


Abstract
Common variable immunodeficiency is characterized by low levels of serum immunoglobulins and antibodies, recurrent infections, and a predisposition to malignancy. Here, we present the 18F-FDG PET/CT findings of a 7-y-old boy with common variable immunodeficiency and Hodgkin lymphoma.
Common variable immunodeficiency is one of the most common primary immune deficiencies, affecting approximately 1 in 10,000–50,000 people. Recurrent infections and granulomatous diseases are main features of this disorder. The risk of malignancy, especially gastric carcinoma and lymphoma, also increases in patients with common variable immunodeficiency (1). Here, we report the 18F-FDG PET/CT findings of a 7-y-old boy with common variable immunodeficiency and Hodgkin lymphoma.
CASE REPORT
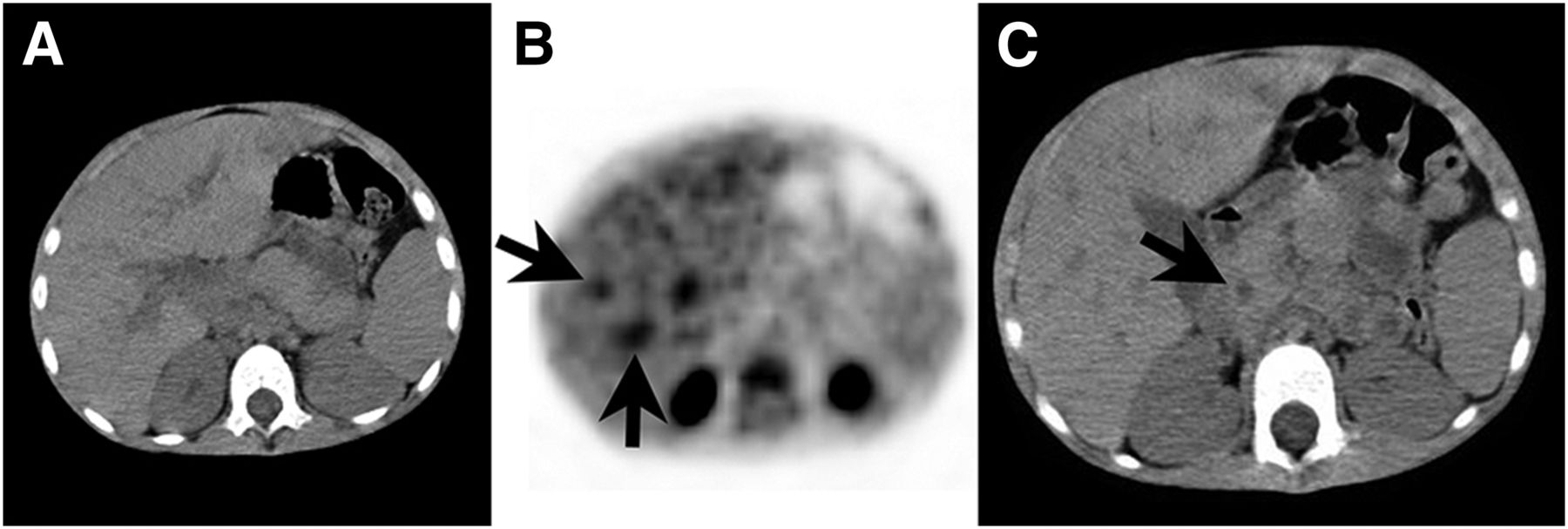
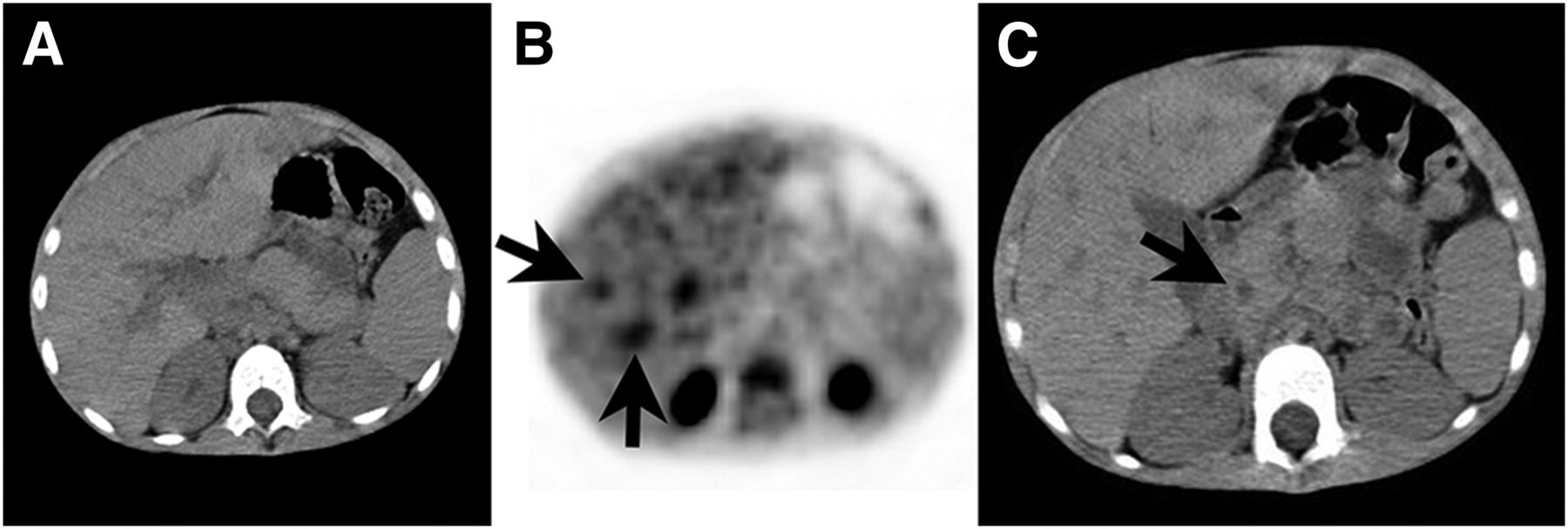
Hodgkin lymphoma was detected in a 7-y-old boy with common variable immunodeficiency. The patient had experienced recurrent lower respiratory tract infections, growth retardation, chronic diarrhea, and hypogammaglobulinemia since he was 4 y old. PET/CT for staging of Hodgkin lymphoma demonstrated 18F-FDG–avid supradiaphragmatic lymphadenopathies (Fig. 1). Abdominal lymphadenopathies seen on the CT images of the PET/CT examination did not show distinctive 18F-FDG uptake (Fig. 2). Widespread bronchiectasis, accompanying infiltration, and peribronchovascular thickening with intense 18F-FDG uptake in the lung fields were demonstrated bilaterally but predominantly in the left