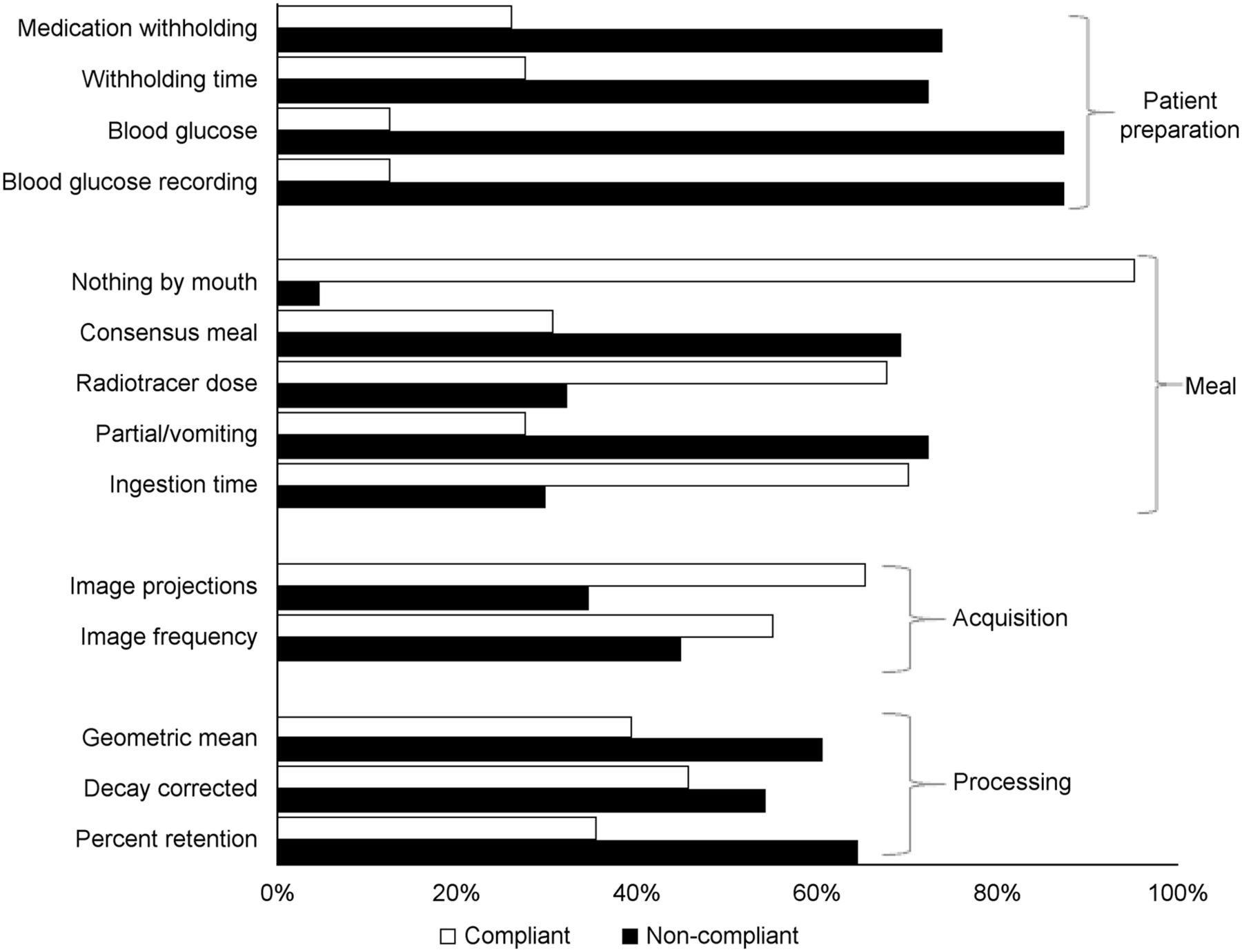
Compliance with 14 individual protocol variables. Results demonstrate that laboratories did not adhere to GES guidelines for most variables (9/14) (n = 127).
