


Abstract
Red blood cells (RBC) labeled in vivo with 99mTc-pertechnetate are used worldwide in nuclear medicine departments. Methods: Here, we present a case of 99mTc-RBC labeling failure associated with chocolate intake in a 25-y-old woman, resulting in uninterpretable images. Because of this clinical observation, we performed in vitro RBC labeling on blood samples from volunteers after they consumed chocolate. Results: Chocolate intake inhibited the labeling rate, compared with the control condition, and significantly increased the 99mTc free fraction (34.1% ± 11.3% vs. 14.0% ± 1.2%). Conclusion: We cannot explain how this interaction could occur, but cacao components are known to modulate red cell and plasma oxidoreductive status and to modify red cell membrane permeability and plasticity. Therefore, for patients who can be considered likely to consume chocolate, such as young patients, we recommend that they limit their consumption of chocolate for 12 h before RBC labeling.
Labeling of red blood cells (RBCs) with 99mTc is a simple and sensitive method for evaluating total RBC mass, performing radionuclide ventriculography, and localizing gastrointestinal bleeding sites. Irreversible tracer trapping is achieved through 2 steps. The first is the accumulation of stannous pyrophosphate inside RBCs; during the second step, technetium pertechnetate anion reaches the internal compartment of the RBCs, is reduced by stannous ion, and subsequently binds to hemoglobin (1,2). 99mTc labeling of RBCs is known to be influenced by some medicines such as digoxin (3), by medicinal plants (4), and by the use of Teflon (DuPont) canulas (5,6). We report here the case of a 25-y-old woman referred for planar equilibrium radionuclide ventriculography because of suspected arrhythmogenic right ventricular dysplasia and for whom images were not interpretable. Known potential sources of image quality degradation were checked, and no explanation other than a strong chocolate intake was obvious. That observation led us to repeat the radionuclide ventriculography after the patient had discontinued chocolate consumption and to study the interference of chocolate intake on RBC labeling in vitro.
MATERIALS AND METHODS
In Vivo RBC Labeling and Image Acquisition
In vivo RBC labeling was done as routinely performed in our nuclear medicine department following manufacturer recommendations. Briefly, 10 mg of stannous pyrophosphate (Angiocis; Cisbio International) in 1.5 mL of physiologic serum were injected in a peripheral vein. After 30 min, 718 MBq of 99mTc-pertechnetate were intravenously injected. The patient was positioned supine. The electrodes used for cardiac gating were placed to ensure an optimal electrocardiography signal. The heart rate was in normal sinus rhythm and at 72 beats per minute. For electrocardiography triggering, we chose the best electrocardiography lead and checked that the R wave was always the marker of the onset of the cardiac cycle. The cardiac cycle was divided into 16 consecutive intervals, and the R-R interval tolerance window was set to 30%. The acquisition was performed in frame mode on a double-head γ-camera (ECAM; Siemens) with a low-energy high-resolution parallel-hole collimator. We used a 20% window centered on the 140-keV photopeak of 99mTc, a 64 × 64 matrix, and an acquisition zoom of 2.67. Imaging was performed in the 45° left anterior oblique orientation to obtain the best septal view and isolate activity arising from the right and left ventricles. An additional caudal–cephalic 5° tilt was used to better separate the left ventricle from the left atrium. Imaging was also performed in a 45° right anterior oblique orientation to better visualize the apical and inferior wall segments. The acquisition lasted for 6 min, corresponding to 420 cycles: 418 accepted and 2 rejected.
Images were analyzed on a Mirage (Segami) workstation. We used automatic and manual determination of the ventricular and background regions of interests. For manual processes, we used end-diastolic and end-systolic images, parametric images (phase and amplitude), and movie mode for an accurate definition of valvular planes.
In Vitro Labeling of RBCs with 99mTc and Sodium Pyrophosphate
We included 5 healthy adults (3 women and 2 men; age range, 32–52 y), who ate 150 g of chocolate (>60% cacao content) 12 h before and drank hot chocolate 2 h before blood collections. This protocol was designed to mimic the chocolate intake in the reported case. Control blood samples were collected from each individual after a 48-h period without chocolate intake. The volunteers were free of any apparent diseases.
