


Article Figures & Data
Figures
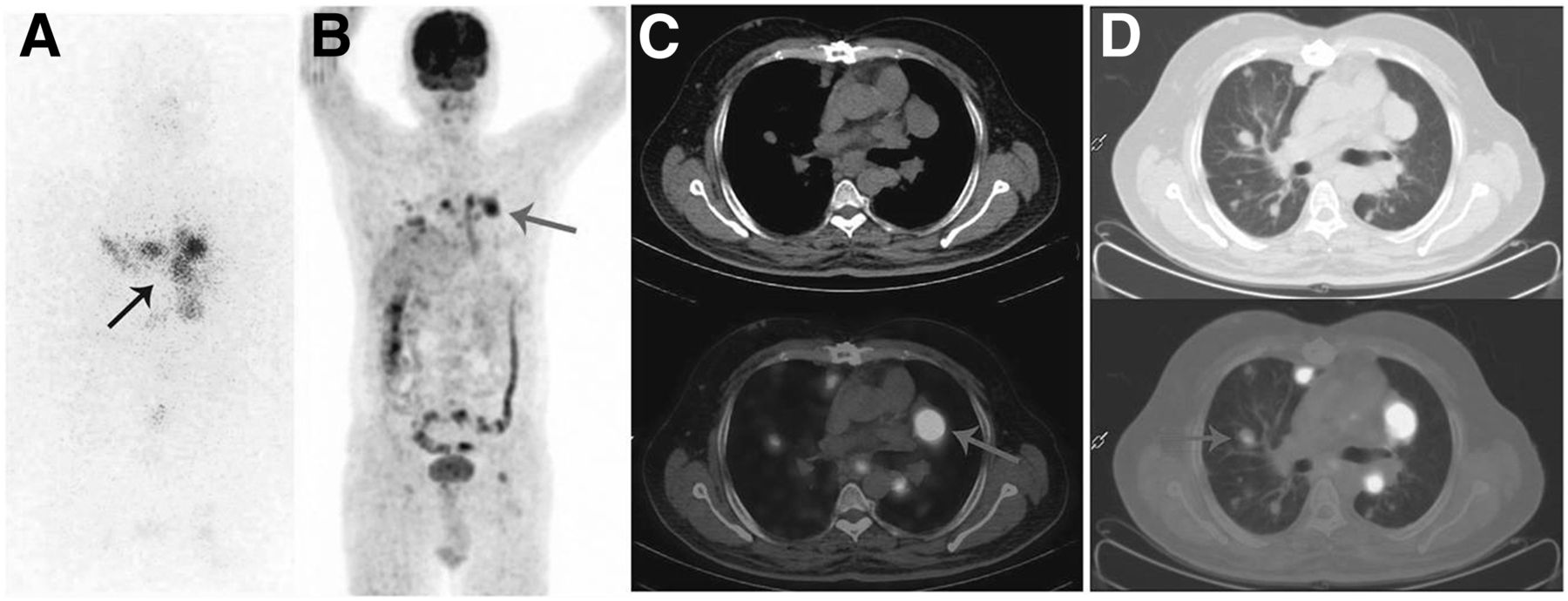
- FIGURE 1.
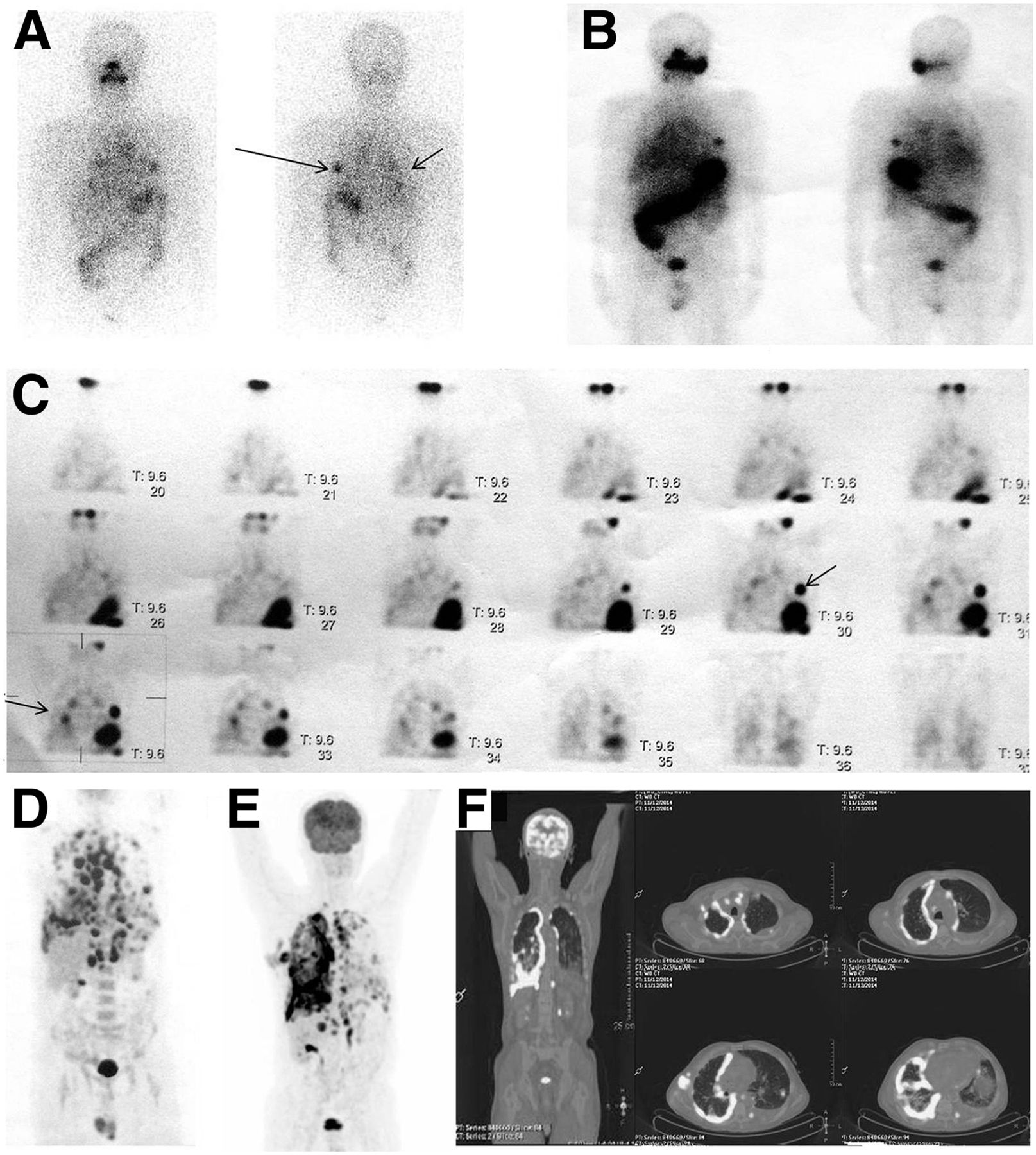
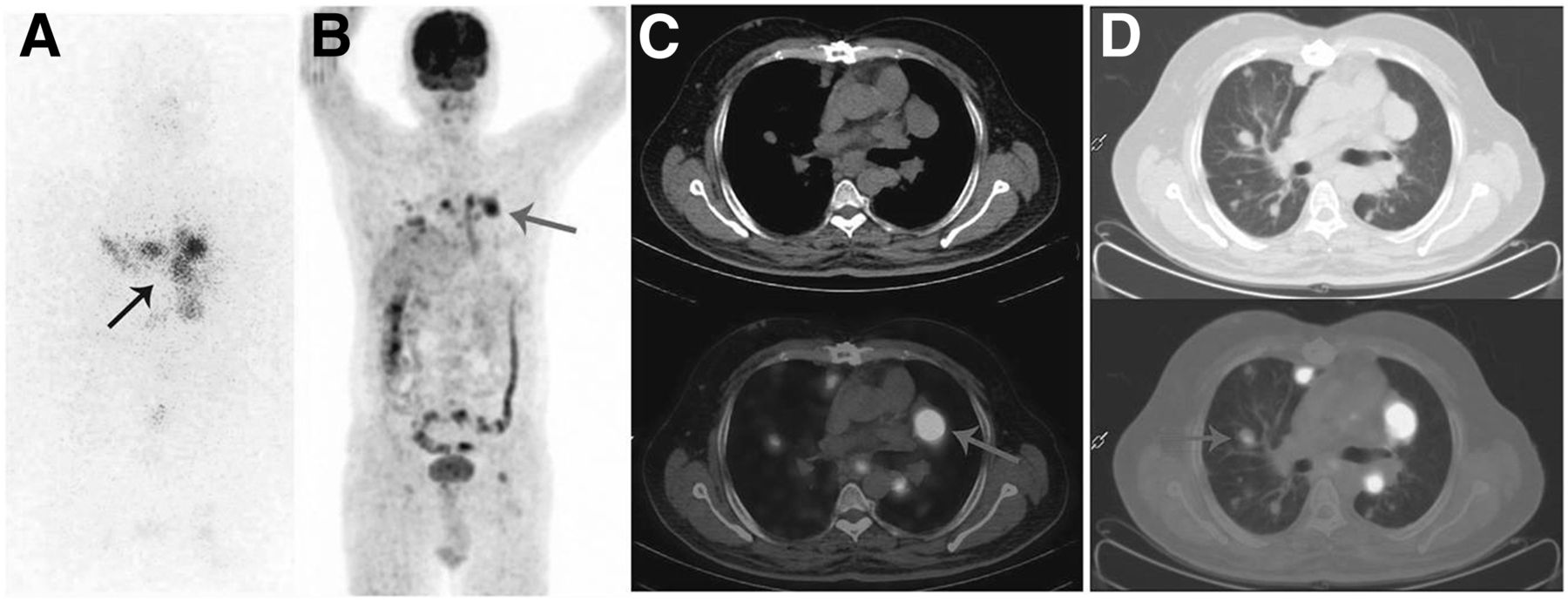
(A) Diagnostic 131I scan showed some 131I-avid foci in both lungs, though lesions were much more numerous on 18F-FDG PET/CT scan (D), which showed multiple metabolically active foci in both lungs and pleurae, as well as mediastinal foci. Lesions on posttreatment 131I planar scan (B) and SPECT scan (C) were similar to those on diagnostic 131I scan. Comparative 18F-FDG PET/CT scan 1 y previously (D) and present scan (E and F) show progressive disease. Serum thyroglobulin level was more than 300 ng/mL on both occasions. Therapy with tyrosine kinase inhibitor (sorafenib) was started in view of progressive symptomatic disease on 18F-FDG PET/CT. Arrows indicate tracer uptake or lack thereof. A color version of F is available as a supplemental file at http://tech.snmjournals.org.