Overall, 69.3% of laboratory protocols were not complaint regarding the consensus meal. Detailed evaluation of the composition of the meals showed that fewer than a third (30.7%) of laboratories used the exact meal content—egg whites, white toast, jelly, and water—recommended in the guidelines (Table 4). Variations of the egg white consensus meal, with partial or additional ingredients, were used in 4.8% of laboratories. A large number of laboratories (47.3%) used whole eggs instead of egg whites with either partial or additional ingredients. Of this group, whole eggs were the sole component of the meal for 16.3% of laboratories. Additional ingredients not recommended in the guidelines but part of the whole-egg meal were used in 14.2% of laboratories and included juice, milk, butter or margarine, lettuce, tomato, and peaches.
Meal Component Variation (n = 127)
Oatmeal alone or combined with additional ingredients was used in 11.8% of laboratories as the standard meal for all patients. Egg allergy was not given as a reason to substitute oatmeal for eggs. Highly unusual GES meals were used by 4.7% of laboratories. These included a honey bun, corn flakes and milk, a peanut butter sandwich, an egg salad sandwich, an egg burrito, or a McDonald’s Egg McMuffin. In addition, we found a variety of unusual meal preparation methods. For instance, several laboratories instructed the patient to bring scrambled eggs from home and added the tracer to the already cooked eggs. Numerous laboratories injected the 99mTc-sulfur colloid (99mTc-SC) directly into the egg yolk.
Overall Variable Compliance
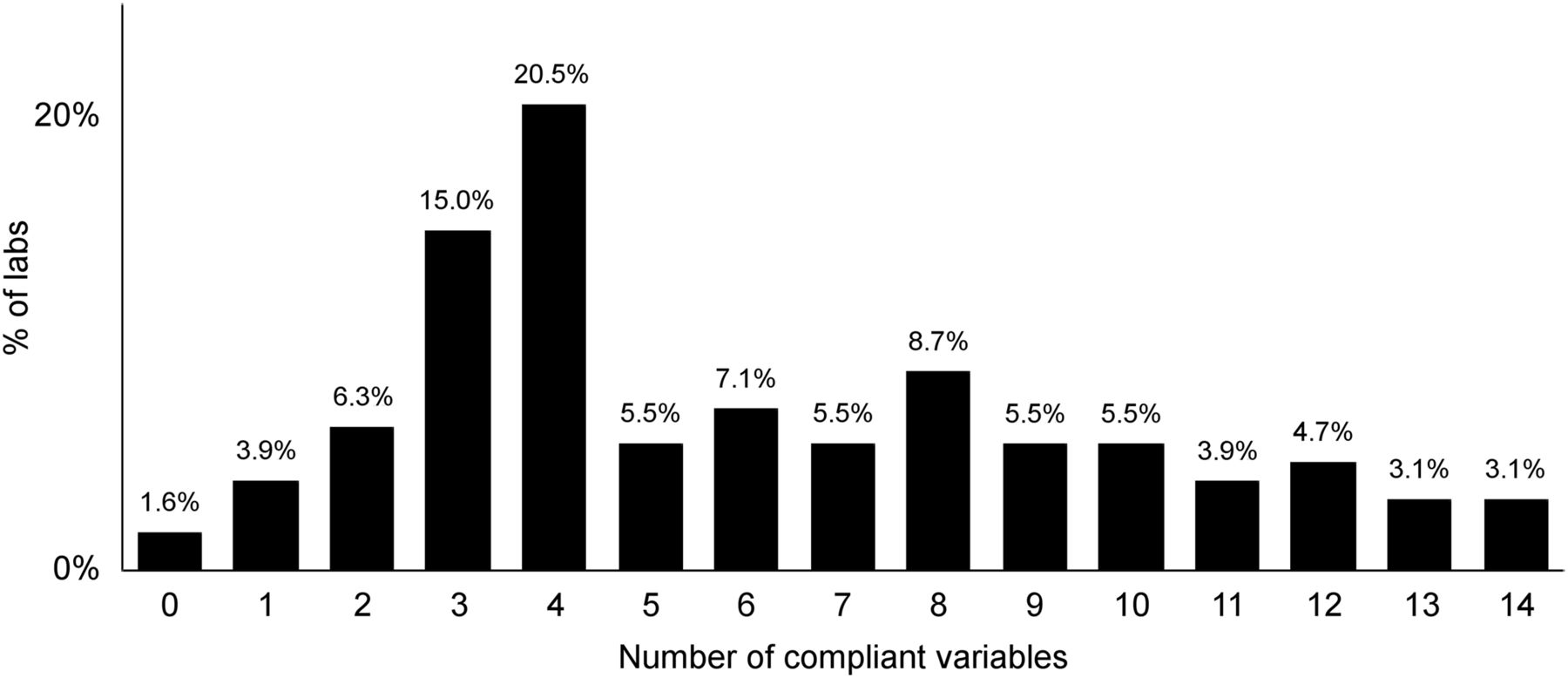
Only 3.1% of laboratories were fully compliant with all 14 variables (Fig. 2), and conversely, 1.6% were not compliant with any of the variables. Over half the laboratories were compliant with only 5 variables or fewer.