The operator labeling the cells was unaware of whether the volunteers had consumed chocolate. Briefly, 5-mL venous blood samples were drawn into Vacutainer tubes (Becton, Dickinson and Co.) containing sodium heparin and were labeled in vitro with 99mTc using sodium pyrophosphate (Angiocis; Cisbio International) as reducing agent. Freshly prepared sodium pyrophosphate (25 μL of a 40 μg/mL solution) was added to the blood samples (final concentration, 1 μg/mL). After 15 min of incubation at 20°C, 2 MBq of 99mTc-pertechnetate recently milked from a 99Mo/99mTc generator (Elumatic; Cisbio International) were added to the blood samples and incubated 30 min at 20°C. The samples were then centrifuged (1,200–1,500g) for 5 min at 20°C, and the supernatant and RBCs were separated. Finally, the radioactivity of the blood sediment and supernatant was assessed using a Medi 404 Activimeter (Medisystem), and RBC labeling efficiency was calculated.
Statistical Analysis
Data are presented as mean ± SD and were statistically compared using the paired Student t test. Significance was defined as a P value of less than 0.05.
RESULTS
Radionuclide Ventriculography After High Chocolate Intake
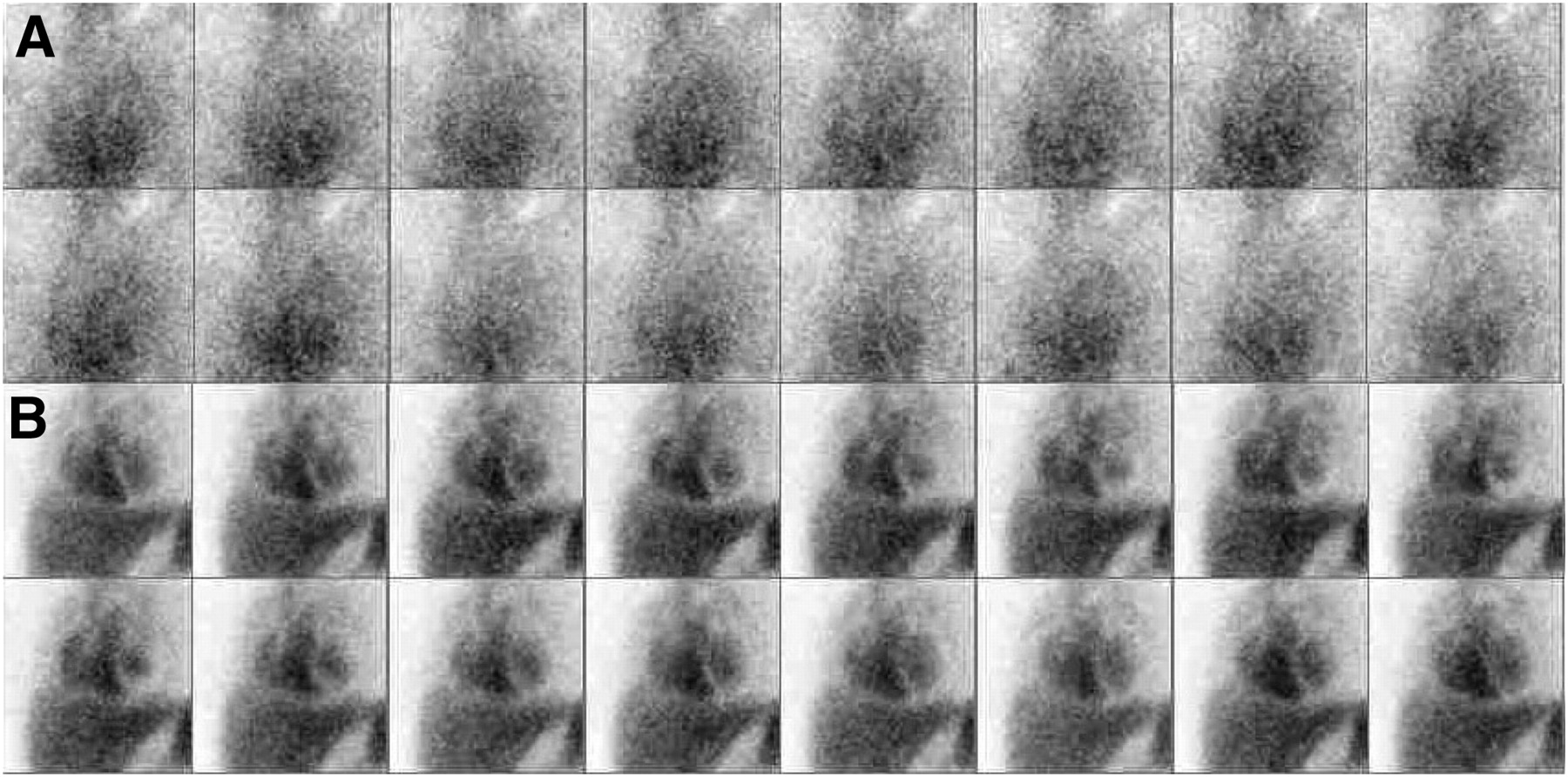
Image analysis showed poor counting statistics, a high level of background activity, and a reduced target-to-background ratio (Fig. 1A). We could not adequately separate the left ventricle from other cardiac chambers or from the tissue background (Fig. 2A–D). The left ventricular region of interest could not be automatically or manually determined.
