


Article Figures & Data
Figures
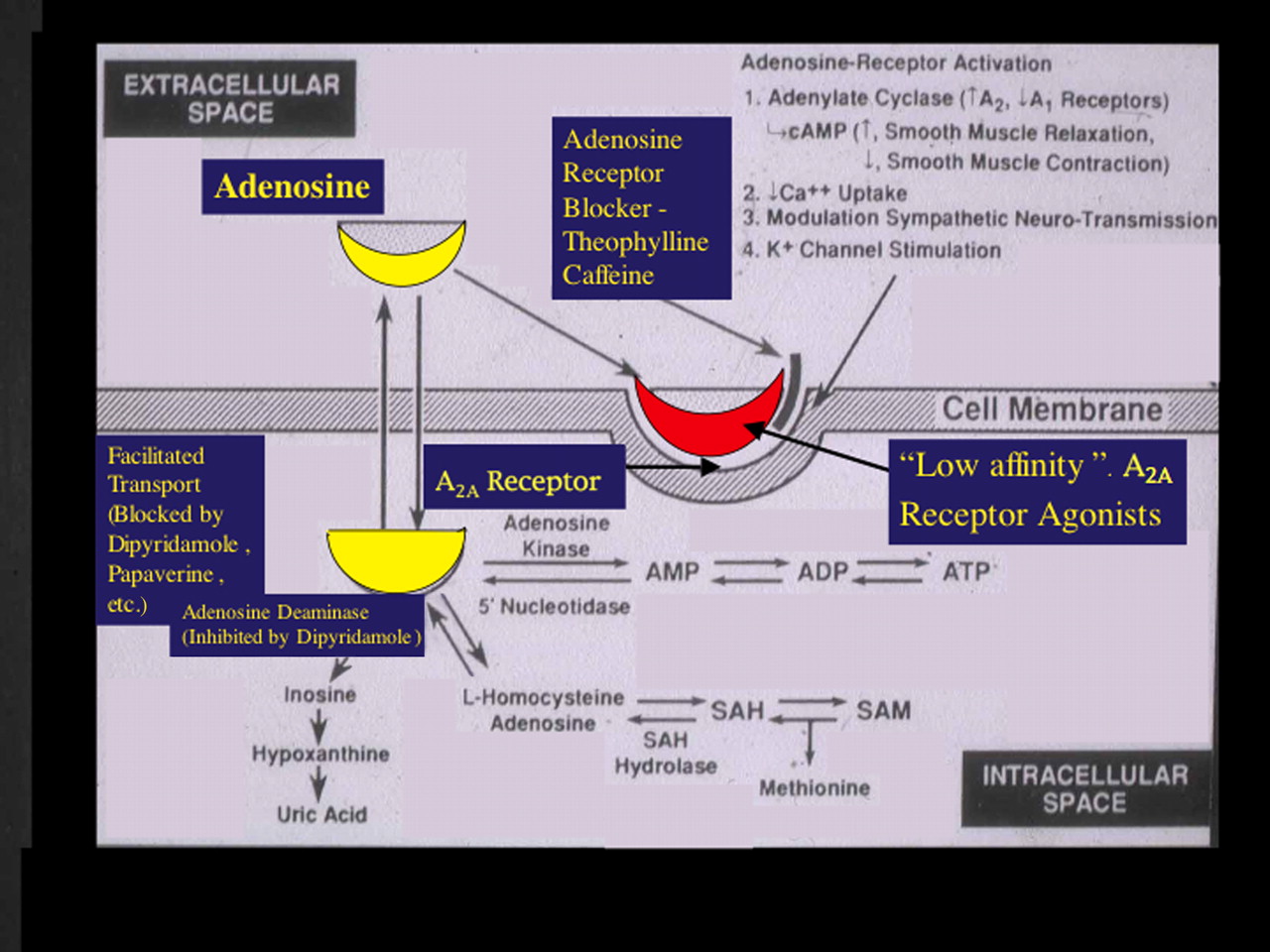
- FIGURE 1.
Shown are pathways of adenosine production transport, receptor activation, and metabolism. (Adapted with permission of (10).)
