


Article Figures & Data
Figures
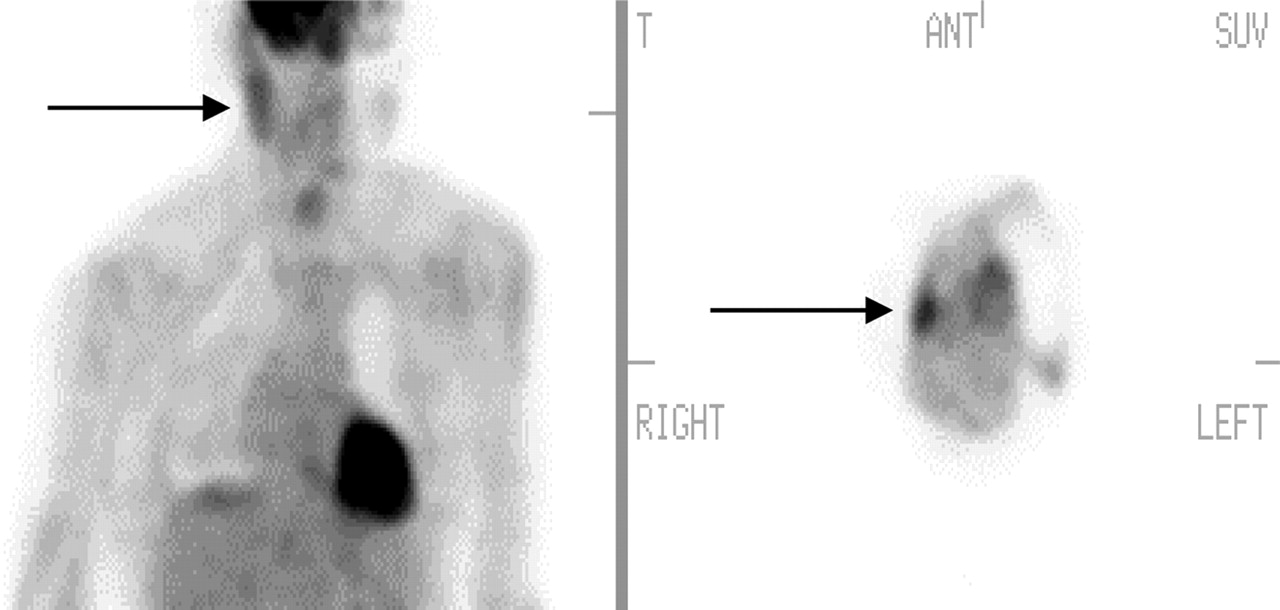
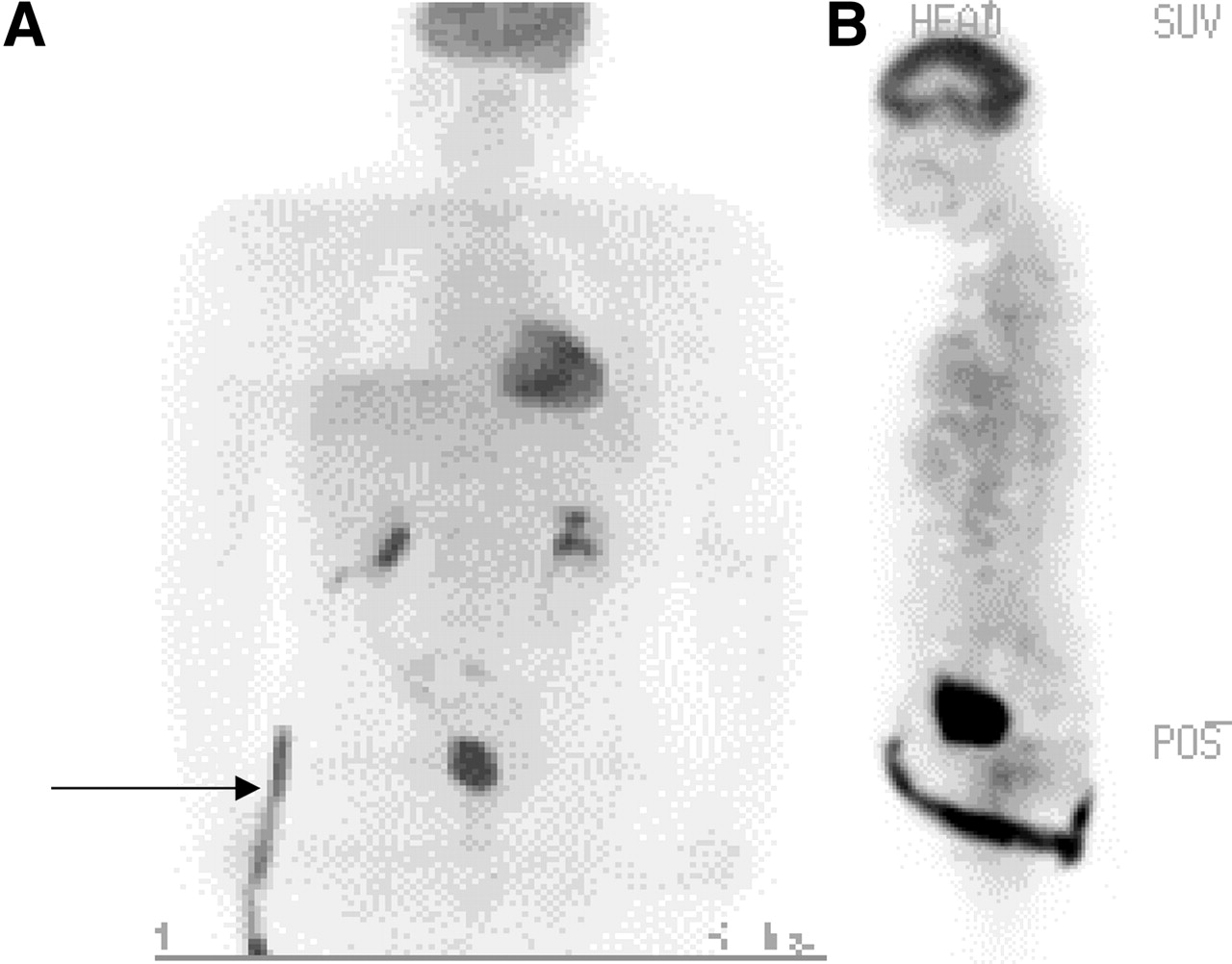