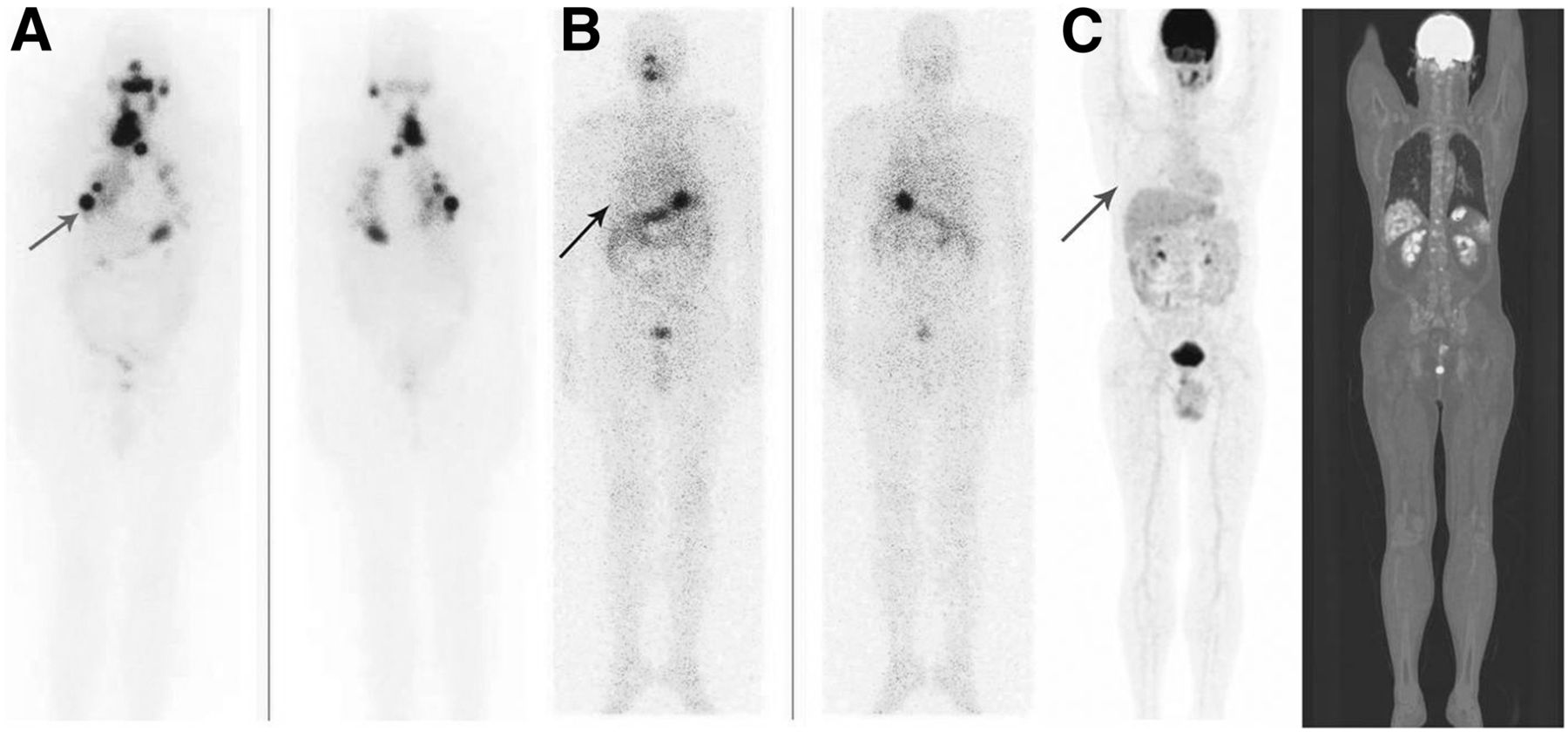
- FIGURE 2.