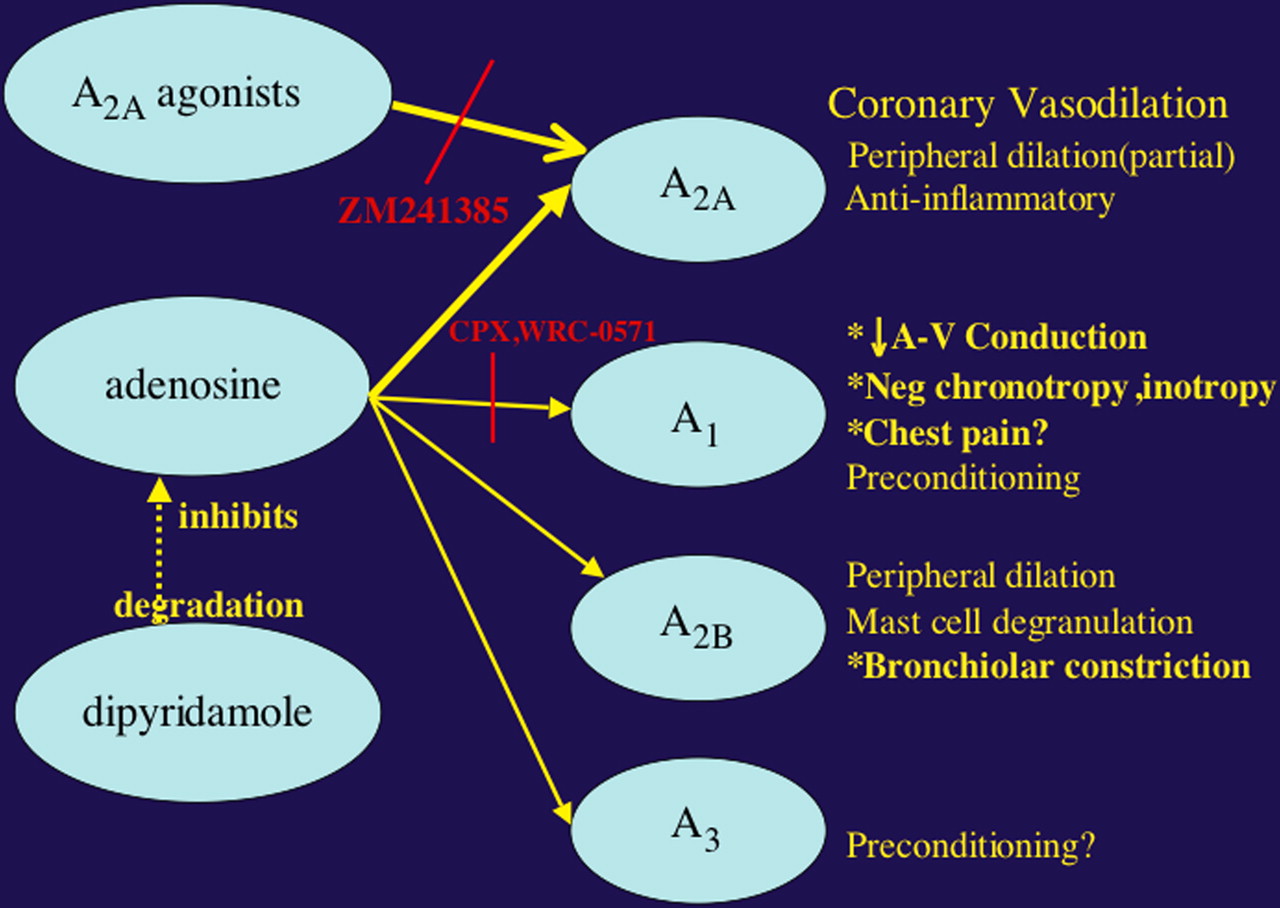
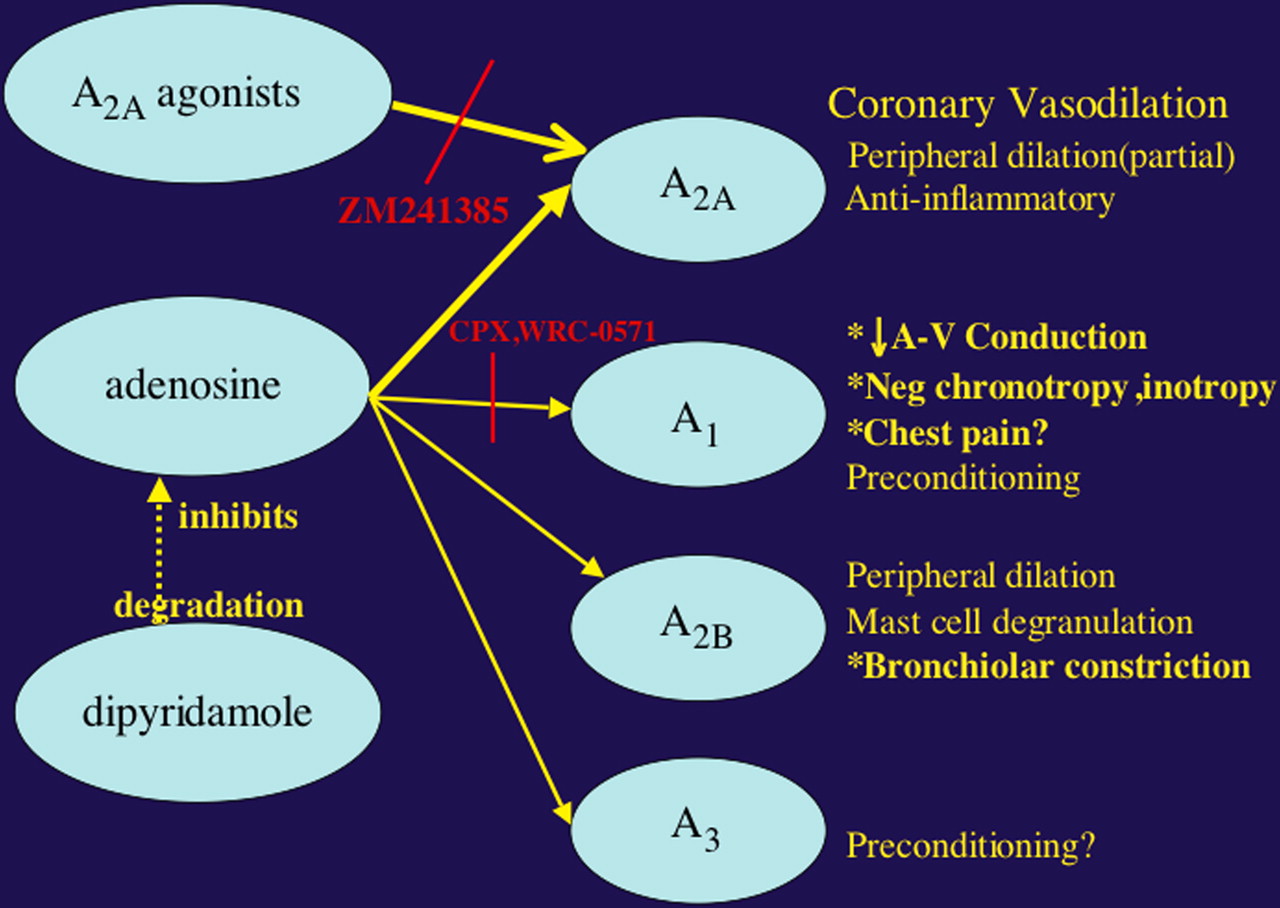
- FIGURE 2.
Four adenosine receptor subtypes—A1, A2A, A2B, and A3—have been characterized and cloned. Stimulation of these receptors accounts for varied effects on electrical conduction, vasodilation, and bronchoconstriction. Illustrated are several adenosine receptor agonists