


Abstract
This report illustrates an excellent partial response of Merkel cell carcinoma with multiple bilobar hepatic metastases to a single cycle of peptide receptor radionuclide therapy (PRRT) with 177Lu-DOTATATE. This response, coupled with minimal side effects, warrants consideration of this therapy early in the disease course (rather than at an advanced stage after failure of other therapies) if the metastatic lesions exhibit adequate tracer avidity on somatostatin receptor–based imaging. Our patient showed progression of systemic disease after having undergone a second surgery and adjuvant radiotherapy to the head and neck, as well as chemotherapy, and hence was considered a candidate for PRRT. In a pretreatment study, the metastatic lesions demonstrated avidity to both somatostatin receptors and 18F-FDG. Three months after the first cycle of treatment, when the patient was being evaluated for a second cycle, both imaging parameters showed evidence of a partial response that included nearly complete resolution of the two previously seen lesions. In view of the relatively good tolerability, minimal side effects, and targeted nature of the treatment, PRRT may evolve to become the first-line therapy for metastatic Merkel cell carcinoma and should be examined further in a larger number of patients.
Merkel cell carcinoma (MCC) is an aggressive dermatologic malignancy of the Merkel cells, which are situated just beneath the epidermis and close to nerve endings that receive the touch sensation. Known risk factors for the development of MCC are exposure to the sun, a weak immune system, and psoralen and ultraviolet A therapy for psoriasis (1). Because Merkel cells are thought to have a neuroendocrine origin and function, MCC is also referred to by the synonyms primary neuroendocrine carcinoma of the skin, cutaneous apudoma, primary small cell carcinoma of the skin, and trabecular carcinoma of the skin (1). Although patients who have small tumors without regional spread have a good prognosis after conventional treatment with radiation and chemotherapy (5-y survival, ∼80%), those with regional spread have a 5-y survival of only 50% and survival for all stages combined is 60% (2,3). Thus, new therapeutic options for metastatic MCC are needed to improve survival.
Examination with both light and electron microscopy and with immunohistochemistry are the primary means of definitively diagnosing the condition. Wide local excision with adjuvant irradiation is the usual treatment approach, with neck dissection added if there are clinically positive nodes. Contrast-enhanced CT has traditionally been the standard modality for staging, but the potential of 18F-FDG PET and somatostatin receptor-based 68Ga-DOTANOC/TATE PET/CT for staging has also been described (4,5). In an early report (4), metastatic disease in subcentimeter-sized lymph nodes was seen on pretreatment 18F-FDG PET/CT but not on CT, and posttreatment 18F-FDG PET correctly depicted a response to therapy. In a more recent report (5), on 24 MCC patients imaged with 68Ga-DOTATOC/TATE PET, the sensitivity of somatostatin receptor PET was 73% for nodal disease, 100% for bone, and 67% for soft-tissue metastases, and in two patients the first detection of brain metastases was on somatostatin receptor PET. These findings suggest the potential of PET imaging (both with 18F-FDG and somatostatin receptor–based) in MCC.
CASE REPORT
A 54-y-old man with Merkel cell carcinoma had undergone surgery twice. The first surgery was a wide local excision 3 y previously for a right malar skin nodule. The second surgery was because of recurrence in the same area along with involvement of the cervical lymph nodes, for which he had undergone excision of a recurrent right infraorbital skin nodule, right parotidectomy, and right neck dissection for right infraparotid and right submandibular lymphadenopathy. After the second surgery, he received external radiotherapy to the right head-and-neck region and adjuvant chemotherapy with capecitabine and temozolomide. He presented with recent-onset abdominal pain. Abdominal ultrasonography revealed two hypoechoic lesions (2.5 × 2 cm and 2.4 × 1.7 cm) in the right lobe of the liver. A contrast-enhanced abdominal CT scan showed multiple liver lesions, the largest being 2.0 × 1.8 cm. In view of systemic disease progression despite radiochemotherapy, he was considered a candidate for peptide receptor radionuclide therapy (PRRT), for which formal consent was obtained in accord with institutional norms.
PRRT with 177Lu-DOTATATE was considered in view of the positivity of the bilobar hepatic metastases on 68Ga-DOTATATE PET/CT (Krenning score of 3). The administered dose was decided according to our institutional protocol for neuroendocrine tumor (5,550–7,400 MBq) and according to the fixed-dose regimen mentioned in the joint guidelines of the International Atomic Energy Agency, European Association of Nuclear Medicine, and Society of Nuclear Medicine and Molecular Imaging (6). The patient was administered 5,735 MBq of 177Lu-DOTA-octreotate intravenously along with amino acids (for nephroprotection).
At follow-up, two lesions in segment VIII showed complete resolution on both 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT, and lesions in segments IVA, VI, and V showed reduced tracer avidity (Fig. 1). On 18F-FDG PET/CT, SUVmax decreased from 9.96 to 7.35 and 16.73 to 13.65 for the two segment IVA lesions, from 11.28 to 6.7 for the segment VI lesion, and from 14.91 to 11.89 and 11.12 to 9.8 for the two segment V lesions. In view of the patient’s excellent partial response and lack of symptoms at the 3-mo assessment, he was administered 7,400 MBq of 177Lu-DOTATATE as the second cycle of PRRT and is currently being monitored.