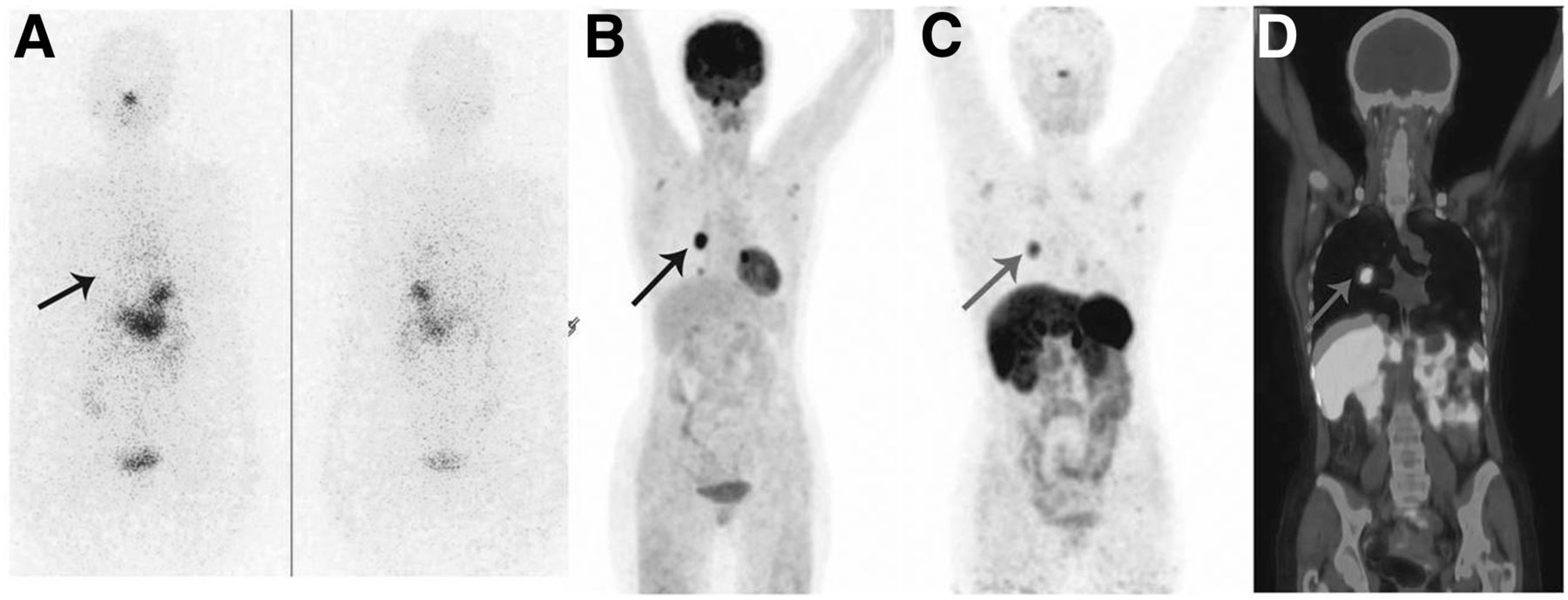
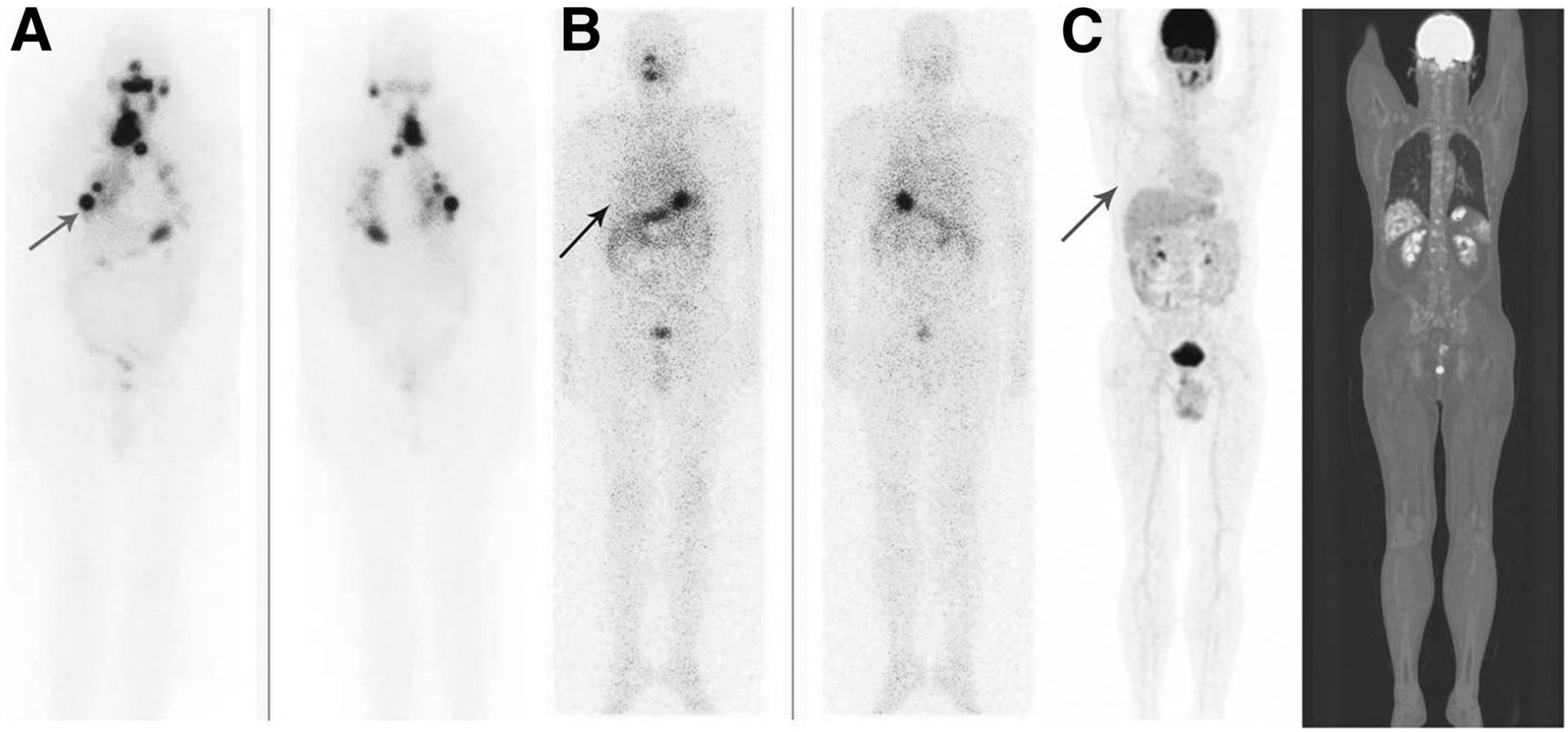
Whole-body 131I diagnostic scintigraphy scan (A), 18F-FDG PET/CT maximum-intensity-projection scan (B), 68Ga-DOTATATE maximum-intensity-projection scan (C), and coronal fused image (D) in known case of follicular variant of PTC. No abnormal tracer activity is seen in