


Abstract
The use of 51Cr-labeled red blood cells to determine erythrocyte survival in circulation is not a routine procedure. Data are acquired by frequent counting of small-volume blood samples to determine the rate of red cell survival over time. Results are entirely quantitative and can involve semilogarithmic graphing techniques. An accurate study can positively identify hemolytic anemia, a disorder characterized by premature destruction of erythrocytes. Additionally, anatomic sites of premature hemolysis will demonstrate a higher radioactive count than the background organ. This procedure review presents a dual survival and sequestration study positive for hemolytic anemia and hypersplenism in an 83-y-old man with systemic lupus erythematosus. 51Cr red cell survival and splenic sequestration studies may be considered when clinical history and laboratory studies cannot establish a definitive diagnosis.
Studies of 51Cr red cell survival and splenic sequestration are rarely performed (1) and have remained virtually absent from medical literature published within the past few decades. Despite the infrequency of the studies and the lack of acquired images for qualitative interpretation, the procedure can be important for particular indications. The dual study offers quantitative results that can positively identify hemolytic anemia, a condition in which circulating erythrocytes are prematurely destroyed (2). Although a complete blood count is routinely performed to assess anemic conditions, the 51Cr red cell survival study with sequestration has the added benefit of determining whether the liver or spleen is the site of premature erythrocyte destruction (3). In this way, the type of anemia can specifically be identified as hemolytic. Other methods for evaluating hemolytic anemia include the direct antiglobulin test and the glucose-6-phosphate dehydrogenase enzyme screen, but these methods are not definitive for hemolysis (4). The 51Cr red cell survival study can be valuable in establishing a diagnosis of hemolytic anemia when clinical history and laboratory studies cannot. This article presents the case of an 83-y-old man with systemic lupus erythematosus who demonstrated positive results for hemolytic anemia and hypersplenism during a study of 51Cr-labeled erythrocyte survival and sequestration.
CASE EXAMPLE
An 83-y-old man with systemic lupus erythematosus was admitted to the hospital with a hip fracture. The patient presented with pallor of the skin and nail beds, shortness of breath, and tachycardia exceeding 140 beats per minute.
Routine blood and serum tests revealed low hematocrit and hemoglobin values and a low number of circulating platelets. Abdominal ultrasound was performed and the spleen was significantly enlarged. Simultaneous 51Cr red cell survival and splenic sequestration studies were ordered to rule out premature hemolysis as a cause for the patient's anemia.
An initial volume of 30 mL of blood was collected from the patient with an anticoagulant. The sample was labeled with 4.07 MBq (110 μCi) of 51Cr-sodium chromate and incubated at room temperature for 60 min. Afterward, approximately 50 mg of ascorbic acid were added to the solution to prevent further tagging of the red blood cells. The total volume was administered intravenously to the patient, who returned 24 h later for the first blood sample collection. On the same day as the collection of blood samples, an uptake probe was used to acquire 10-min counts over specified anatomic locations including the heart, liver, and spleen. Indelible ink was used to mark these areas so consistent geometry in counting would be maintained throughout the study. The probe was placed directly on the skin of the marked areas for counting. The same protocol was followed for subsequent days, with the patient returning on the second, third, seventh, 10th, 13th, 15th, and 17th days for additional blood collection and external anatomic counting.