lung (Fig. 1). Dilatation of the ductus choledochus and 18F-FDG accumulation in the biliary tract, suggesting cholangitis, were also seen on the PET/CT images (Fig. 3). MR cholangiopancreatography revealed intra- and extrahepatic duct dilatation and lymph nodes in the hepatic hilus. High alanine aminotransferase and aspartate aminotransferase levels were noted. It was thought that an obstructive suppurative cholangitis had resulted from biliary obstruction provoked by enlarged lymph nodes. The patient received 6 cycles of doxorubicin, vinblastine, and dacarbazine and 3,000 cGy of total mediastinal radiotherapy. Bleomycin was not administered. Unfortunately, the patient died of sepsis 15 mo after the initial diagnosis. Informed consent for publication of the case was obtained from the patient’s parents.
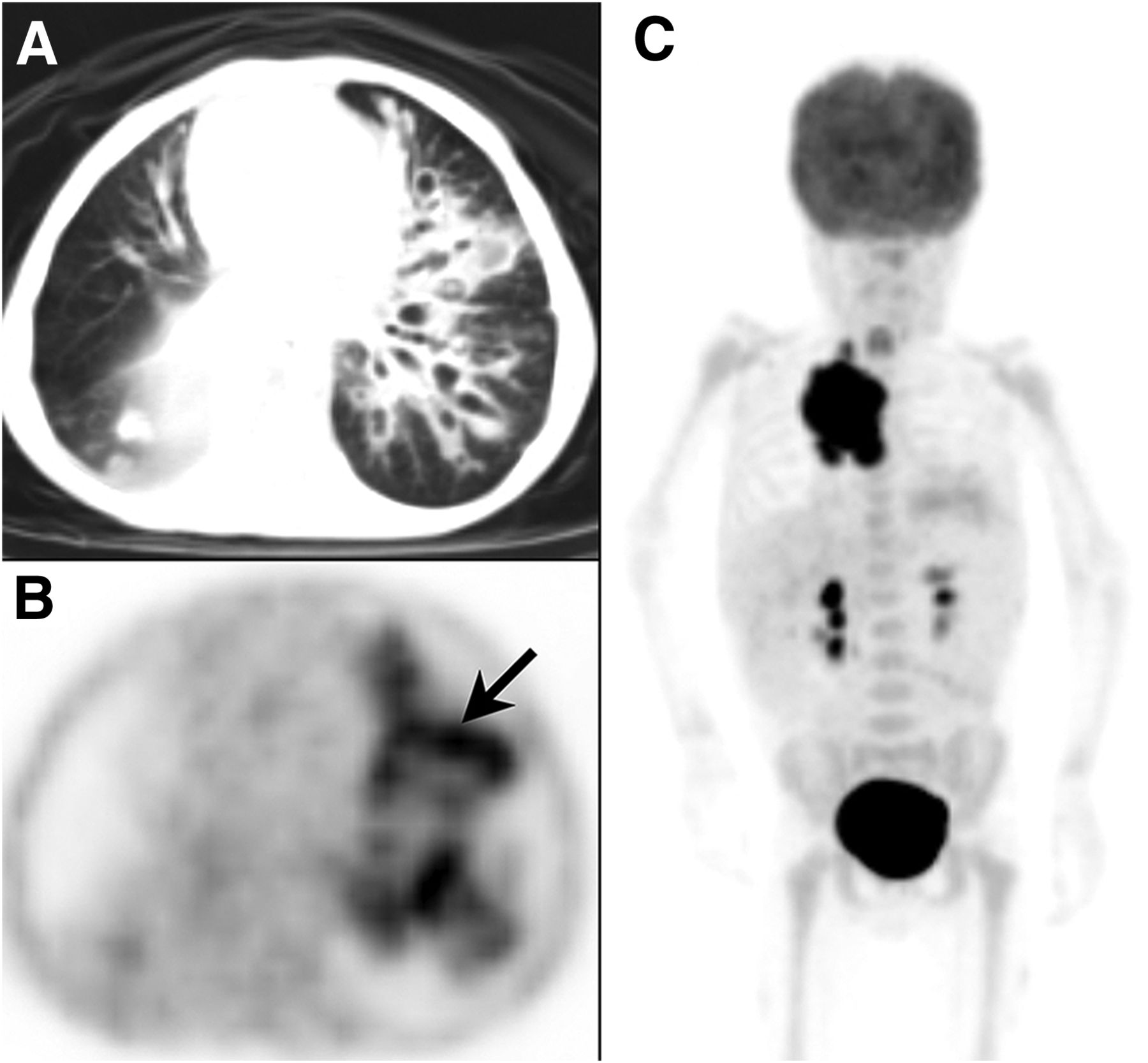
PET/CT demonstrated widespread bronchiectasis, accompanying infiltration, and peribronchovascular thickening in left lung (A and B, arrow) and 18F-FDG–avid supradiaphragmatic lymph nodes (C).

Abdominal lymph nodes were seen on the CT images (arrows), but they showed no distinctive uptake on the PET images.
18F-FDG PET/CT demonstrated 18F-FDG accumulation in biliary tract (A and B, arrows) and dilatation of ductus choledochus (C, arrow).
DISCUSSION
In our patient, infectious foci in the lung and biliary tract were detected on the 18F-FDG PET/CT scan. Recognition of coincidental infections is important in cancer patients under immunosuppression because they have an increased risk of sepsis secondary to the toxic effect of chemotherapy. 