and physiologic responses that result from stimulation of selective receptor subtypes. Shown also are inhibitors of 2 pathways. (Adapted with permission of (28).)
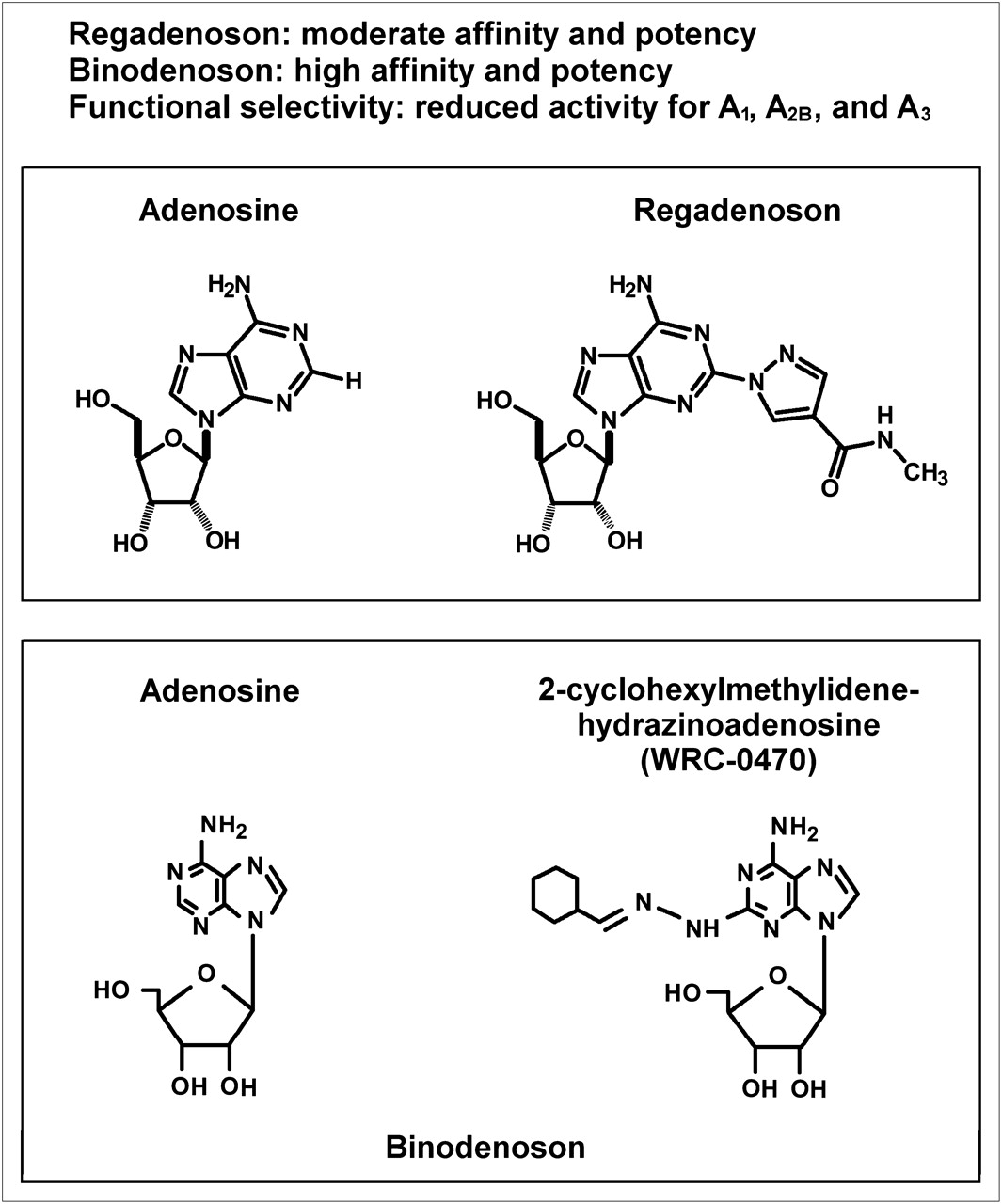
- FIGURE 3.
Shown are chemical compositions for regadenoson and binodenoson, compared with adenosine. Also presented are parameters of affinity and