thoracic region on 131I scan. 18F-FDG–avid lesion and somatostatin receptor–avid lesion (on 68Ga-DOTATATE scan) are seen in thoracic region and axillary nodes. Arrows indicate tracer uptake or lack thereof. A color version of this figure is available as a supplemental file at http://tech.snmjournals.org.
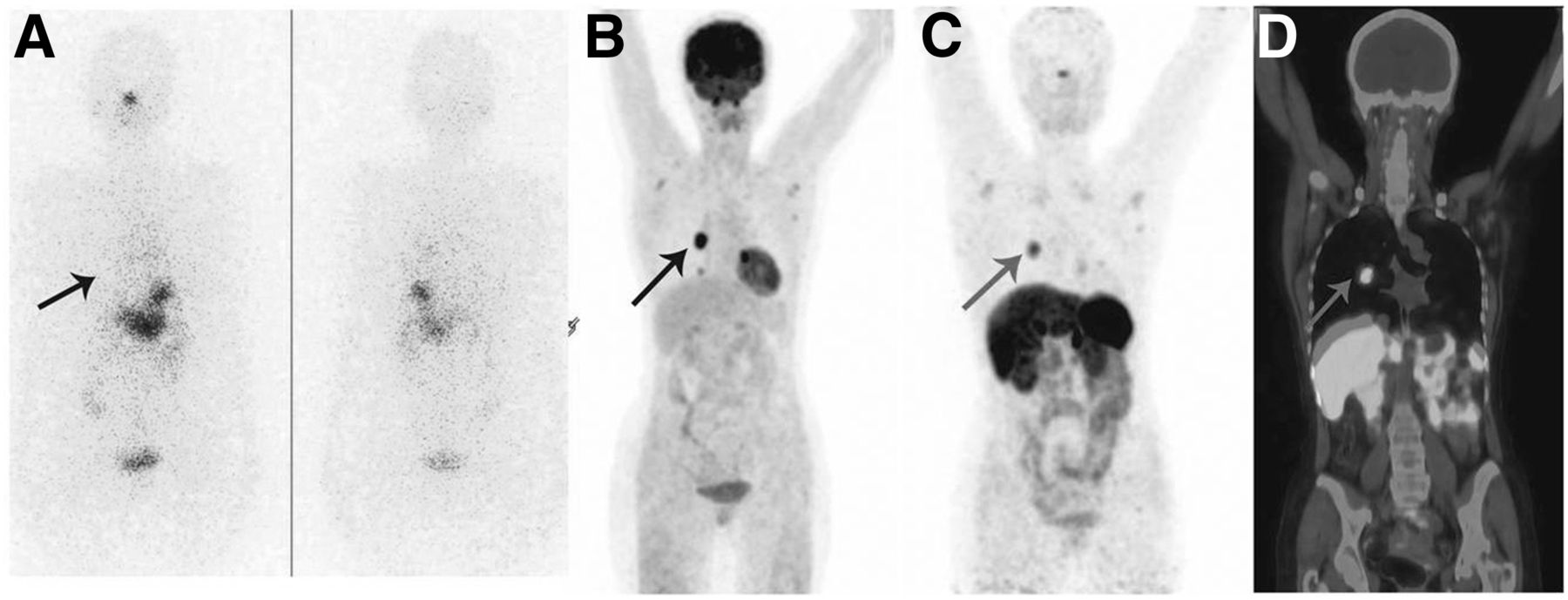
- FIGURE 3.