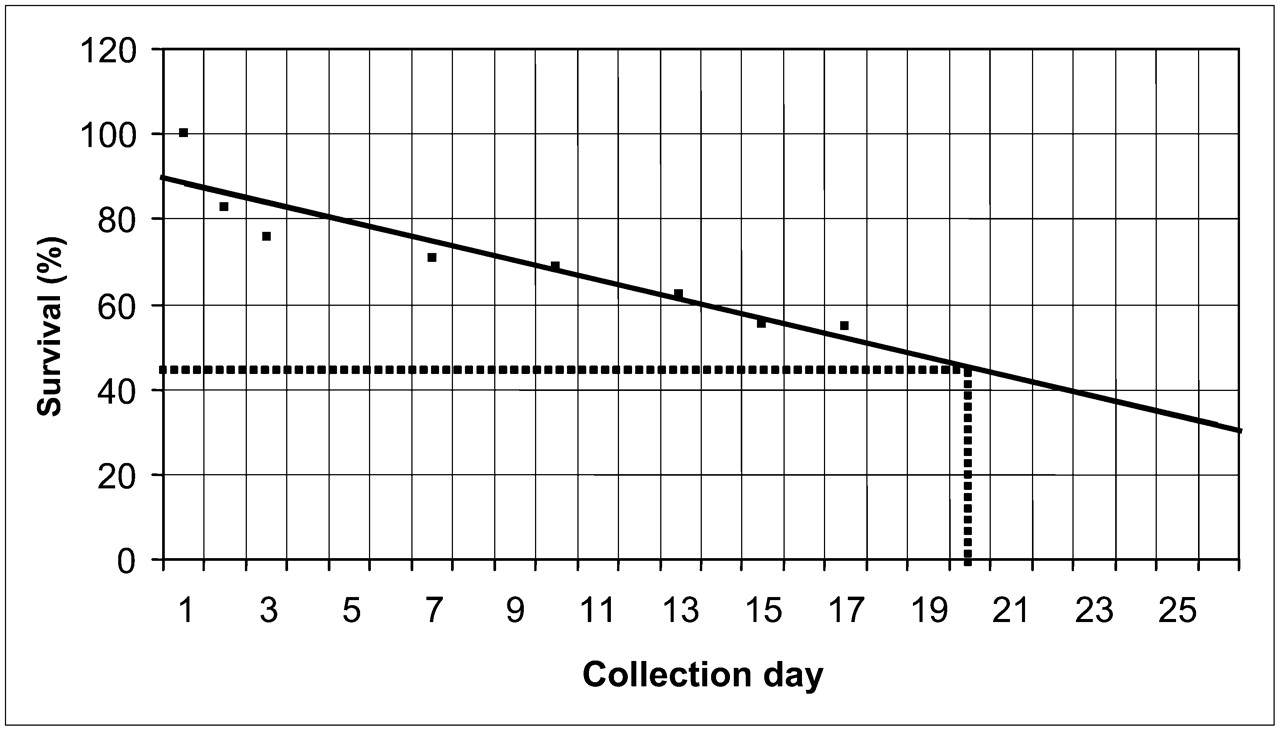
At the end of the collection period for the study of red cell survival, the samples were centrifuged and allotted into 5-mL portions. All the prepared whole-blood and plasma samples were counted for 10 min each using a scintillation well counter (Biodex Medical Systems) and multichannel counting system (Atomlab 450) with an energy window of 280–360 keV. Whole-blood and plasma counts per minute were recorded for each of the 8 d. Plasma counts were subtracted from whole-blood counts to calculate red blood cells in counts per minute (Table 1). After the samples had been collected and counted, the percentage of red blood cells surviving was calculated by dividing the red blood cells (cpm/mL) by the hematocrit and then expressing the result as a percentage based on day 1 (Table 2). The patient's hematocrit was monitored on each sample collection day to ensure that circulatory homeostasis was present. Changes in hematocrit values of greater than 2% during the study indicate that a steady state does not exist and could indicate an inaccurate study (5). The percentage of red cells surviving from Table 2 was plotted on linear graph paper (Fig. 1). Extrapolation techniques determined that the patient's half-time survival of red blood cells was approximately 20 d, whereas the normal half-time survival for 51Cr-labeled cells is between 25 and 35 d.

Red cell percentage survival graphed linearly for each collection day. Red cell survival half-life was extrapolated.
Red Cell Survival Data
Percentage of Red Blood Cells Surviving Each Day
Heart, liver, spleen, and background counts per minute from the scintillation uptake probe (Biodex Medical Systems) were recorded and decay corrected to represent the ongoing splenic sequestration study. The data for the splenic sequestration study revealed that the ratio of net spleen counts (corrected for heart counts) to net liver counts (also corrected for heart counts) was 3.5 to 1 (Table 3), which is higher than the expected normal value of 1 to 1 (6). Although the results did not significantly appear to be positive until days 15 and 17, the results were reported as positive.