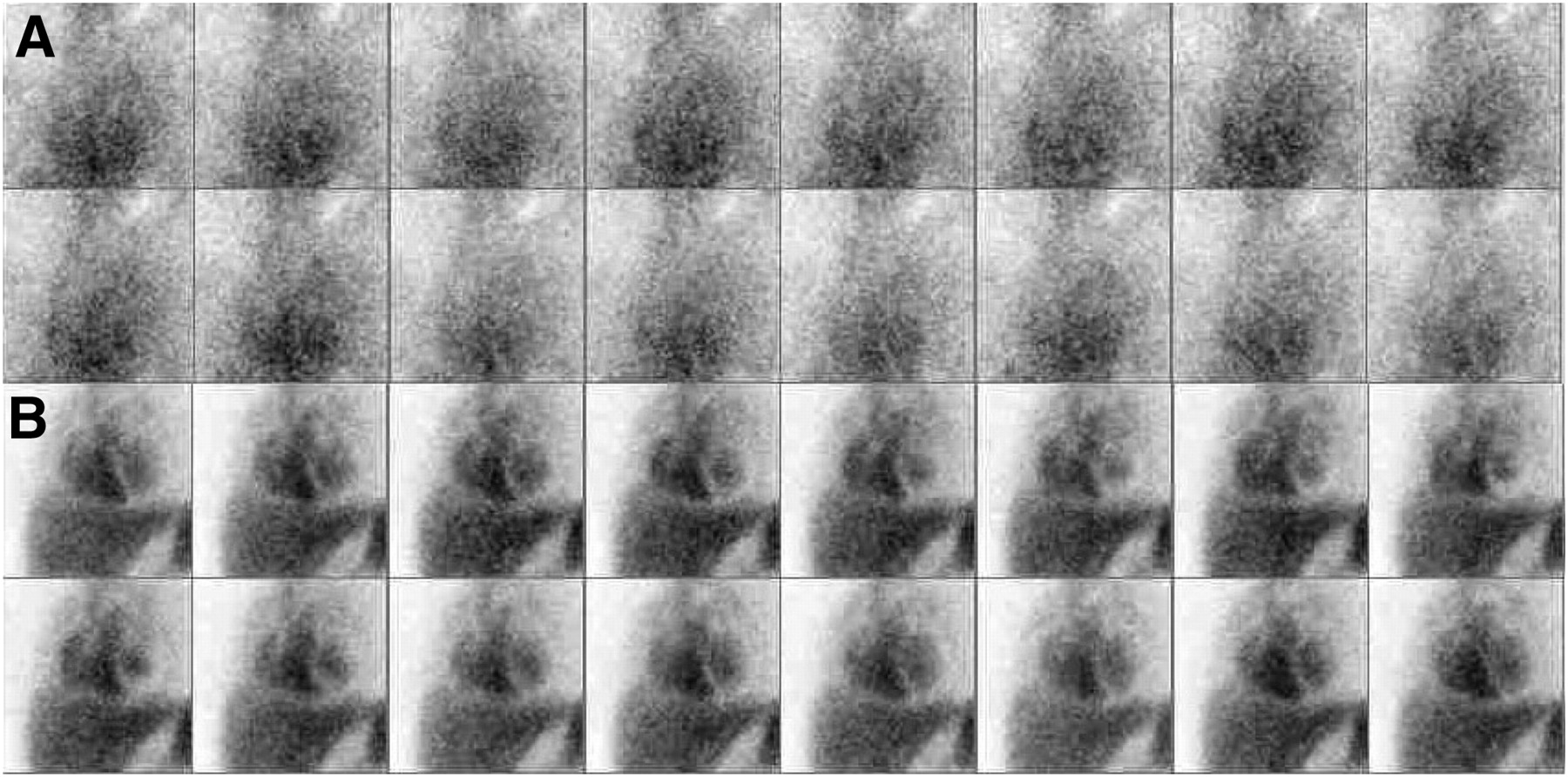
Synchronized radionuclide ventriculography (16 gates per cycle) with (A) and without (B) chocolate intake. Counting statistics are poor and background noise high after chocolate intake (A).