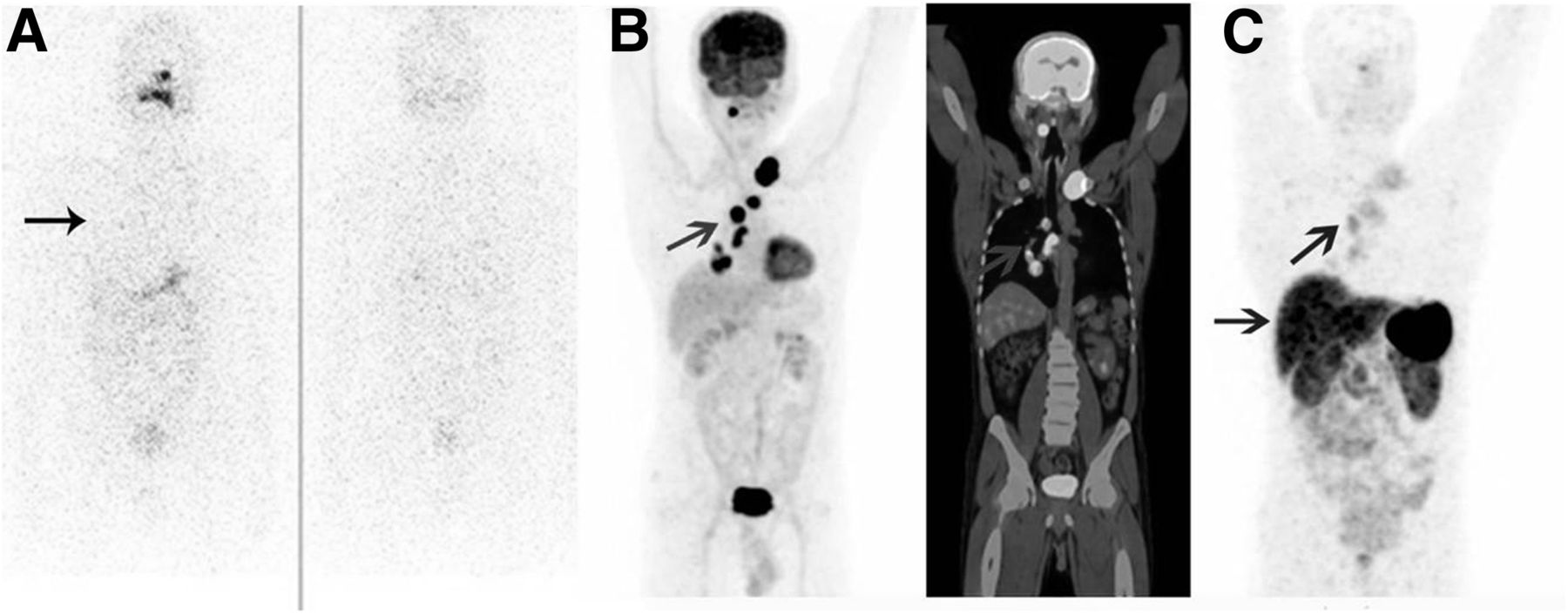
Whole-body 131I diagnostic scintigraphy scan (A), 18F-FDG PET/CT maximum-intensity-projection scan and coronal fused image (B), and 68Ga-DOTATATE maximum-intensity-projection scan (C) of known case of PTC in patient with raised serum thyroglobulin level. No abnormal 131I activity is seen in thoracic or neck regions. Intense 18F-FDG activity is seen in thoracic, left supraclavicular, and right upper parapharyngeal regions on 18F-FDG PET/CT, whereas 68Ga-DOTATATE scan shows faint tracer activity in these regions, as compared with liver. Arrows indicate tracer uptake or lack thereof. A color version of this figure is available as a supplemental file at http://tech.snmjournals.org.