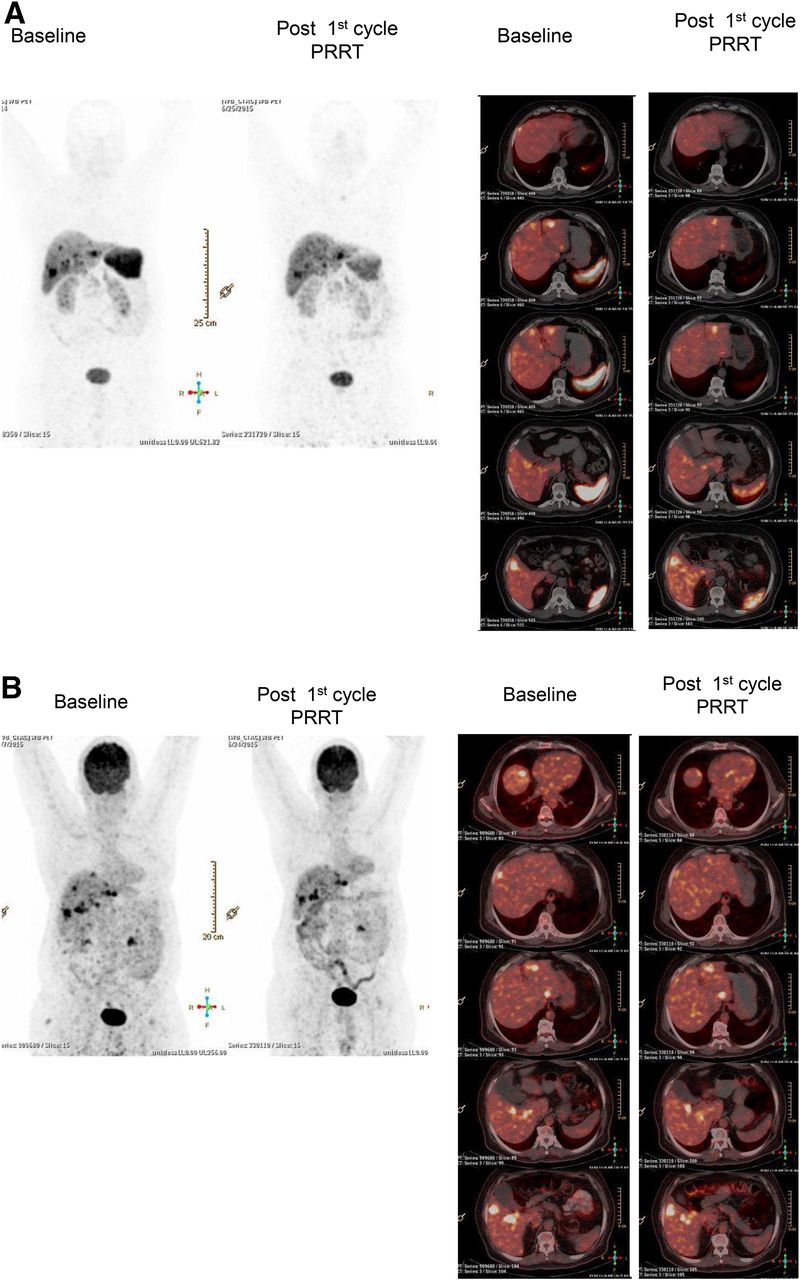
Maximum-intensity projection (left) and transaxial (right) slices from whole-body 68Ga-DOTATATE PET/CT (A) and 18F-FDG PET/CT (B) studies demonstrating nearly complete resolution of two lesions in segment VIII and reduced tracer avidity for lesions in segments IVA, VI, and V.
DISCUSSION
Targeted somatostatin receptor–based PRRT has emerged as a promising therapeutic approach in neuroendocrine tumors, specifically metastatic gastroenteropancreatic neuroendocrine tumors. This molecular receptor-targeted radionuclide therapy also holds promise for other malignancies that have a neuroendocrine component, such as metastatic medullary carcinoma of the thyroid and pulmonary neuroendocrine tumor, and hence is being increasingly explored in this clinical setting. Because of the relative rarity of MCC, there is no clear consensus about the best therapy when metastases are present and there is a need to examine new therapeutic regimens. Both of the published reports on PRRT for Merkel cell carcinoma involved the use of synchronous PRRT and radiosensitizing chemotherapy (7,8). In the report of Schmidt et al., two patients with progressive disease after chemotherapy were treated with PRRT and showed a temporary partial response, although they died 10 and 14 mo after the first clinical symptoms had appeared (7). Salavati et al. reported on a case of stage IV MCC for which synchronous PRRT and radiosensitizing chemotherapy brought about an impressive improvement in clinical symptoms; however, a mixed response was found on follow-up 18F-FDG and 68Ga-somatostatin receptor PET/CT (8).
Because the present case had shown recent disease progression after adjuvant radiochemotherapy, it was decided to administer only PRRT, to which objective evidence of a partial response was subsequently seen. The response was evaluated through 3 parameters: symptoms, imaging findings, and level of the tumor marker serum chromogranin A. The toxicity of the therapy was assessed by evaluating renal function, the hematologic profile, and liver function (detailed in Tables 1 and 2).
Kidney, Blood, and Liver Parameters at Baseline and 3 Months After First Cycle of PRRT
Kidney Parameters and Serum Chromogranin A at Baseline and 3 Months After First Cycle of PRRT
CONCLUSION
In view of the relatively good tolerability, minimal side effects, and good disease control of PRRT for metastatic Merkel cell carcinoma, it may evolve to become the first-line targeted therapy and needs to be examined further in high-powered prospective studies.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 15, 2015.
REFERENCES
- Received for publication July 8, 2015.
- Accepted for publication September 2, 2015.





{kind=link}