Ventriculography with (top) and without (bottom) chocolate intake: telediastolic 45° left anterior (A and E) and right anterior (B and F) oblique orientations; comparative phase images (C and G) and histograms (D and H). On first examination (A–D), ventricles cannot be adequately separated, resulting in uninterpretable images. Second ventriculography (E–H) shows much better image quality, with normal global ejection fraction and phase.
The high target-to-background ratio was consistent with insufficient counting statistics or inadequacy of radiolabeling. There was no obvious explanation for the observed inadequacy of the counting statistics. Injected activity, acquisition duration, and spectrometric window were correct. There was no gating error: the cardiac rhythm was regular, with sufficient accepted cycles and only 2 rejected cycles during the acquisition. The patient was not taking any medication (e.g., chemotherapy, β-blockers, heparin, or digoxin) reported to decrease RBC labeling efficiency or to reduce the target-to-background ratio (7). Consultation with the patient revealed that she had consumed a large amount of chocolate the evening before the examination and a hot chocolate beverage 2 h before. No free 99mTc-pertechnetate was suspected, because neither the thyroid gland nor the stomach could be visualized. We noticed an increase in urinary elimination of the radiotracer on static renal images. Finally, our lack of interpretable results could not be explained by problems with camera uniformity or spectroscopy or by movement of the patient.
Because of the compromised image interpretation, planar radionuclide ventriculography was performed again 2 mo later, and we asked the patient not to consume any chocolate for at least 1 d before the examination.
Radionuclide Ventriculography Without Prior Chocolate Intake