Number of variables compliant with guidelines per laboratory. Very few laboratories were compliant with all 14 variables.
Compliance Comparisons with Demographic Variables
We analyzed for correlations between the compliance variables and the laboratory demographic variables to search for trends. However, few significant differences were found. Regarding compliance with the consensus meal, laboratories were more likely to comply when there were ABNM-certified physicians on staff (P = 0.005). However, there was no significant difference based on whether the medical director was ABNM-certified (P = 0.265). Significant positive correlations were found between meal compliance and number of technologists (r = 0.231, P = 0.009) and between meal compliance and annual volume of general nuclear medicine studies (r = 0.243, P = 0.029). Meals were also more likely to be compliant with the consensus meal in larger laboratories with a greater number of technologists and a higher annual volume of studies.
DISCUSSION
Evidence-based procedure guidelines provide concise instructions on how to perform a diagnostic study, thus ensuring protocol standardization (6). The principal aim of practice guidelines is to improve the quality of patient care and outcomes (7). Studies have shown that practice guidelines can improve the process of care and reduce variation in practice (8). Guidelines improve consistency by making it more likely that patients receive the same care regardless of where the test is performed and who performs it.
In 2009, SNMMI published Procedure Guideline for Adult Solid-Meal Gastric-Emptying Study 3.0 with the aim of standardizing the performance of GES protocols and avoiding unreliable test results, nonvalid clinical interpretations, and problematic variations between nuclear medicine sites (4). This guideline reflected the consensus of several professional societies (1). Data obtained from laboratories applying for IAC accreditation show that almost 8 y after the publication of the guideline, there is a low rate of compliance with them in our study group of 127 laboratories. A small number of laboratory protocols (3.1%) were fully compliant with the guideline protocol components.
GES Variability
Patient Preparation
When a diagnostic protocol differs from the standard methodology, a variety of technical and physiologic sources of error and variation in the test results may be introduced. Our results demonstrated that 74.0% of laboratory protocols did not include instructions for withholding medications. In general, unless determining a treatment response is the purpose of the GES study, medications that alter gastric emptying should be withheld for an appropriate period, often 48–72 h, depending on the specific half-life (4). Although most medical and technical staff are aware of the potential confounding effects of prokinetic drugs, such as the effect of metoclopramide on the measurement of gastric emptying, less consideration is given to drugs not specifically prescribed for their gastrointestinal action, such as opiates, erythromycin, atropine, theophylline, and benzodiazepines (Appendix A). It is particularly important for the protocol to list not only the classes of medication that may interfere with the test but also the various brand and generic names and the length of withholding. Nuclear medicine technologists are usually responsible for obtaining the patient’s medical history, including medications, and screening for contraindications or other factors that may affect the results of the test. Technologists are unlikely to be aware of the entire list of medications that can alter the rate of gastric emptying; therefore, a comprehensive list in the protocol is useful for easy reference. Improved education of all staff will lead to improved compliance and generate more accurate and reproducible results.
Most of the protocols (87.4%) in our study did not contain an instruction to measure the patient’s blood glucose level immediately before testing (9). Ideally, the blood glucose level should be less than 200 mg/dL. Hyperglycemia is an important cause of delayed gastric emptying. The blood glucose level should be recorded and included in the final report so that the effects of elevated blood glucose may be taken into consideration in the final interpretation.