- FIGURE 4.
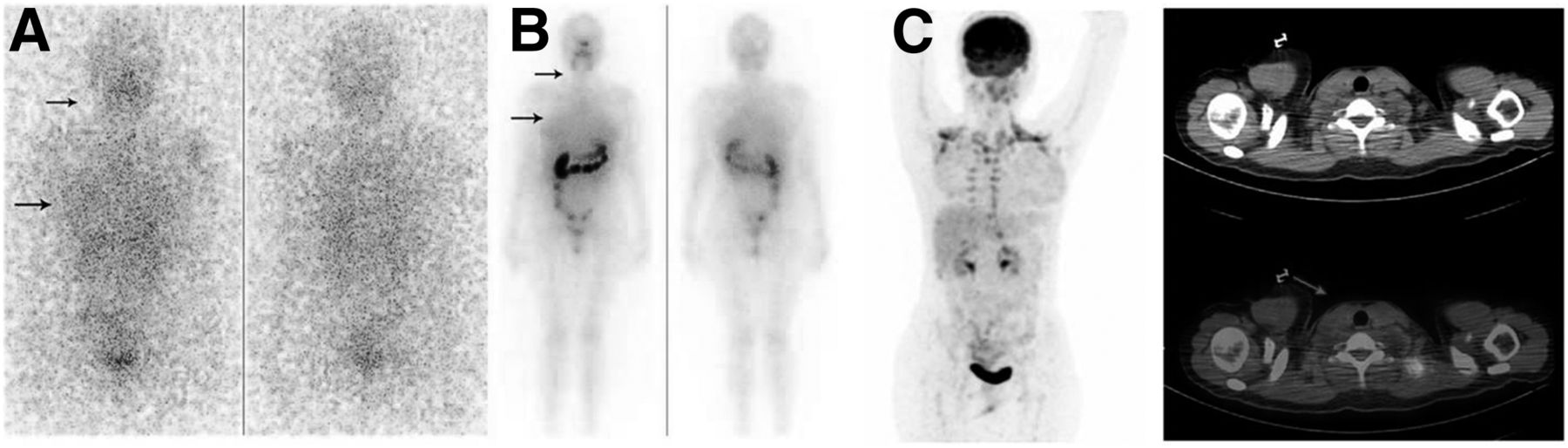
Whole-body 131I diagnostic scintigraphy scan (A), posttherapy (131I ablation) scintigraphy scan (B), and 18F-FDG PET/CT scan (C) of known case of PTC with raised serum thyroglobulin level. No abnormal 131I activity in neck or thoracic regions is seen on diagnostic or posttherapy scan. 18F-FDG uptake is seen only in brown fat of neck (lower arrow in C). Arrows indicate tracer uptake or lack thereof. A color version of this figure is available as a supplemental file at http://tech.snmjournals.org.
- FIGURE 5.
Whole-body 131I diagnostic scintigraphy scan (A), 18F-FDG PET/CT maximum-intensity-projection scan (B), axial PET/CT and CT images (C), and posttherapy (131I ablation) whole-body scintigraphy scan (D) of known case of PTC with raised serum thyroglobulin level. Diagnostic 131I scan show physiologic tracer activity in stomach and no abnormal tracer activity in thoracic region, whereas 18F-FDG activity is seen in left lung nodule, and posttherapy 131I scan shows tracer activity in left thoracic region. Arrows indicate tracer uptake or lack thereof. A color version of this figure is available as a supplemental file at http://tech.snmjournals.org.
- FIGURE 6.
(A) Whole-body 18F-FDG PET scans demonstrate no uptake in any skeletal metastatic lesion. Uptake is seen only in scalp lesion (for which patient presented to clinic). (B) Coronal T2-weighted (left) and postcontrast (right) MR images demonstrate hyperintense (on T2-weighted image), well-defined, invasive, heterogeneously enhancing soft-tissue lesion involving both tables of skull and extending to dural lining but remaining extraaxial. (C) Posttreatment 131I scan just before patient was discharged after second dose of 131I demonstrates extensive skeletal metastases concentrating 131I avidly. Incidentally noted is relatively low uptake in scalp lesion. (Reproduced with permission of (11).) MIP = maximum-intensity projection.
- FIGURE 7.