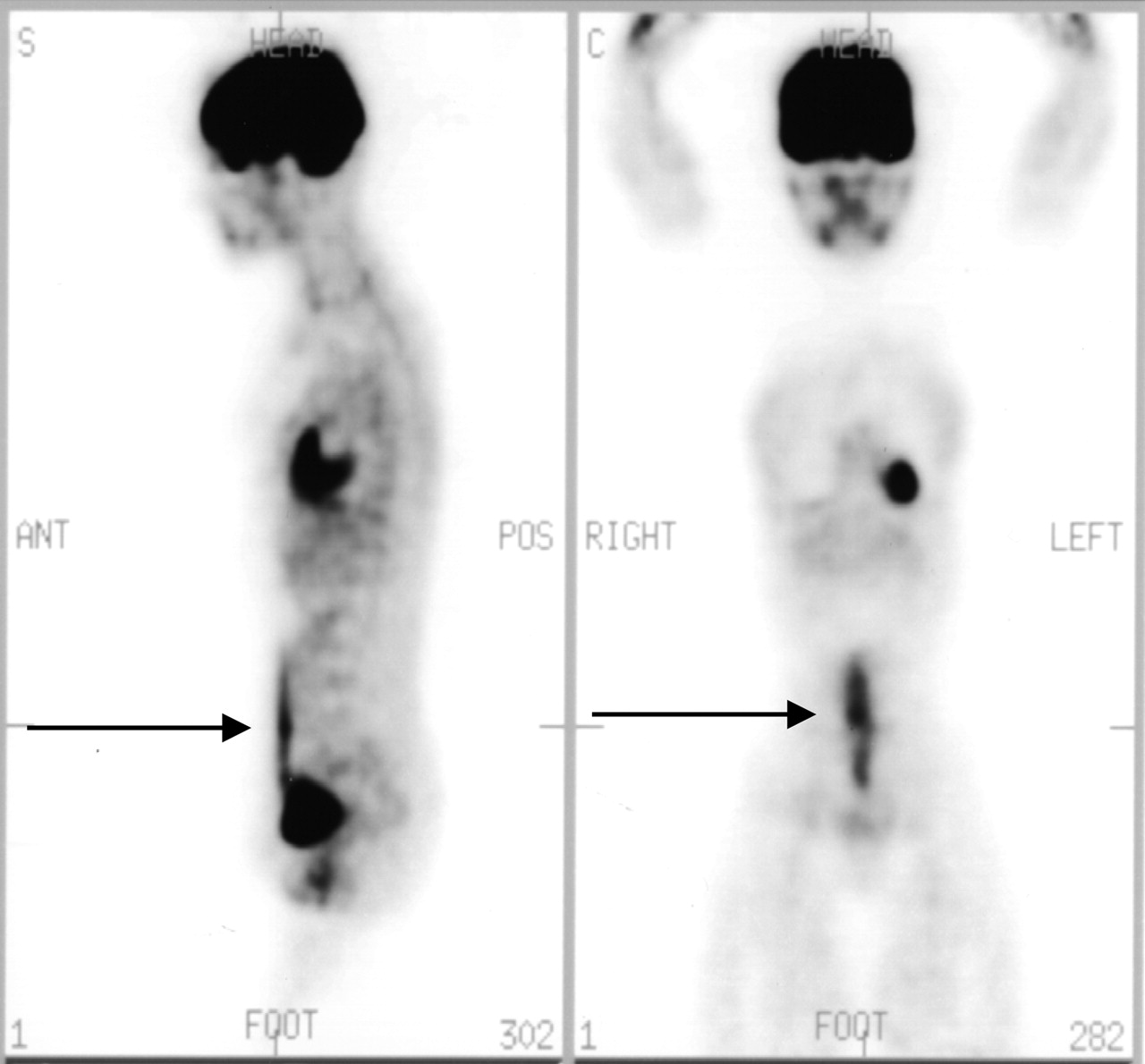
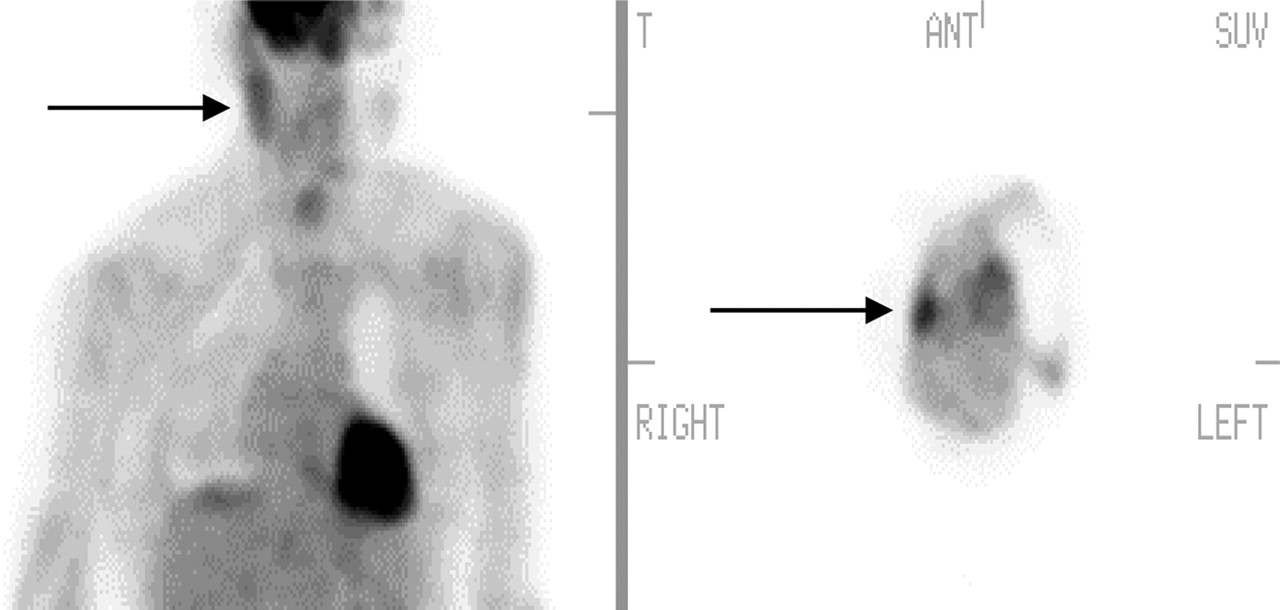
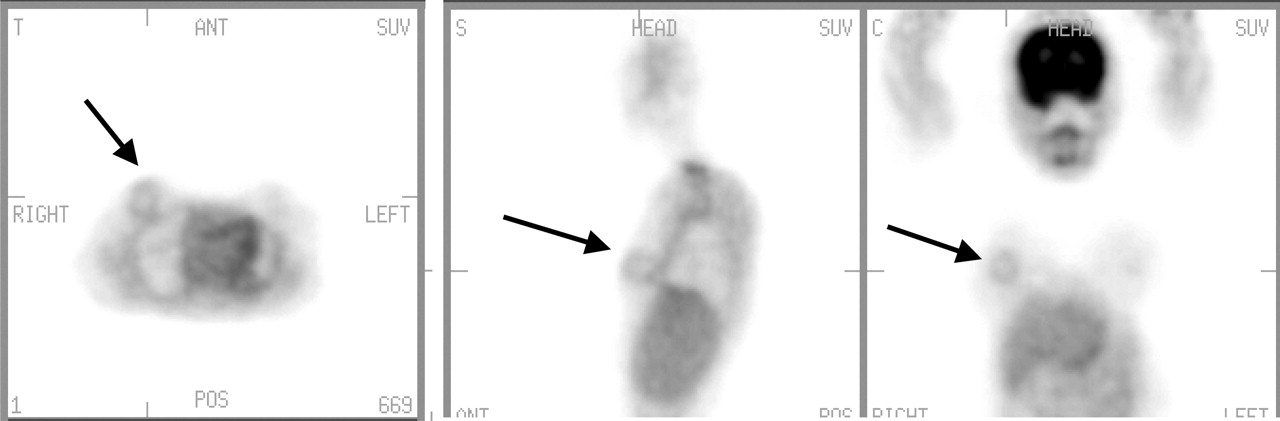
- FIGURE 1.
