


Abstract
In selected patients with differentiated thyroid carcinoma, 18F-FDG PET/CT has been shown to have added value. We present 2 clinical examples in the settings of both iodine-concentrating and non–iodine-concentrating lesions with tracheal involvement with special reference to its importance in planning of surgery or radioiodine therapy and assessing completeness of surgery. We believe that the use of PET/CT should be considered on a case-by-case basis and specifically when SPECT/CT is unavailable or has inconclusive findings.
This article presents 2 clinical examples of the added value of 18F-FDG PET/CT in managing neck recurrences of differentiated thyroid carcinoma (in the settings of both iodine-concentrating and non–iodine-concentrating lesions) with tracheal involvement. Special reference has been made to its importance with respect to the planning of surgery or 131I therapy.
CASE REPORTS
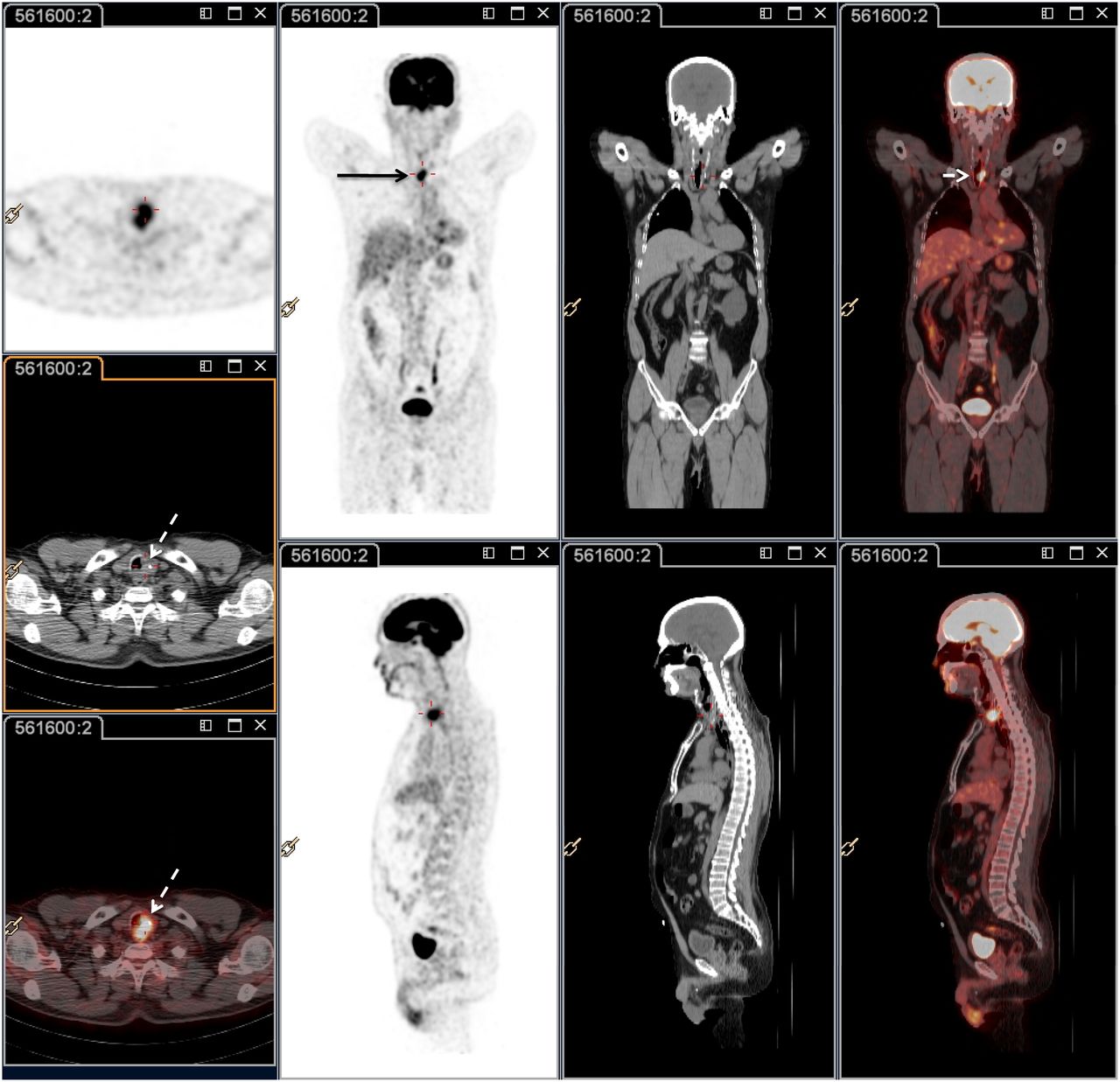
The first case was of a 67-y-old man who presented with an iodine-concentrating neck recurrence 2 y after radioiodine ablation therapy with 1,961 MBq (53 mCi) of 131I. The original tumor was differentiated papillary carcinoma of the thyroid with no evidence of nodal metastasis. The whole-body scan at that time (obtained with 82.88 MBq [2.24 mCi] of 131I) demonstrated foci of intense tracer uptake in the neck (midline and to its left). The stimulated serum thyroglobulin level was more than 250 ng/mL, the usual maximum titer that is provided at our institutional laboratory. Whole-body 18F-FDG PET/CT (Fig. 1) demonstrated a