99mTc-pertechnetate (732 MBq) was infused 50 min after 10 mg of stannous pyrophosphate had been injected intravenously. All acquisition parameters were strictly identical to those presented above. For the same region of interest, in the center of the left ventricular cavity, the number of counts was twice that in the previous examination. The image quality allowed us to correctly interpret the findings (Figs. 1B and 2E–2H): global ejection fraction was normal, with normal phase and kinetics.
Reduced In Vitro RBC Labeling Efficiency After Chocolate Intake
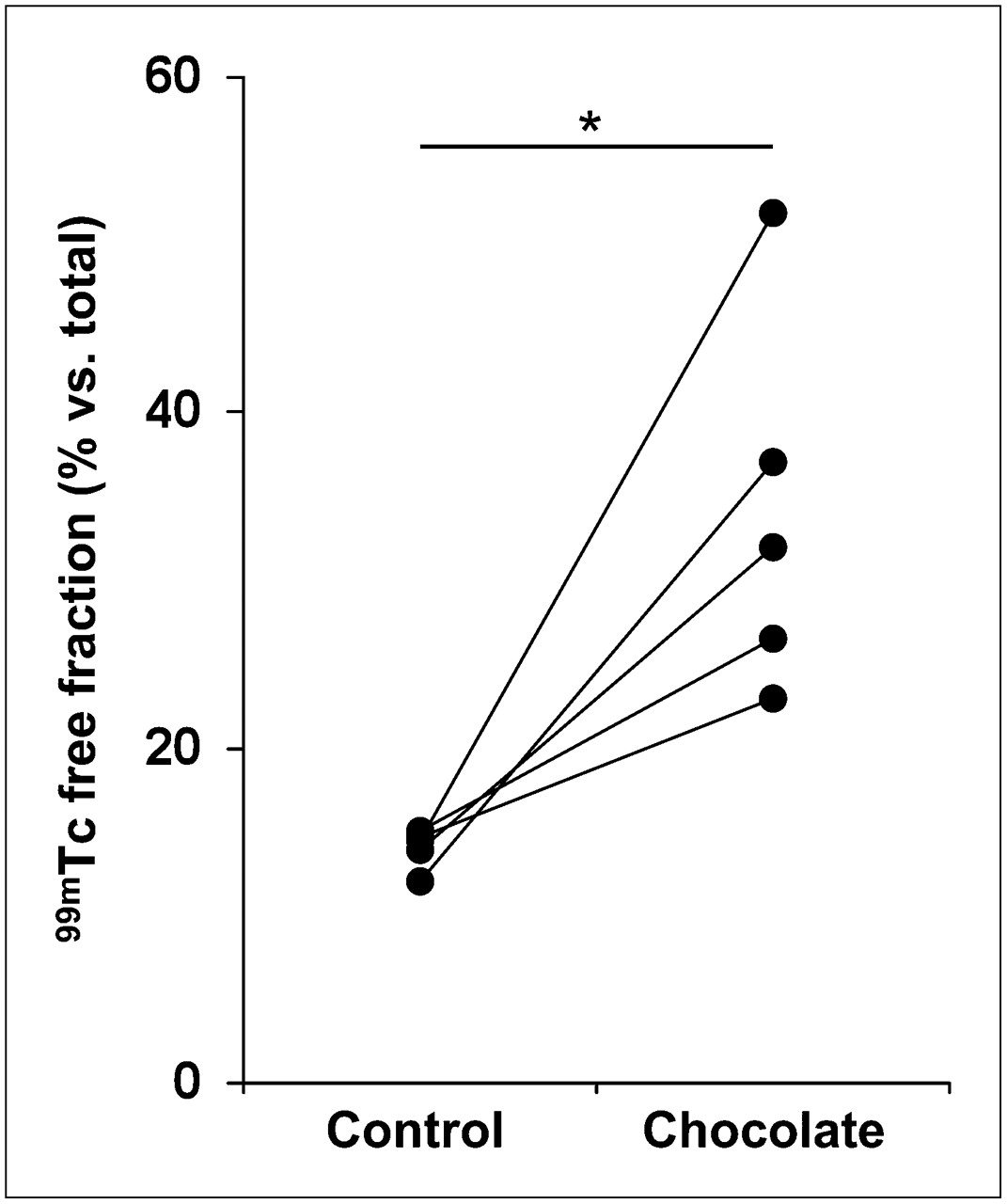
The effect of chocolate intake on RBC labeling rate by 99mTc and stannous pyrophosphate is shown in Figure 3. Chocolate intake markedly inhibited the RBC labeling rate, with a significant increase (P = 0.018) in 99mTc free fraction (34.1% ± 11.3%), compared with the control condition (14.0% ± 1.2%). In addition, the 99mTc free fraction was more variable after chocolate consumption (23%−52%) than under the control condition (12%−15%).
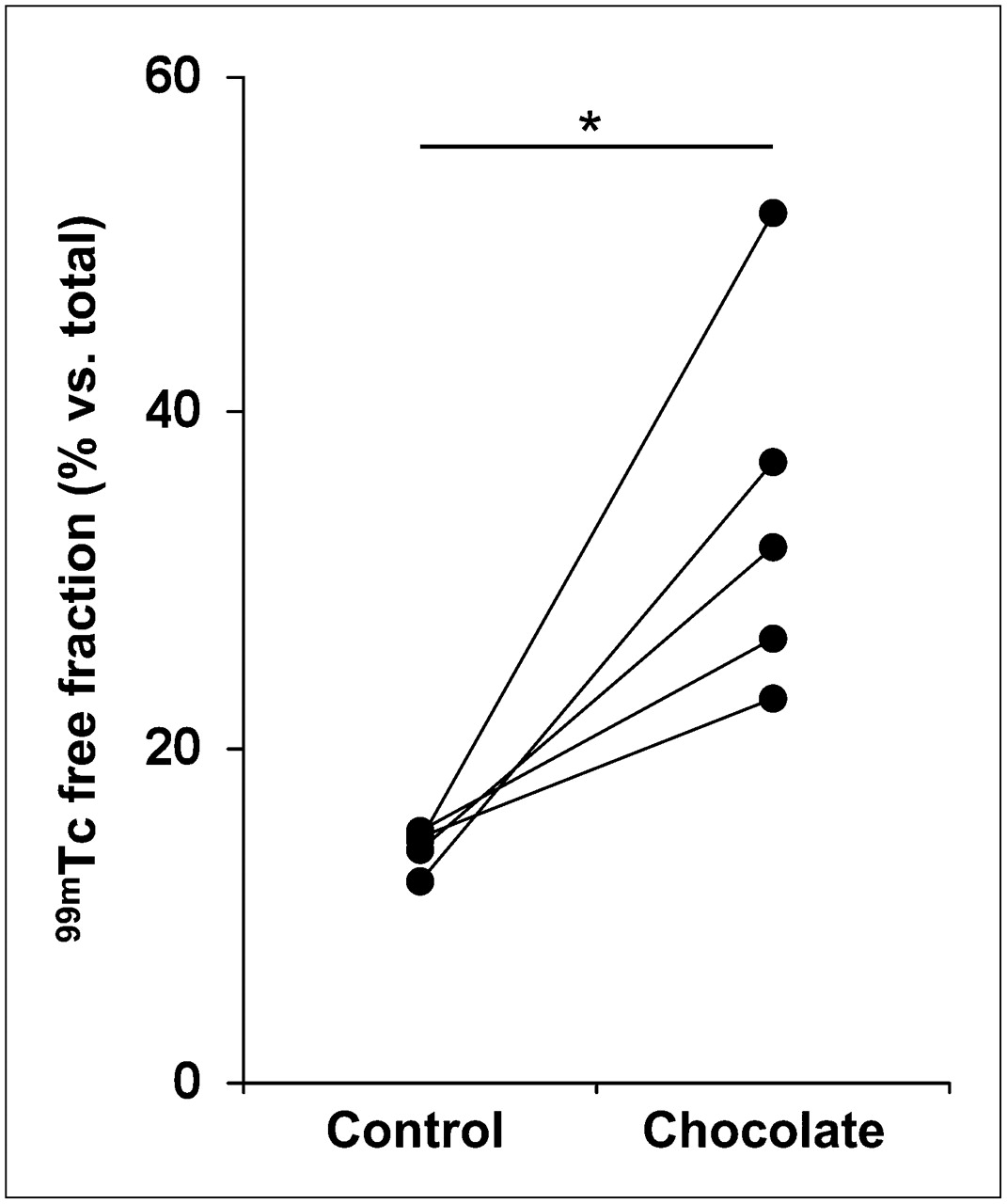
Reduction in RBC labeling efficiency after chocolate intake: residual plasmatic free 99mTc with (chocolate) or without (control) chocolate intake before in vitro 99mTc-RBC labeling (n = 5). *P = 0.018.
DISCUSSION
We have reported here a clinical case of compromised interpretation of radionuclide ventriculography findings associated with an excessive consumption of chocolate during the 24 h before 99mTc-RBC labeling. Scintigraphy was repeated 2 mo later without chocolate intake and produced interpretable images. The absence of other factors known to modulate RBC labeling efficiency brought us to suspect chocolate consumption as the source of the compromised interpretation. Therefore, we performed in vitro RBC labeling on blood samples of 5 volunteers with or without chocolate intake and found a significant reduction of labeling efficiency after chocolate intake.