18F-FDG PET/CT may therefore be valuable for monitoring patients with common variable immunodeficiency. However, patients with this disorder are hypersensitive to x-irradiation and radiomimetic drugs such as bleomycin, and increased radiosensitivity is one of the risk factors for malignancy. It has been shown that lymphocytes derived from patients with common variable immunodeficiency are significantly more radiosensitive than those from healthy individuals and that chromosomal aberrations (chromatid breaks and gaps) in such patients increase after x-ray exposure (2). Significant radiation exposure occurs from PET/CT, even with a child-adapted low-dose regimen. In one study, the average radiation dose from 18F-FDG PET/CT was estimated to be 12.15 mSv: 5.89 mSv from 18F-FDG PET and 6.26 mSv from CT (3). 18F-FDG PET/MRI provides a lower radiation exposure, and the sensitivity and specificity of 18F-FDG PET/MR have been shown to be similar to those of 18F-FDG PET/CT for the staging of lymphoma patients (4).
CONCLUSION
18F-FDG PET/CT may be useful in monitoring malignancies and detecting infectious foci in pediatric patients. However, because of the risk of hypersensitivity to x-irradiation, PET/MR may be a better choice for staging lymphomas in patients with primary immune deficiencies.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 30, 2016.
- Received for publication March 16, 2016.
- Accepted for publication June 1, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.