soft-tissue mass from the retrotracheal region in the left posterolateral aspect and encroaching on almost the entire lumen except for the right anterolateral aspect. An endoscopic view of the tumor showed it to be a left-sided tracheal mass just below the cricoid cartilage and extending over 2 rings. The tumor was widely excised with the first and second tracheal rings and adjacent paratracheal muscle coupled with tracheostomy. Overall, the tumor tissue measured 2.5 × 2.5 × 1.5 cm macroscopically. The histopathology report confirmed well-differentiated papillary thyroid carcinoma with invasion into the paratracheal muscle and tracheal cartilage. Two months after surgery, 18F-FDG PET/CT (Fig. 2) demonstrated persistent 18F-FDG uptake in the retrotracheal and left paratracheal regions (though less intense than in the presurgical study) but not demonstrating any extension or evidence of disease into the tracheal lumen. The diagnostic 131I study (with 129.5 MBq [3.5 mCi]) showed 2 distinct foci of tracer uptake in the neck, one at midline and the other on the left side. Thus, from the findings of both scans it could be concluded that although the intratracheal recurrence was completely removed during the surgery, disease in the left paratracheal and retrotracheal regions had not been completely removed and needed further treatment with radioiodine. The patient was treated with 5.55 GBq of 131I, and the posttherapy scan (Fig. 3) demonstrated 2 foci of radioiodine uptake in the neck corresponding to the foci noted in the diagnostic 131I study and on 18F-FDG PET/CT.