Meal Composition
This study demonstrated that the composition and preparation of the GES test meal is a major source of variability. Meal composition (volume, caloric content, and fat content) significantly affects the rate of gastric emptying. Solids, indigestible foods, and fats empty more slowly, whereas liquids, highly digestible foods, proteins, and carbohydrates empty more rapidly (10–13). Divergence of the test meal from the standard precludes valid comparisons to published normal values and, thus, may factitiously alter the interpretation of normal versus delayed emptying (1).
The standardized meal described in the GES guideline consists of 18.5–37 mSv (0.5–1.0 mCi) of 99mTc-SC scrambled with 120 g of liquid egg white (Egg Beaters [Conagra Brands] or generic) plus 2 slices of white toast, 30 g of strawberry jelly, and 120 mL of water (4). In the current study, laboratory test meals with additional ingredients such as juice or butter, oatmeal, or another nonstandard composition would not be expected to have the same emptying rate or reference values as the consensus meal. It cannot be emphasized more strongly that an alternative meal has no validity for interpreting GES results unless specific reference databases for that particular meal have been developed by the individual laboratories.
Meal Preparation
The liquid egg whites must be cooked together with the 99mTc-SC, thereby forming a bond with the protein component as it becomes denatured during heating; this property is exploited to trace true solid gastric emptying. Firm binding between the egg whites and the 99mTc-SC produces a stable solid that keeps the labeled component from being absorbed or binding to the mucous membranes of either the stomach or small intestine. If the tracer separates from the protein, the test result will vary because the meal becomes a part-solid, part-liquid mixture. A common error in this study was that some laboratories simply added the tracer to an already prepared solid food (e.g., honey bun, peanut butter sandwich, or previously cooked scrambled eggs). However, these methods have no binding property, and the tracer does not remain associated with the solid particles (14,15).
Another common protocol variant found in this study was the use of whole eggs rather than the recommended liquid egg product (14). Several laboratory protocols included instructions to inject the tracer directly into the egg yolk. 99mTc-SC binds to the egg white albumen, and there is no evidence that egg yolk, which is primarily fat, binds 99mTc-SC (14). Egg white substitute is preferred over scrambled fresh, whole eggs because the substitute has a higher binding percentage and is less likely to disintegrate in gastric fluid. The labeling efficiency of egg substitute is approximately 85%. Approximately 80% of 99mTc-SC remains bound to the egg substitute at 3 h. An additional source of error is the increased fat content of the meal from the egg yolk, which slows gastric emptying.
Acquisition
The frequency and duration of image acquisition were not according to guideline standards in 45.0% of laboratories. The consensus protocol recommends imaging until up to 4 h for improved sensitivity in detecting delayed gastric emptying. The literature has suggested that retention of more than 10% of the meal at 4 h is abnormal and is the best discriminator between normal and abnormal results (4,16,17). Recently published articles suggest that a shortened protocol may be a satisfactory compromise (16), but consensus has not yet been established in the literature. This issue is complex because of differences in gastric fundal and antral actions (18).
Processing
In this study, 54% of laboratories performed their assessment using half-time of emptying, despite guidelines and literature supporting the use of percentage retention of the meal in the stomach. Interpretation using half-time is potentially less accurate than percentage retention, especially for patients with delayed emptying, for which extrapolation is needed to calculate half-time if half the meal does not leave the stomach during the test. Furthermore, it has long been established that solid food does not empty from the stomach in a linear fashion but has distinct phases corresponding to the roles played by the fundus and antrum (19). The ideal methodology, such as percentage retention, takes into account the entire time–activity curve (nonexponential for solids).
Guideline Implementation
It is troubling that nearly 8 y after publication of the GES guidelines, there is a low rate of compliance. In translational research, there is a well-known, documented gap in widespread implementation of published guidelines (20–22). It usually takes an average of 9.3 y for guidelines to become customary practice (23), as is unfortunately supported by the results of this study. Our finding of poor adherence to guidelines agrees with a 2011 study on 134 laboratories in the Department of Veterans Affairs approximately 2 y after the publication of the consensus recommendations (24). Only 12% of Veterans Administration laboratories strictly followed the standardized protocol, compared with 8.5% for the same criteria in our population.