potency along with demonstration of its functional selectivity for A2A receptors. Affinity relates to tightness of binding of agent to receptor and its resultant duration of action. Adenosine is a low-affinity agent that is quickly released. Higher affinity of new and more specific A2A agonists does not seemingly interfere with preferential aminophylline binding and its use as antidote.
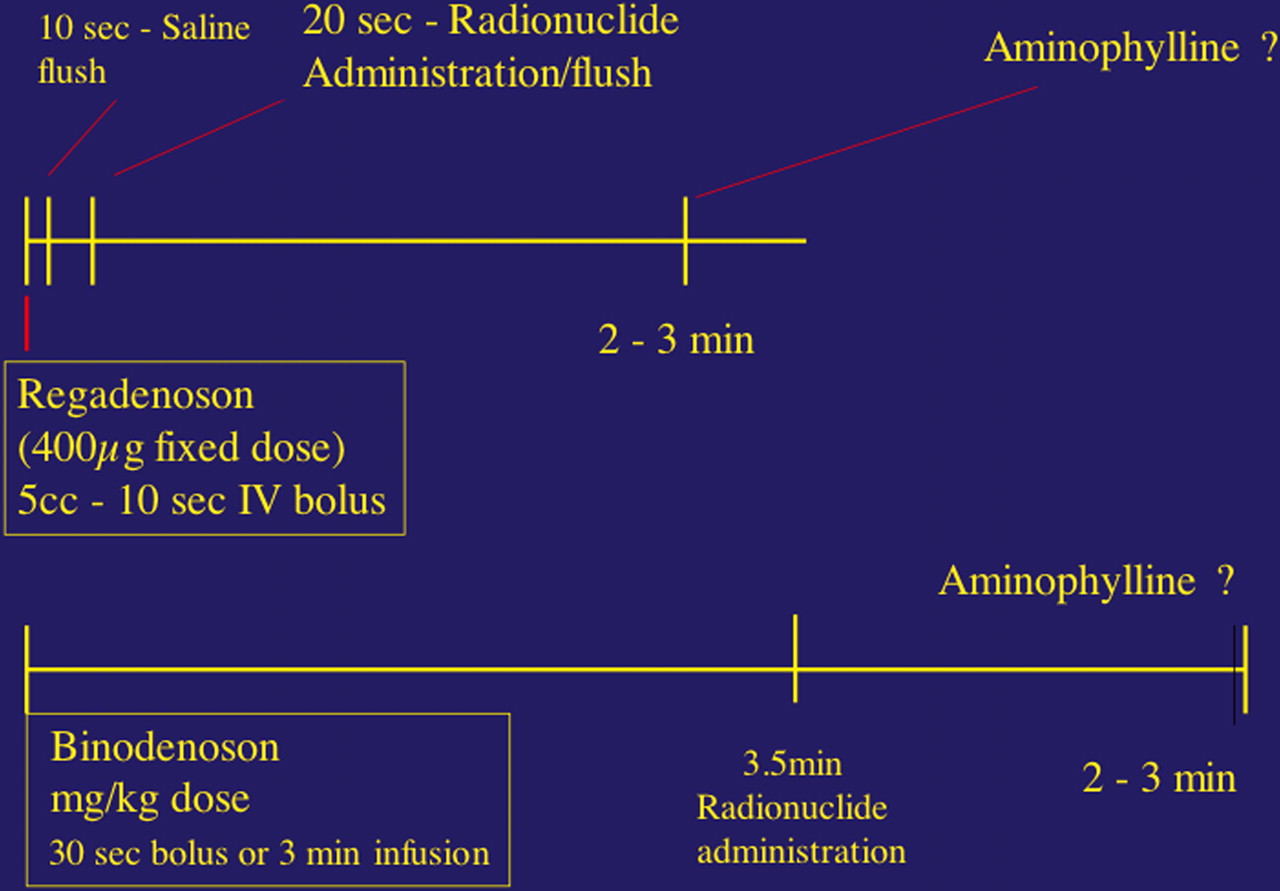
- FIGURE 4.
Shown diagrammatically are clinical infusion protocols recommended for regadenoson and binodenoson. These are designed on the basis of pharmacokinetics of the agents and their necessary interaction with the imaging agent.
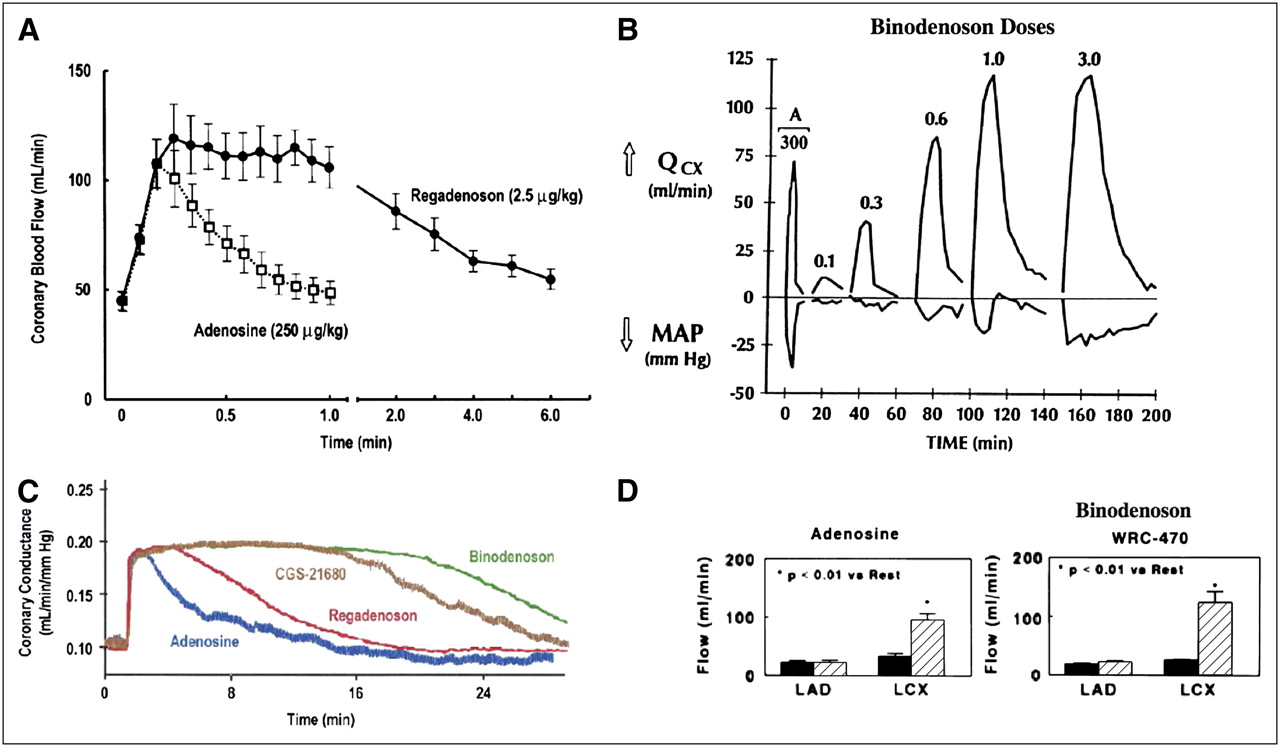
- FIGURE 5.