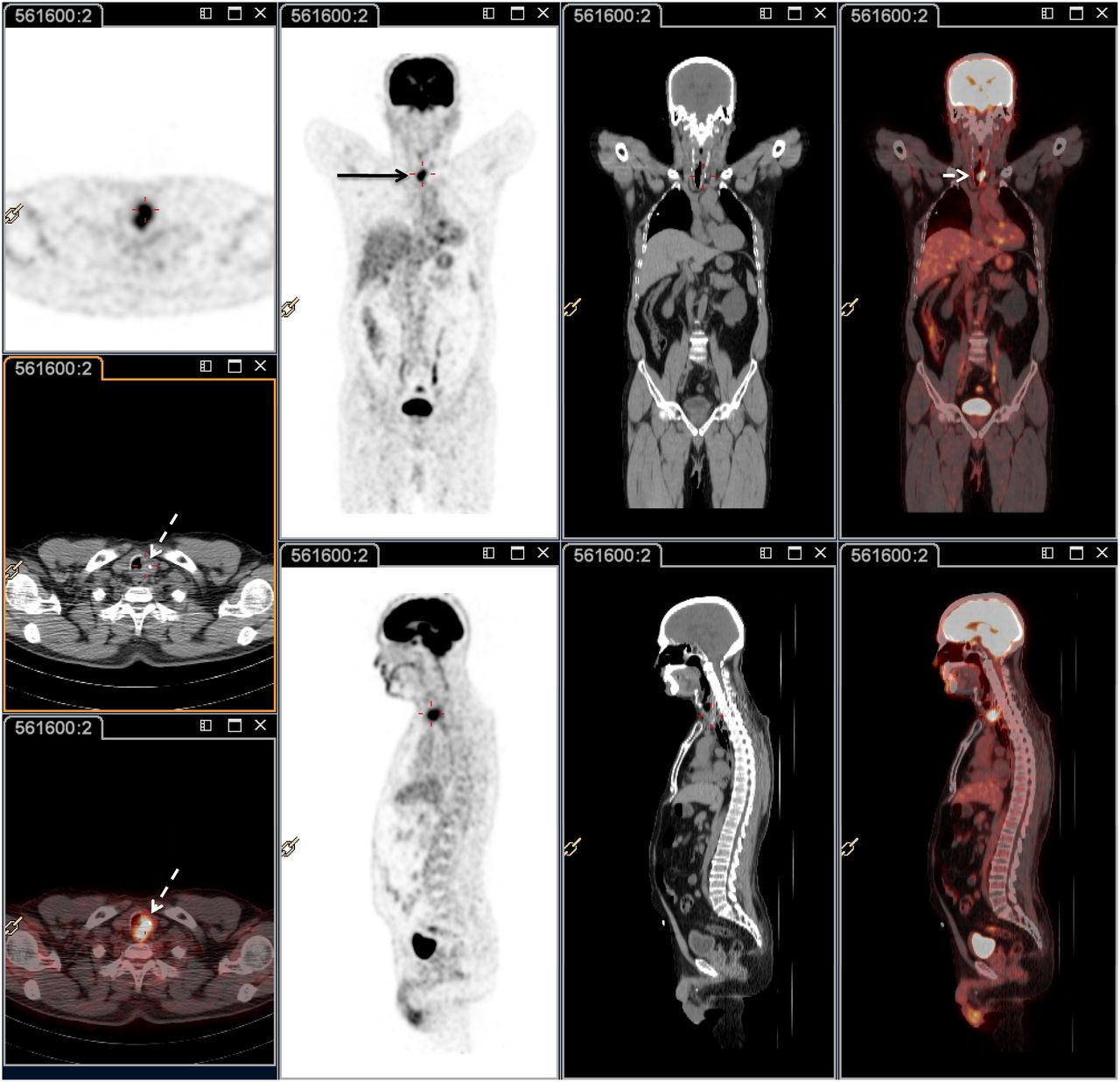
Whole-body 18F-FDG PET/CT scan of case 1 demonstrating soft-tissue mass from retrotracheal region and left posterolateral aspect that encroaches almost entire lumen except for right anterolateral aspect.
18F-FDG PET/CT scan (2 mo after surgery) demonstrating persistence of 18F-FDG uptake in retrotracheal region (though less intense than in presurgical study).