Splenic Sequestration Probe Counts
The physician interpreted the results as premature destruction of red blood cells at the anatomic location of the spleen. The final report indicated that the onset of hemolytic anemia was most likely related to the patient's underlying chronic autoimmune disorder. The patient was subsequently referred for treatment with corticosteroids and possible splenectomy.
DISCUSSION
Hemolytic anemia arises from the more generalized group of blood disorders known as anemia, which is characterized by a deficiency in the number of circulating red blood cells or in the amount of hemoglobin produced by the cells. More specifically, hemolytic anemia is a condition in which red blood cells are prematurely destroyed, or hemolyzed. The bone marrow is unable to keep up with the rate of hemolysis, resulting in a reduced number of circulating erythrocytes. Hypoxia may develop as the red blood cells are unable to meet the body's oxygen requirements, and the clinical presentation of symptoms includes tachycardia, dyspnea, angina, fatigue, pale skin, and pale nails (7). Jaundice and splenomegaly may also occur, and these symptoms suggest underlying disorders such as chronic lymphocytic leukemia, some types of lymphomas, and systemic lupus erythematosus (8). There are reportedly more than 200 causes of hemolytic anemia, but for classification purposes the disorder is either hereditary (such as glucose-6-phosphate dehydrogenase deficiency or sickle cell anemia) or, as in the case of this patient, acquired because of immune disorders, toxic chemicals, toxic drugs, or systemic infections. Symptoms may go unnoticed for some time, but the anemia becomes severe when cardiovascular symptoms are experienced, possibly leading to cardiac failure and death if untreated. The most common screening tool for general anemia is a complete blood count, in which hematocrit and platelet values are below the normal range. Treatment of hemolytic anemia depends on the severity of the disorder and the underlying condition. Transfusion therapy, administration of corticosteroids, and splenectomy are the main treatments of autoimmune hemolytic anemia (9).
The study of 51Cr red blood cell survival was established more than 50 y ago as an indication for evaluating hemolytic conditions (10,11). In 1975, Giles et al. (12) analyzed 2 methods for labeling sheep erythrocytes and determined that 51Cr activity was rapidly eluted from circulation when compared with cohort 59Fe-labeling techniques. However, it has since been established that the random 51Cr tag is more convenient and less expensive than cohort labeling (13).
In addition to tracking a random sample of red blood cells to determine survival time in circulation, quantitative methods have been developed to evaluate splenic red blood cell destruction. Studies indicate that erythrocyte destruction takes place almost exclusively in the spleen, especially in those patients who demonstrate splenomegaly (14–16).
The results of the combined studies are entirely quantitative, so there are no images acquired. However, it is extremely important to maintain accuracy and consistency throughout the length of the study. The standard protocol suggests that the patient have blood drawn 3 d a week for at least 2–3 wk. However, this study was completed in 17 d. Collection of 2 additional blood draws would improve the statistical accuracy of this study and allow for a more definitive interpretation. In addition, replication of sample counting with 2 samples for each measurement ensures accuracy and should always be considered for in vivo data collection.