(A) Shown is time course of changes in coronary blood flow with regadenoson (solid curve) and adenosine (dashed curve). (Adapted with permission of (33).) (B) Shown above line for dogs are incremental changes in coronary flow (QCX) noted with serial increases in binodenoson dosage, compared with adenosine dosage. Decremental changes in mean arterial pressure (MAP) are plotted below line. (Adapted with permission of (34).) (C) Shown is time course of changes in coronary conductance, coronary blood flow normalized for perfusion pressure, with regadenoson (red curve), binodenoson (green curve), adenosine (blue curve), and CGS-21680, an unsuccessful dilator that has been withdrawn. (Adapted with permission of (31).) (D) Shown is increased coronary flow with adenosine (left) and binodenoson, WRC-470 (right) in a dog with tight stenosis of left anterior descending (LAD) coronary artery but without evident left circumflex (LCX) disease. Flow at baseline is shown in black, and flow with respective dilators is shown with hatched bar. Note blunted LAD response; LCX responds fully, given presence of flow-limiting agent. The binodenoson seems to bring same or higher flow response. (Adapted with permission of (34).)
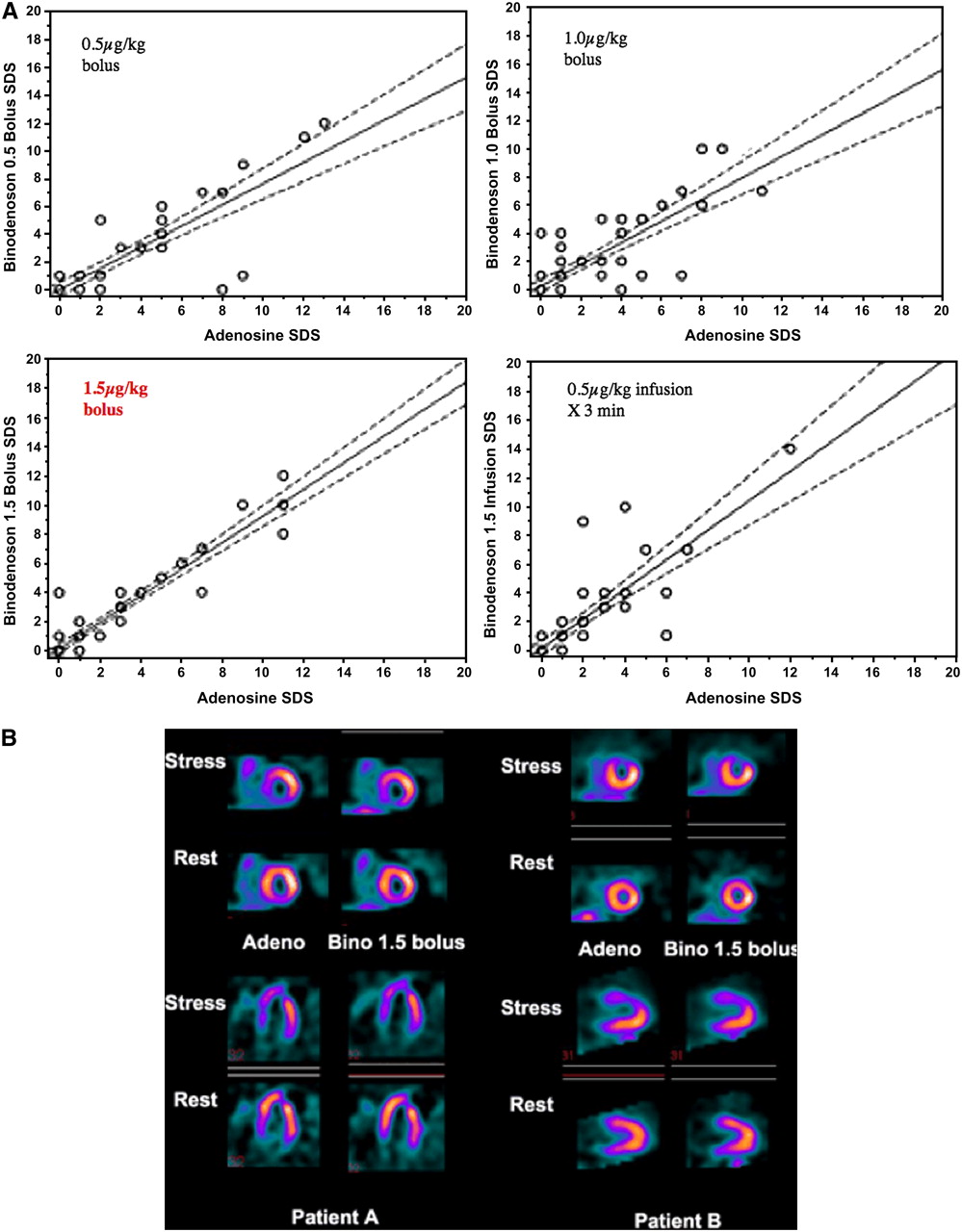
- FIGURE 6.