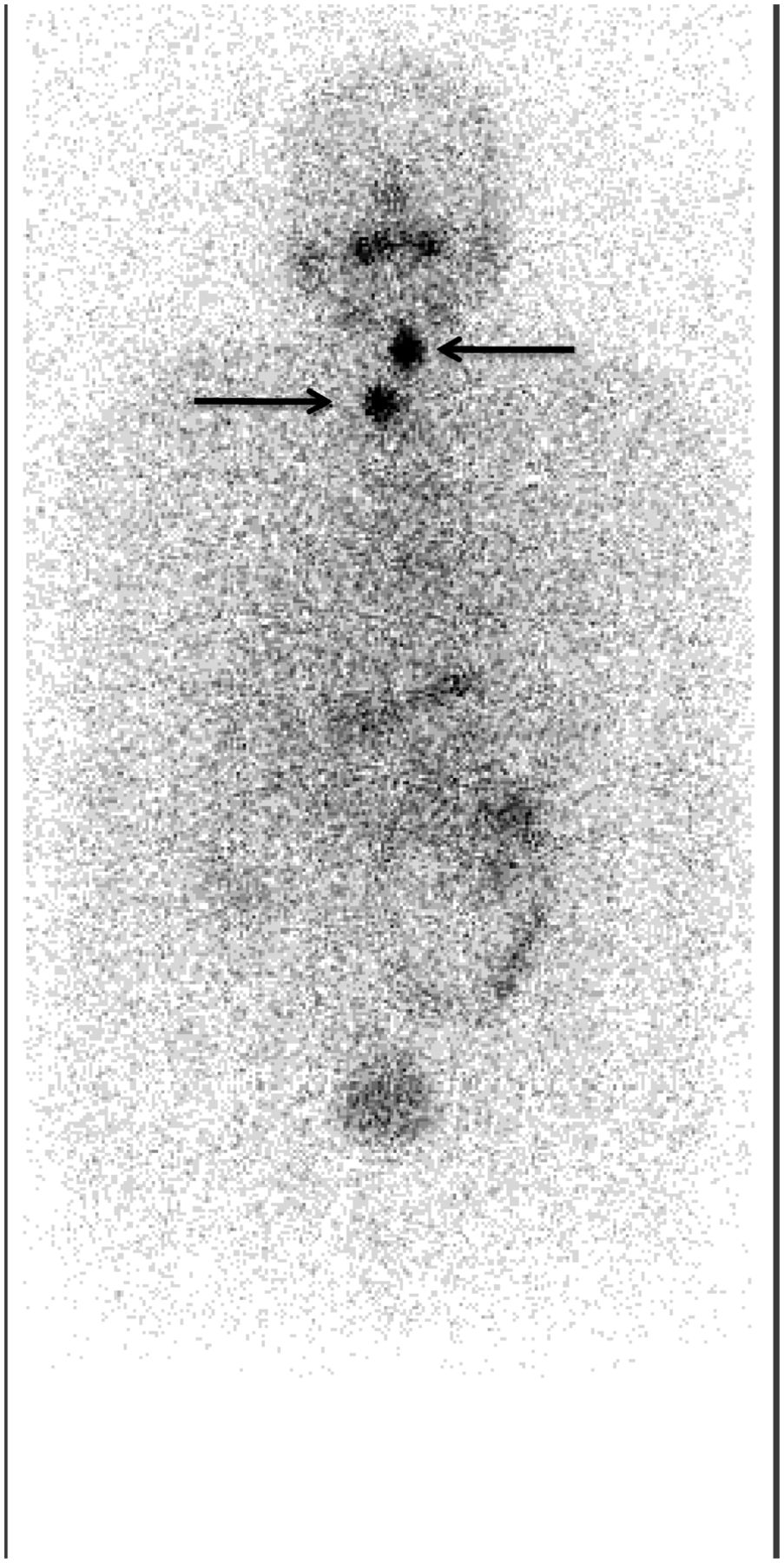
Posttherapy 131I scan demonstrating 2 foci (arrows) of radioiodine uptake in neck.