Although we cannot establish a direct link between our reported case and our in vitro results, we argue that the in vitro data can partly explain the clinical observations—particularly, the high level of background activity, the reduced target-to-background ratio, and the high urinary excretion of tracer. In fact, our in vitro study revealed that unbound 99mTc after chocolate intake increases from 2 to 4 times according to the volunteer tested and can represent up to 52% of total activity. An increase in 99mTc free fraction of this intensity can induce in vivo, as we observed in our patient, a high background activity and can compromise image interpretation. Such an increase in background activity after in vivo RBC labeling has been reported in rats in the presence of digoxin or prazosin (3). In that work, the authors did not observe stomach or thyroid tracer accumulation. That observation, which supports our results, argues for the presence of 99mTc reduced species in plasma and tissue rather than for the presence of 99mTc-pertechnetate. The flavonoids in cacao are predominantly catechins and condensed procyanidins (8). These molecules are well known to modulate red cells or plasma oxidoreductive status (9,10), which in turn modulates pertechnetate ion reduction. Flavonoids have also been reported to accumulate at the RBC membrane surface and to modulate membrane permeability (11). In addition, cacao is a rich source of methyl-xanthine theobromine, also known to modulate red cell membrane fluidity (12,13). Either interaction could decrease stannous pyrophosphate entry in RBCs, as evoked in the presence of digoxin by Lee et al. (3). They could also induce a pertechnetate ion reduction in the plasma compartment in accordance with the absence of tracer trapping in the thyroid, salivary glands, and stomach.
CONCLUSION
To our knowledge, this report is the first dealing with a putative interaction between chocolate intake and RBC labeling. Even though the patient of our case report confessed to having abused chocolate the night before imaging, we recommend that chocolate consumption be limited for at least 12 h before radionuclide ventriculography using 99mTc-RBC labeling.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 6, 2009.
- Accepted for publication February 23, 2009.





{kind=link}
{kind=link}
{kind=link}