What are the possible barriers to compliance with the published consensus recommendations? First, facility personnel may simply be unaware of the existence of the published guideline (25). If this is true, it points to the need for better and more effective dissemination. For example, the results of this study showed that facilities were more likely to follow the consensus meal when ABNM-certified physicians are on staff. One reason is that noncertified physicians may not consult the SNMMI guidelines for protocols, and the American College of Radiology does not have a detailed, comprehensive guideline for this procedure. Even if personnel are aware of the published guidelines, the sheer volume of published material makes it impossible to read and remember the details of many articles and guidelines and, thus, apply them properly.
Another barrier may be interpreting-physician preference or longstanding use of a specific test meal or reporting method. Imaging physicians and technologists may be anxious about and resistant to changing their habitual practice. For instance, there may be concern that the longer protocol may tie up a camera and make scheduling more difficult and perhaps less efficient. Lack of staff time and lack of resources to make changes may be a factor. Simple inertia, lack of motivation, or refusal has been shown to play a small role (26).
A final impediment may be the controversy in the recent literature suggesting that assessment of liquid emptying may be more important than previously realized, as well as controversy about the most expedient duration of imaging for GES (16,17). These unresolved issues may cause practitioners to question whether a protocol change is warranted (27). Physicians may not follow guidelines if they think that they are based on poor evidence (28). If the medical and technical staff do not believe that following the guideline recommendations makes a difference in the test result, they are hardly inclined to do so (29). In addition, if guidelines are convoluted or complex, facilities may be less likely to comply. These reasons may have been a factor in the current study, in which most of the labs had been through the accreditation process more than once but were still not completely following the consensus recommendations.
The findings of our study highlight the need for continued educational efforts to disseminate the published standardized guideline protocols. Guideline implementation is complex. Therefore, the need for strategies to facilitate implementation and continually monitor for compliance is essential. A review of literature on changing physician behavior demonstrates that active forms of continuing medical education (as opposed to passive forms) with multiple interventions are the most efficient for promoting guideline implementation into customary practice (23,30,31). This applies equally to technologists. Examples of active forms include academic detailing (presentations by trained individuals at the physician’s office), educational outreach programs tailored specifically to the needs of a specific clinic, or small-group workshops. Passive forms such as printed educational brochures and traditional conferences are effective at raising awareness but less effective at bringing about change (32).
Limitations
This study was a retrospective evaluation of accreditation applications submitted to the IAC. The IAC database was designed to manage the accreditation process but not specifically to perform observational research. It is possible that laboratories may be following the guidelines but not documenting their practice in the protocol. For the purpose of this research, we followed the adage “not documented, not done.” Consequently, if laboratories did not explicitly state their protocol, they were considered noncompliant. An additional limitation is that adherence to guidelines was chosen as a surrogate for quality because measuring direct patient outcomes in diagnostic medicine is complicated. Finally, there are no data to compare with non–IAC-accredited laboratories. Thus, the results are applicable only to IAC-accredited laboratories.
CONCLUSION
Almost 8 y after the publication of the SNMMI GES guidelines, there is low adherence with them among laboratories applying for IAC Nuclear/PET accreditation. This substantial degree of noncompliance is concerning. The variability in GES protocols may have a significant effect on patient management, as results may be inaccurate. Consistent use of the standardized GES protocol permits interpretation of results in a standardized manner, allowing interlaboratory comparisons and fostering acceptance of the test validity by referring clinicians. The current low level of protocol adherence indicates a continued gap between guideline publication and implementation and points to a need for further dissemination of the consensus protocol and strategic education efforts.
DISCLOSURE
Mary B. Farrell and Maria Costello are employees of the IAC. Lorraine M. Fig and Leonie L. Gordon are members of the IAC Board of Directors. No other potential conflict of interest relevant to this article was reported.
Medications That Alter Gastric Emptying*
Footnotes
Published online Feb. 2, 2017.
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than March 2020. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication October 11, 2016.
- Accepted for publication November 14, 2016.





{kind=link}
{kind=link}