(A) Correlations with 4 dosing regimens. Summed defect scores (SDS) generated with adenosine correlated well with those using binodenoson in a 1.5 μg/kg bolus dosage. (B) Shown are rest and stress adenosine and binodenoson perfusion images in 2 case examples (patients A and B). Agreement is apparent. (Adapted with permission of (30).)
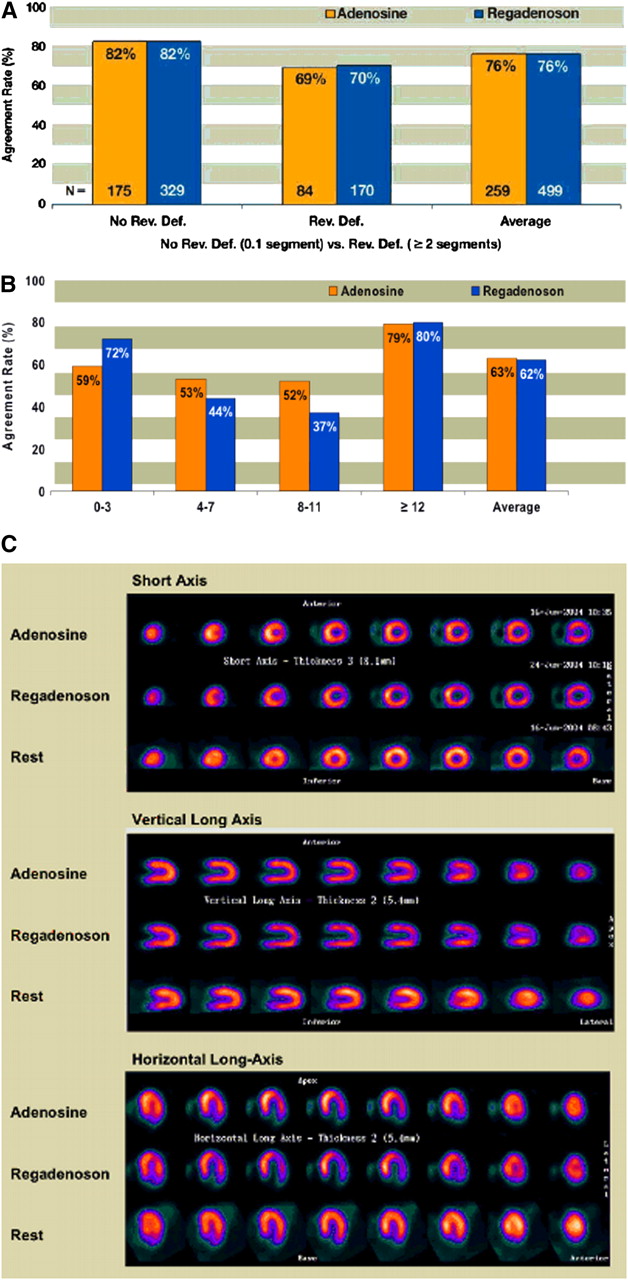
- FIGURE 7.
(A) Shown are agreement rates between adenosine–adenosine images (orange bars) and regadenoson–adenosine images (blue bars) based on presence or absence of reversible defects. Equality between these comparisons is evident. (B) Shown are agreement rates between adenosine–adenosine images (orange bars) and regadenoson–adenosine images (blue bars) by SSS, the summed stress score, based on a 17-segment model. Again, equality is evident. (C) Shown are SPECT images obtained with adenosine (top), with regadenoson (middle), and at rest (bottom) in 3 orthogonal views. Lateral reversible defect is seen on both sets of images and is more prominent with regadenoson. Rev. Def. = reversible defect. (Adapted with permission of (35).)



Tables
Perfusion Wall motion Initial event in the ischemic cascade Follows induced perfusion abnormality Does not require ischemia Requires ischemia Specific indicator of ischemia or ischemic potential Nonspecific indicator of ischemia Not significantly affected by loading conditions Affected by loading conditions Not significantly affected by resting wall motion abnormalities Affected by resting wall motion abnormalities Not generally affected by conduction abnormalities Affected by conduction abnormalities Adapted from (3).
