


Abstract
An aberrant right subclavian artery can be diagnosed by PET/CT, as demonstrated in this case of a 70-y-old man undergoing PET/CT for staging of squamous cell carcinoma of the right lung. It is important to report this finding during the evaluation of oncologic patients, to prevent severe complications that may arise from various oncologic interventions.
To our knowledge, this is the first case in the literature that describes the identification of an aberrant right subclavian artery on PET/CT. It is important to identify the presence of an aberrant right subclavian artery in order to prevent an erroneous diagnosis, an unnecessary imaging workup, and rare severe complications.
CASE REPORT
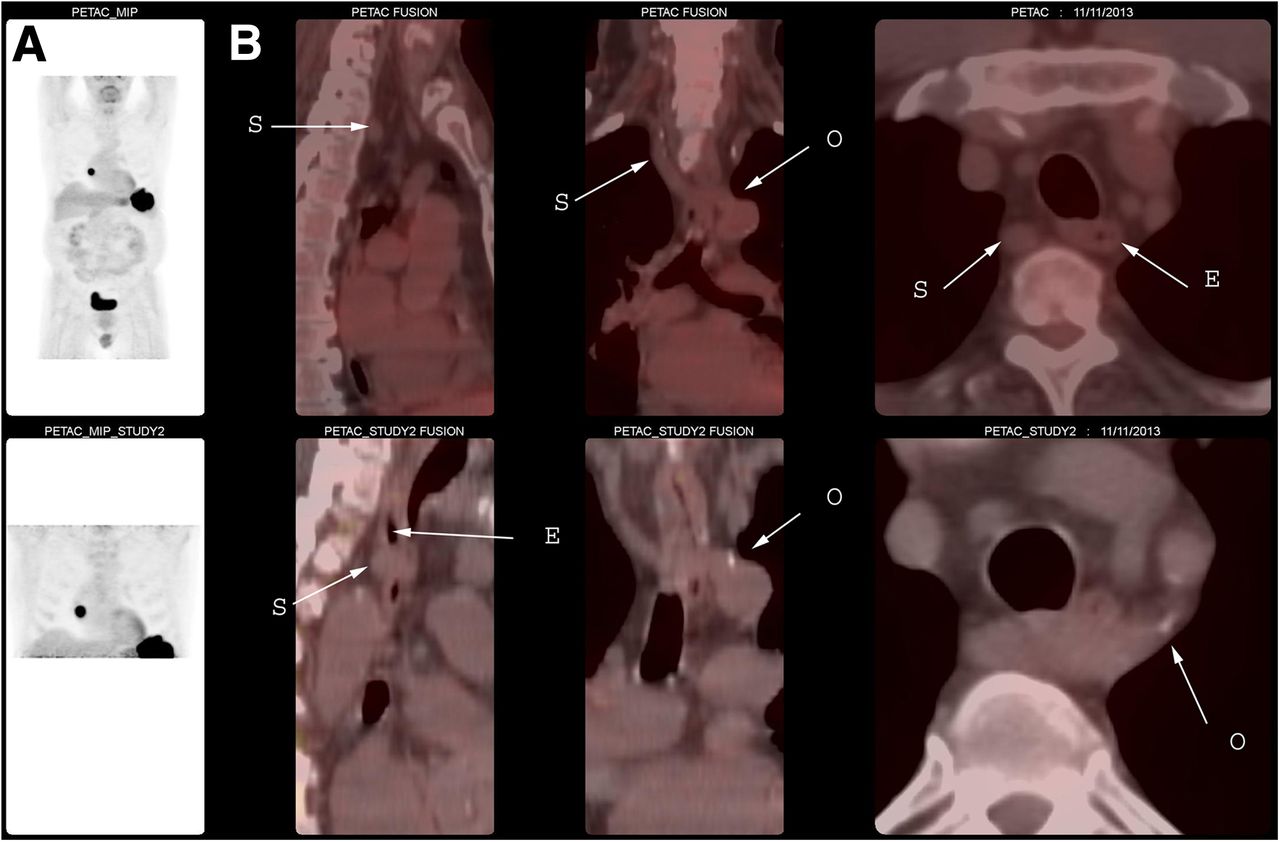
A PET/CT scan was ordered for staging in a 70-y-old man with a history of squamous cell carcinoma of the right lung. The imaging was performed on a dedicated 16-slice body PET/CT scanner (Discovery DST; GE Healthcare). Ninety minutes after intravenous administration of 619.01 MBq (16.73 mCi) of 18F-FDG under fasting conditions, sequential unenhanced CT images and then PET images were acquired. For the PET component, imaging was performed at each bed position for 3 min, using 6–8 bed positions to cover the entire body. A 3-dimensional high-sensitivity mode was used, with an axial field of view of 15 cm in a 256 × 256 matrix. The images were reconstructed iteratively on a 128 × 128 matrix using an ordered-subsets expectation maximization algorithm for 30 subsets and 2 iterations, with a 7.0-mm postreconstruction filter. For the CT component, the following imaging parameters were used: 140 kVp, 120–200 mA, 0.8 s per CT rotation, a pitch of 1.75:1, a detector configuration of 16 × 1.25 mm, a 3-mm slice thickness, and oral contrast material only. The PET scan was positive for an 18F-FDG–avid soft-tissue lesion in the right middle lobe and for a low-density lesion in the spleen. An aberrant right subclavian artery was also visualized posterior to the esophagus (Fig. 1).

Maximum-intensity-projection PET images (A) and fusion PET/CT images (B; sagittal view [left], coronal view [middle], and axial view [right]). E = esophagus; O = origin of aberrant subclavian artery from aorta; S = subclavian artery.
DISCUSSION
An aberrant right subclavian artery is a rare congenital anomaly with a reported incidence of less than 1%–2% (1–4). It results from regression of the right fourth aortic arch and persistence of the dorsal aorta (1,3,4). Patients with an aberrant right subclavian artery are mostly asymptomatic. However, dysphagia, stridor, thoracic pain, and cough are the most common symptoms (1). In more than 80% of cases, the aberrant right subclavian artery is posterior to the esophagus, making the artery susceptible to extrinsic compression—such as by placement of nasogastric or endotracheal tubes—that could lead to a right subclavian artery esophageal fistula causing severe upper gastrointestinal bleeding (2). It is essential to identify an aberrant right subclavian artery so that it may be included in the differential diagnosis of dysphagia in children as it may be overlooked by endoscopy (3). Given that there are no important vessels in the area between the esophagus and the spine at the level above the aortic arch, it is considered a safe area in patients undergoing esophageal dissection and is often uninvestigated before surgery. Thus, the surgeon should consider this condition because a transected aberrant right subclavian artery could lead to upper-limb ischemia (4). Barium contrast imaging of the esophagus, MR imaging, CT, and angiography are used to diagnose an aberrant right subclavian artery and its complications (1). In this case, PET/CT detected this condition as well. Surgery is reserved for symptomatic patients or those with an aberrant right subclavian artery aneurysm (1).
CONCLUSION
18F-FDG PET/CT can reveal an aberrant right subclavian artery. It is important to report this finding during the evaluation of oncologic patients, to prevent severe complications that may arise from various oncologic interventions.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
-
Published online Aug. 14, 2014.
- Received for publication January 19, 2014.
- Accepted for publication June 26, 2014.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.