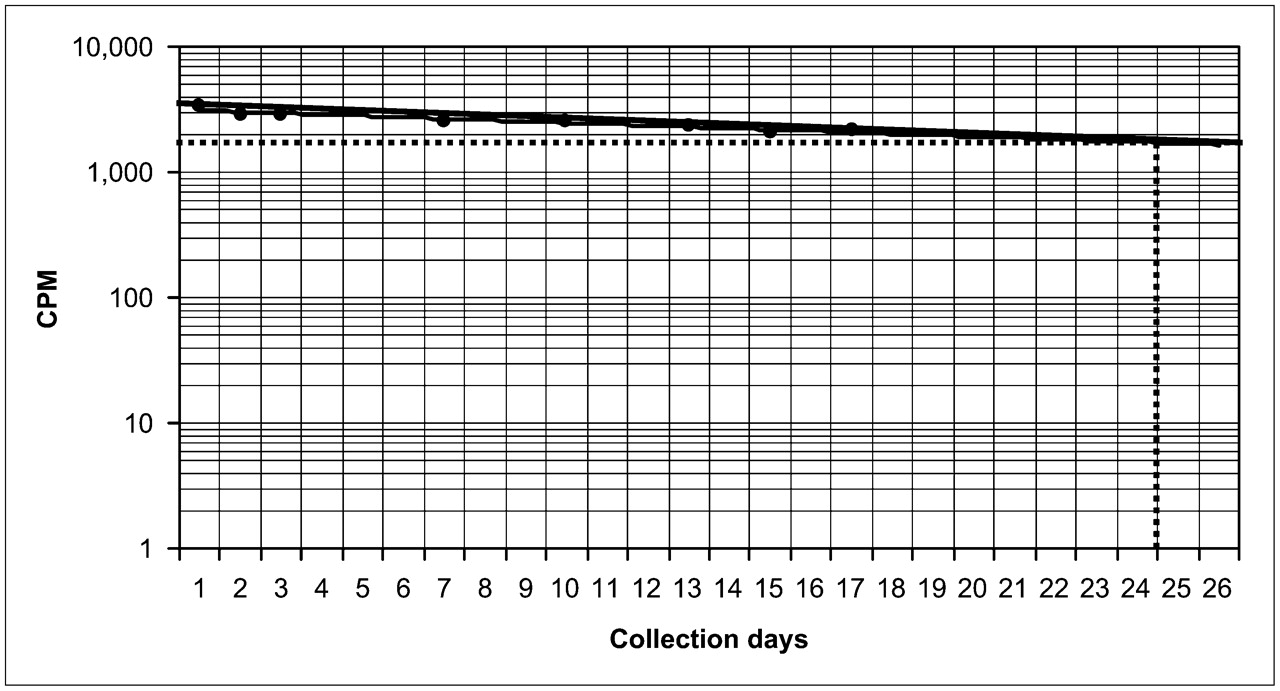
The data presented in this case were graphed linearly as the percentage of red cells surviving over a period of days. Extrapolation of the best-fit line between data points revealed a half-time survival of 20 d (Fig. 1), which is just below the average 51Cr half-time survival of 25–35 d. Some authors suggest graphing the net red blood cell counts on semilogarithmic paper as a function of time (17). For the purposes of this review, the patient's data were analyzed using the counts per minute. With this method, the half-time survival was found to be 24.5 d (Fig. 2), still just below the documented normal value. Use of this graphing technique for final interpretation may have altered the results. At this time, further research is needed to determine which method of graphing is more accurate.

Red cell counts per minute graphed for each day. Red cell survival half-life was extrapolated using best-fit line.
In the sequestration study, it is important to maintain consistent geometric parameters when taking counts over the heart, spleen, and liver. In this case, the patient was marked with indelible ink so the uptake probe could be placed in the same position on the patient's skin each day of the study. The numeric ratios reported in Table 3 indicate a positive result for hypersplenism (increased red cell destruction by the spleen). There are no obvious values to suggest inaccuracy for this study; all counts are similar throughout the 17-d study with the exception of the increased spleen counts.
The final ratio of spleen to liver counts (corrected for background) was 3.5 to 1, and a ratio of 4 to 1 is highly positive for hypersplenism (6).
CONCLUSION
Although this study is somewhat labor-intensive and inconvenient to perform, a dedicated technologist and cooperative patient may succeed in providing accurate results for interpretation. As one of the few definitive tests for hemolytic anemia, this study may be considered by physicians who suspect autoimmune or acquired hemolytic disorders, especially when blood and serum tests fail to provide a definitive diagnosis.
Acknowledgments
We acknowledge Patrick Molloy, CNMT, for his technical and professional assistance in preparing case materials.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 14, 2007.
- Accepted for publication January 26, 2008.





{kind=link}
{kind=link}