Direct tests of CFR (vasodilator stress agents) Indirect tests of CFR (exercise/dobutamine) Seek to provoke flow heterogeneity Seek to provoke ischemia (perfusion or wall motion abnormality) Best suited for perfusion endpoint Fits either perfusion or function ischemic endpoint (must be used with wall motion endpoint) Less likely influenced by antianginal drugs Vary in ability to augment flow demands and test CFR Strongest, most reproducible, tests of CFR Permit serial function analysis Adapted from (3).
- TABLE 3
Physical, Chemical, and Clinical Characteristics of Current Pharmacologic Stress Agents
Agent Characteristic Dipyridamole Adenosine Dobutamine Source Synthetic Natural Synthetic FDA approved for stress testing Yes Yes No Mechanism Tests CFR Tests CFR True ischemic stress Action on CFR Indirect Direct Indirect Preparation Simple Simple Complicated (requires trained nurse) Dosage mg/kg mg/kg mg/kg Infusion Timed pump (may be hand titrated) Timed/isolated intravenous source Pump titration (requires trained nurse) Agent duration (half-life) Prolonged (∼90 min) Very short (12 s) Short (2.4 min) Intravenous line fails during infusion Problematic Redo Problematic Variable infusion rate Tolerable Intolerable Intolerable Stress-test duration ∼10–12 min ∼4–8 min ∼20–30 min Supervision and quality control Modest High High Patient tolerance High High Moderate Complications/side effects Bronchospasm/heart block Bronchospasm/heart block Ischemia/arrhythmia hypotension Symptom duration Usually brief Brief May be prolonged Safety Like exercise test Like exercise test Less than exercise test (only apply to selected patients) Safety with baseline dipyridamole Preserved Reduced Preserved Antidote Aminophylline Discontinue β-blocker Speed of reversal Minutes Seconds Minutes Diagnostic indicator Perfusion Perfusion Perfusion/wall motion Prognostic value High High Modest Sensitivity with caffeine Reduced Reduced Unchanged Sensitivity with β-blocker Reduced? Reduced? Reduced Prognosis with β-blocker Enhanced? Enhanced? Reduced Adapted from (3).
Selective A2A Agonists Characteristics CGS21680 (X) MRE-0470 Binodenoson ATL-146e (X) CVT-3146 Regadenoson Selectivity Low High Very high Moderate Affinity High High High Moderate Potency Moderate High Very high Moderate Stable Yes Yes Yes Yes Onset 1–2 min 1–2 min 1–2 min <1 min Duration >20 min 6–12 min 10–20 min 3 min Trials — 2 (phase III) 1 in 2003 2 FDA approved — To be submitted — YES Adapted with permission of (28).
Symptom Adenosine (n = 267) Regadenoson (n = 517) P (Fisher exact test) Any event 210 (79) 409 (79) 0.93 Any severe event 18 (7) 25 (5) 0.32 Flushing 63 (24) 86 (17) 0.02 Dyspnea 49 (18) 128 (25) 0.05 Headache 42 (16) 148 (29) <0.001 Chest discomfort 42 (16) 57 (11) 0.07 Chest pain 34 (13) 41 (8) 0.04 Angina pectoris 22 (8) 40 (8) 0.78 Feeling hot 17 (6) 19 (4) 0.10 Nausea 12 (4) 29 (6) 0.61 Dizziness 9 (3) 35 (7) 0.05 Abdominal discomfort 5 (2) 32 (6) <0.01 Data are presented as number of patients, with percentage in parentheses. Medical Dictionary for Regulatory Activities–preferred terms reported by 5% of patients or more in either treatment at any time after start of infusion are shown. Symptoms did not vanish with regadenoson and, in fact, differed little in their frequency, compared with those related to adenosine administration. This similarity may be related, in part, to the methods applied to determine the presence of symptoms. Adapted with permission of (35).
Question Tolerance level Adenosine Regadenoson P (Cochran-Mantel-Haenszel test) How did you feel? <0.001 Comfortable 1 85 (32) 200 (39) Slightly uncomfortable 2 133 (50) 271 (52) Very uncomfortable 3 38 (14) 39 (8) Extremely uncomfortable 4 11 (4) 7 (1) Mean ± SE 1.9 ± 0.05 1.7 ± 0.03 How did this test compare with the first (open-label adenosine) test? <0.001 Much better 1 41 (15) 177 (34) Somewhat better 2 74 (28) 129 (24) About the same 3 108 (40) 126 (24) Somewhat worse 4 30 (11) 74 (14) Much worse 5 14 (5) 11 (2) Mean ± SE 2.6 ± 0.06 2.3 ± 0.05 Data are presented as number of patients, with percentage in parentheses, unless otherwise indicated. When symptoms were considered for their tolerability, regadenoson showed a clear advantage. Adapted with permission of (35).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}