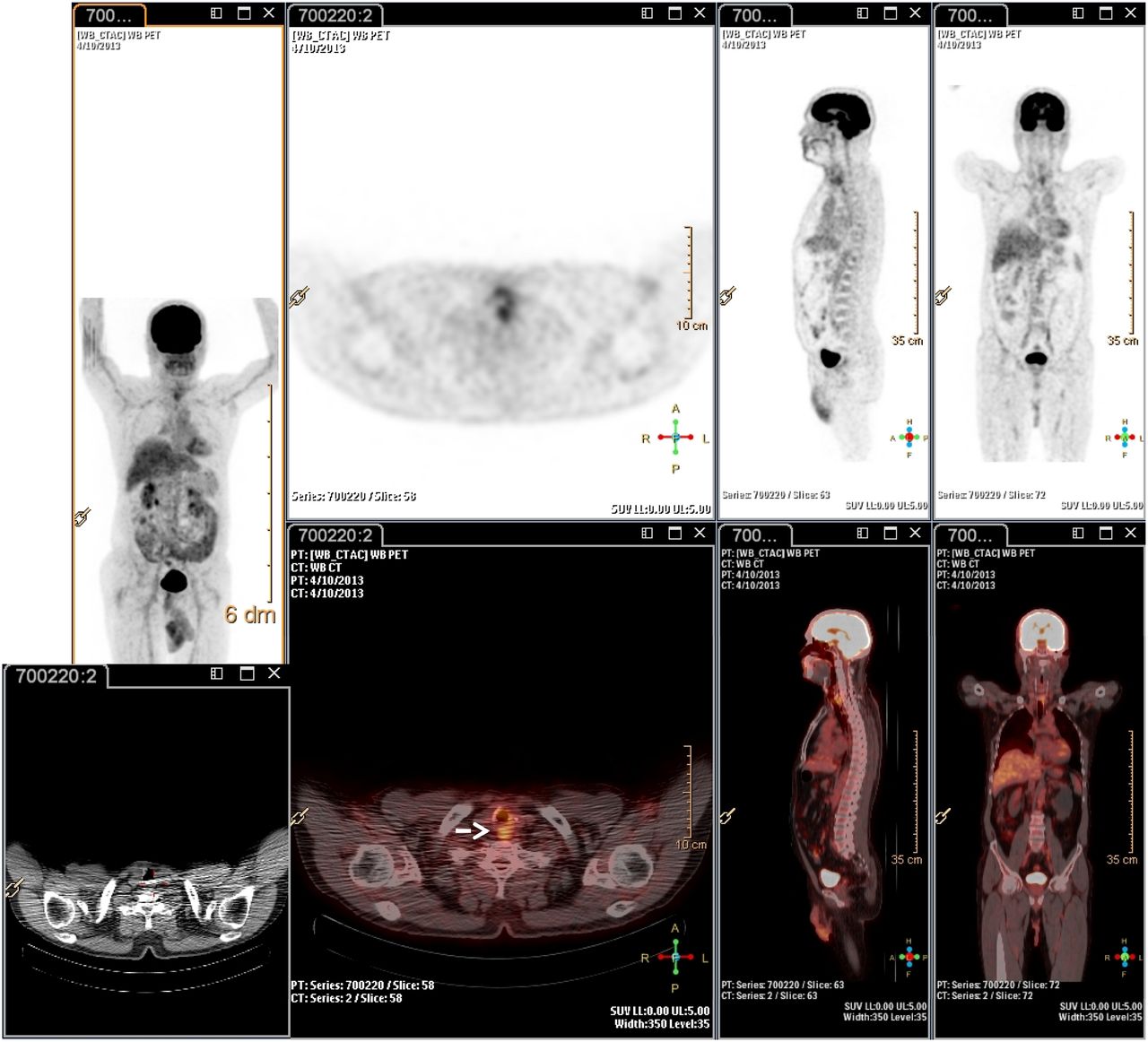
The second case was of a 74-y-old woman with differential thyroid carcinoma whose disease had been well controlled for 10 y but who then presented with a recent onset of increasing serum thyroglobulin (the most recent unstimulated thyroglobulin level had been 19 ng/mL). The original tumor was papillary carcinoma of the thyroid with extrathyroidal extension, with 1 of 3 lymph nodes showing evidence of metastasis. Whole-body radioiodine scanning (obtained with 118.4 MBq [3.20 mCi] 72 h after oral administration of 131I) showed no focal uptake suggestive of active disease (Fig. 4). The thyroid-stimulating hormone level at the time of the 131I scan was more than 100 μIU/mL. The patient was on a low-iodine diet as part of our routine protocol, and care was taken to exclude the possibility of a false-negative 131I result due to iodine interference. 18F-FDG PET/CT (Fig. 5) showed a focus of intense 18F-FDG uptake arising from the posterolateral aspect of the left side of the trachea and protruding into the lumen. A less intense focus seen in left level IV was shown on ultrasonography-guided fine-needle