Posttherapy (131I ablation) whole-body scintigraphy scan (A), whole-body 18F-FDG PET/CT maximum-intensity-projection scan (B), and 2 levels of axial thoracic 18F-FDG PET/CT and CT images (C and D) of known case of follicular variant of PTC in patient with raised serum thyroglobulin level who had received total cumulative dose of 37 GBq (1 Ci) of 131I at time of imaging. Persistent tracer activity is seen in thoracic region (A and B), and 18F-FDG uptake is seen in mediastinal lymph nodes (C) and lung nodules (D). Arrows indicate tracer uptake or lack thereof. A color version of this figure is available as a supplemental file at http://tech.snmjournals.org.
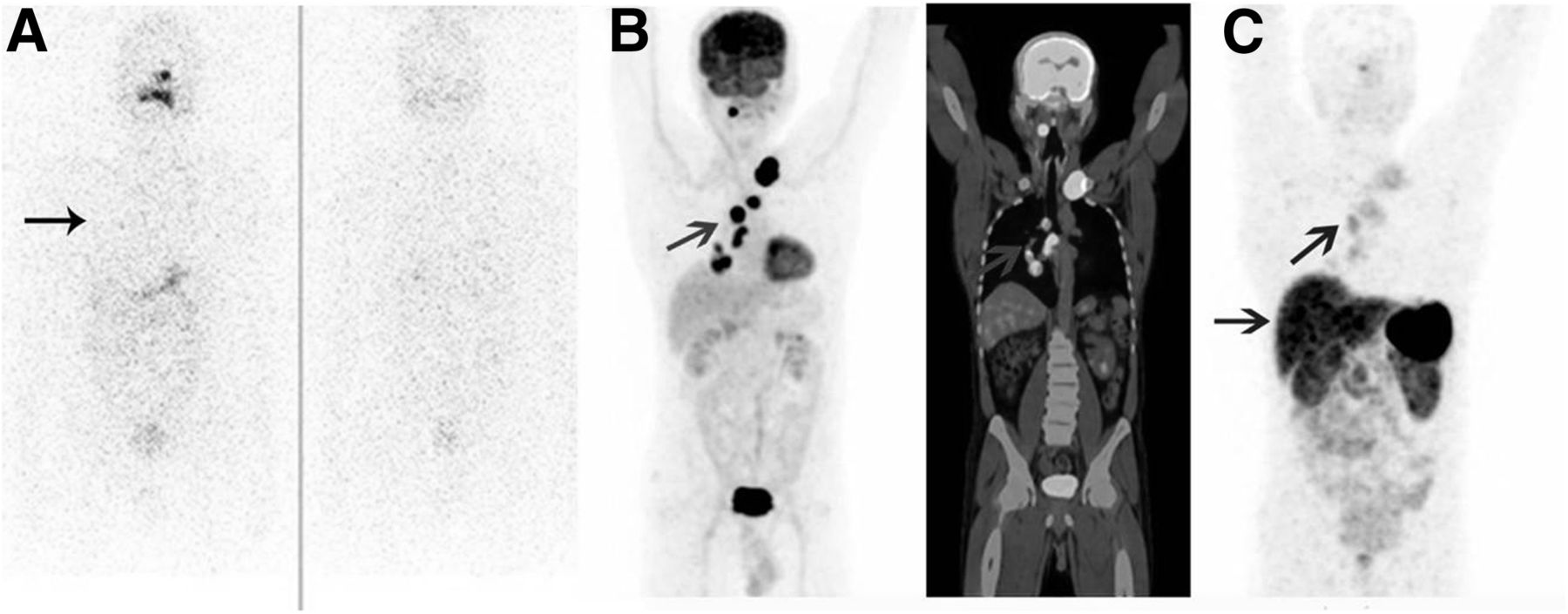
- FIGURE 8.
(A) Whole-body posttherapy (single fraction of 131I ablation) scintigraphy scan of DTC patient shows abnormal uptake in lung, solitary rib metastasis (posterior view), and neck. Whole-body posttherapy 18F-FDG PET/CT scan (C) shows no abnormal tracer activity in thoracic or neck region. (B) Subsequent follow-up 131I scintigraphy scan shows excellent response. Arrows indicate tracer uptake or lack thereof. A color version of this figure is available as a supplemental file at http://tech.snmjournals.org.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- METASTATIC DTC WITH SOME LESIONS DEMONSTRATING 131I UPTAKE
- TENIS SYNDROME WITH INCREASING 18F-FDG UPTAKE AND 68GA-DOTATATE AVIDITY
- TENIS SYNDROME WITH 18F-FDG–AVID LESIONS THAT ARE MINIMALLY OR NON–68GA-DOTATATE-AVID
- TENIS SYNDROME WITH NORMAL 18F-FDG PET/CT FINDINGS
- PREDICTION OF AGGRESSION IN A PARTICULAR LESION BY DUAL-TRACER IMAGING
- 18F-FDG UPTAKE AS AN OUTCOME DETERMINANT IN 131I-AVID LESIONS
- CONCLUSION
- DISCLOSURE
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.