aspiration cytology to be metastatic from differential thyroid carcinoma. Left level IV nodal dissection and excision of an intratracheal soft-tissue mass measuring 1.2 × 1 × 0.8 cm was performed. The final histopathologic report confirmed the presence of metastatic papillary carcinoma in the intratracheal soft-tissue specimen and in 1 of 5 nodes, with perinodal extension. Follow-up 18F-FDG PET/CT showed no abnormal foci suggestive of residual disease, implying that the surgery had been adequate. The follow-up level of stimulated thyroglobulin was 2.1 ng/mL, and the patient is being observed on a regular basis.
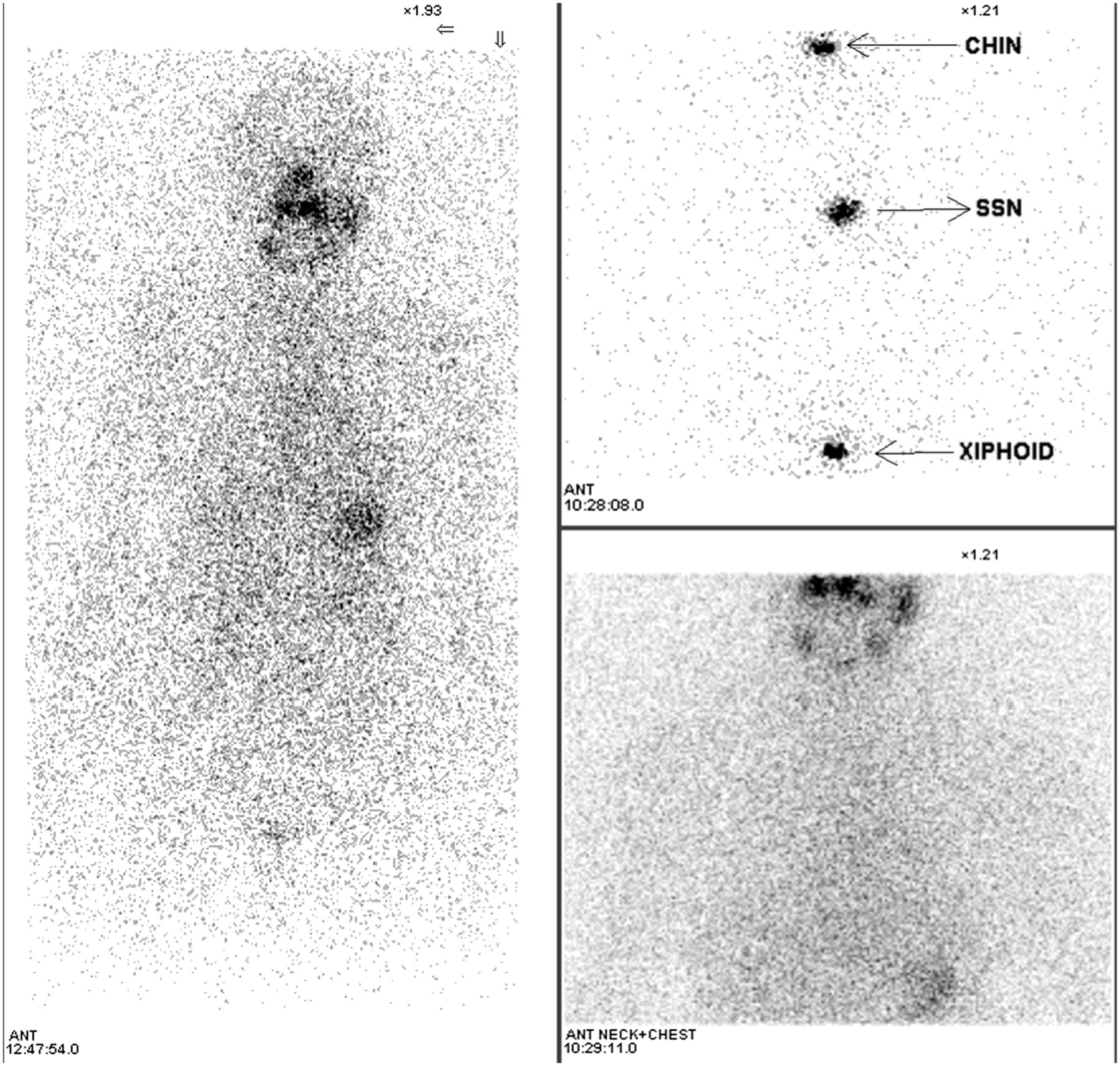
Whole-body radioiodine scan of case 2, which does not demonstrate any uptake to suggest focus of active disease. SSN = suprasternal notch.

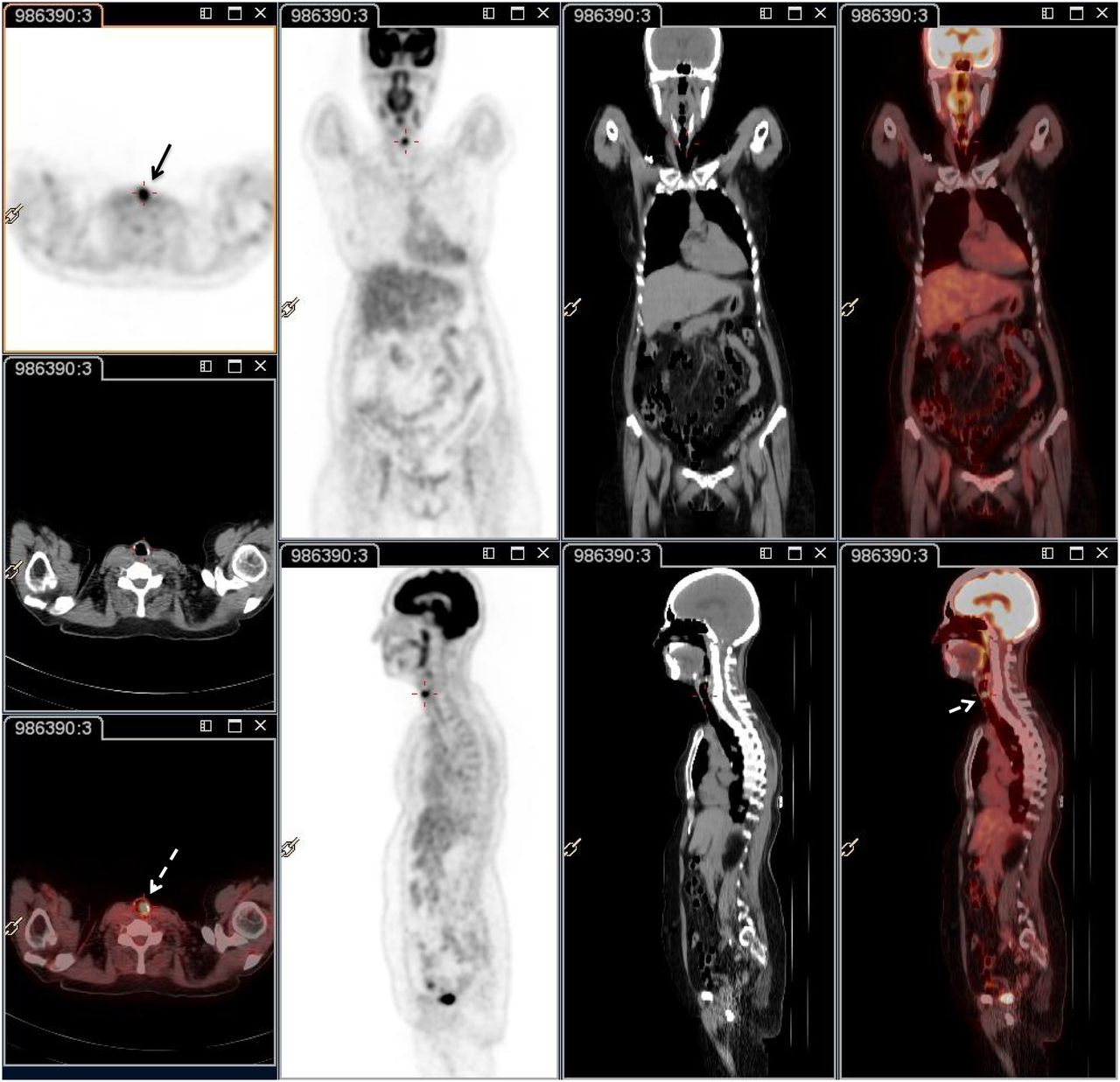
18F-FDG PET/CT scan demonstrating focus of intense 18F-FDG uptake that arises from left side of trachea (from posterolateral aspect) and protrudes into lumen (clearly visualized in triangulated transaxial, sagittal, and coronal slices of fused images). Also observed is less intense focus in left level IV, which on ultrasonography-guided FNAC was found to be metastasis from differential thyroid carcinoma.
DISCUSSION
The first case, of iodine-concentrating disease, classically demonstrates the importance of determining whether a recurrent neck lesion noted on planar 131I imaging extends within the trachea and thus requires tracheostomy before 131I therapy. Non–contrast-enhanced CT is imperative in this scenario, taking into account that such patients may be potential candidates for radioiodine therapy should the surgeon deem surgery not feasible. Thus, non–contrast-enhanced 18F-FDG PET/CT may serve a valuable role. Obviously, for accurate surgical planning, such characterization is pivotal (as seen in both cases), but equally important is evaluating the completeness of surgery and planning future 131I therapy of the residual lesions.
CONCLUSION
These two cases of differential thyroid carcinoma emphasize 3 added clinical benefits of 18F-FDG PET/CT: in the evaluation of patients who have an elevated level of thyroglobulin but negative findings on iodine scintigraphy, in disease prognostification, and in the detection of second malignancies. Various reports have also mentioned the utility of 18F-FDG PET/CT for evaluating suspected neck recurrences (1–5). The present communication exemplifies yet another advantage in applying 18F-FDG PET/CT to clinical decision making in patients with differential thyroid carcinoma. In both of our patients, the added value shown for 18F-FDG PET/CT in determining tracheal involvement, intratracheal extension, and the completeness of surgery had important decision-making implications for surgery and radioiodine therapy. The new hybrid systems that use state-of-the-art spiral CT scanners (up to 16-slice scanners that can generate images of diagnostic quality) can be of great value in precisely evaluating iodine-avid neck recurrences. We believe that with the availability of more such advanced SPECT/CT instruments, the use of PET/CT should be considered on a case-by-case basis and specifically when SPECT/CT is unavailable or has inconclusive findings.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 24, 2013.
REFERENCES
- Received for publication June 19, 2013.
- Accepted for publication August 8, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.