Asymmetric salivary gland uptake (projection view). Note increased 18F-FDG uptake in right face/salivary gland and region (arrow) as compared with contralateral side. Patient’s head moved during acquisition. SUV = standardized uptake value.
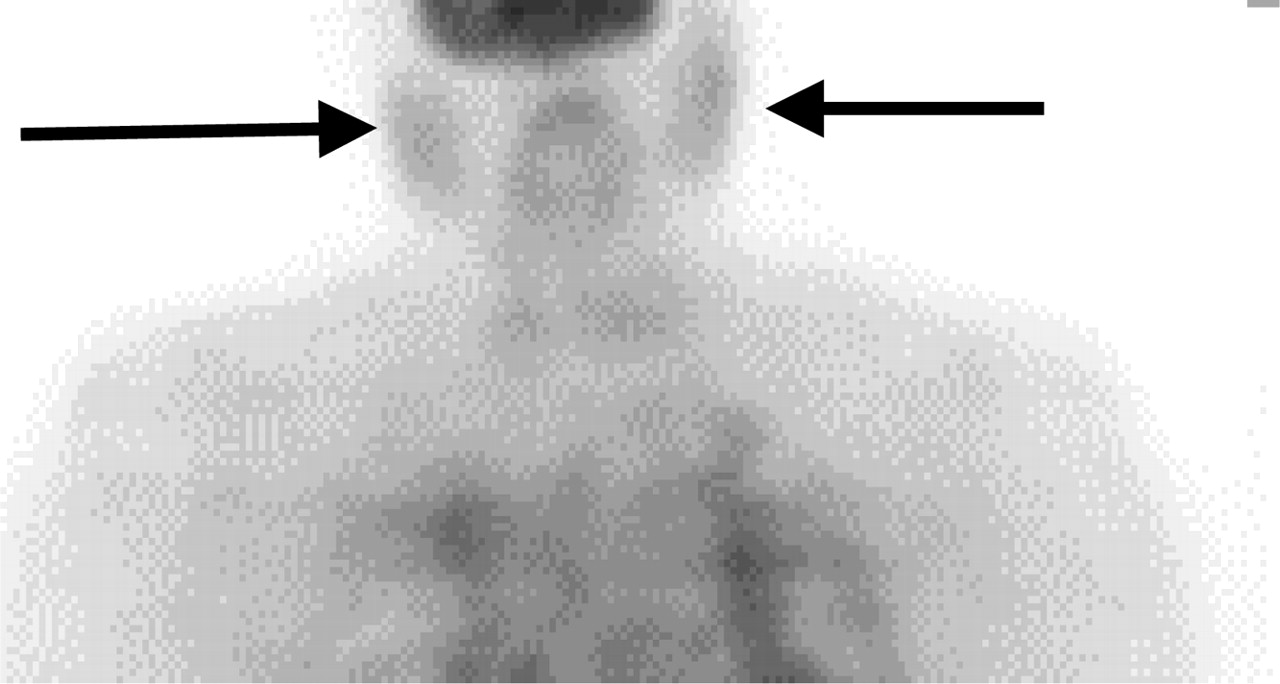
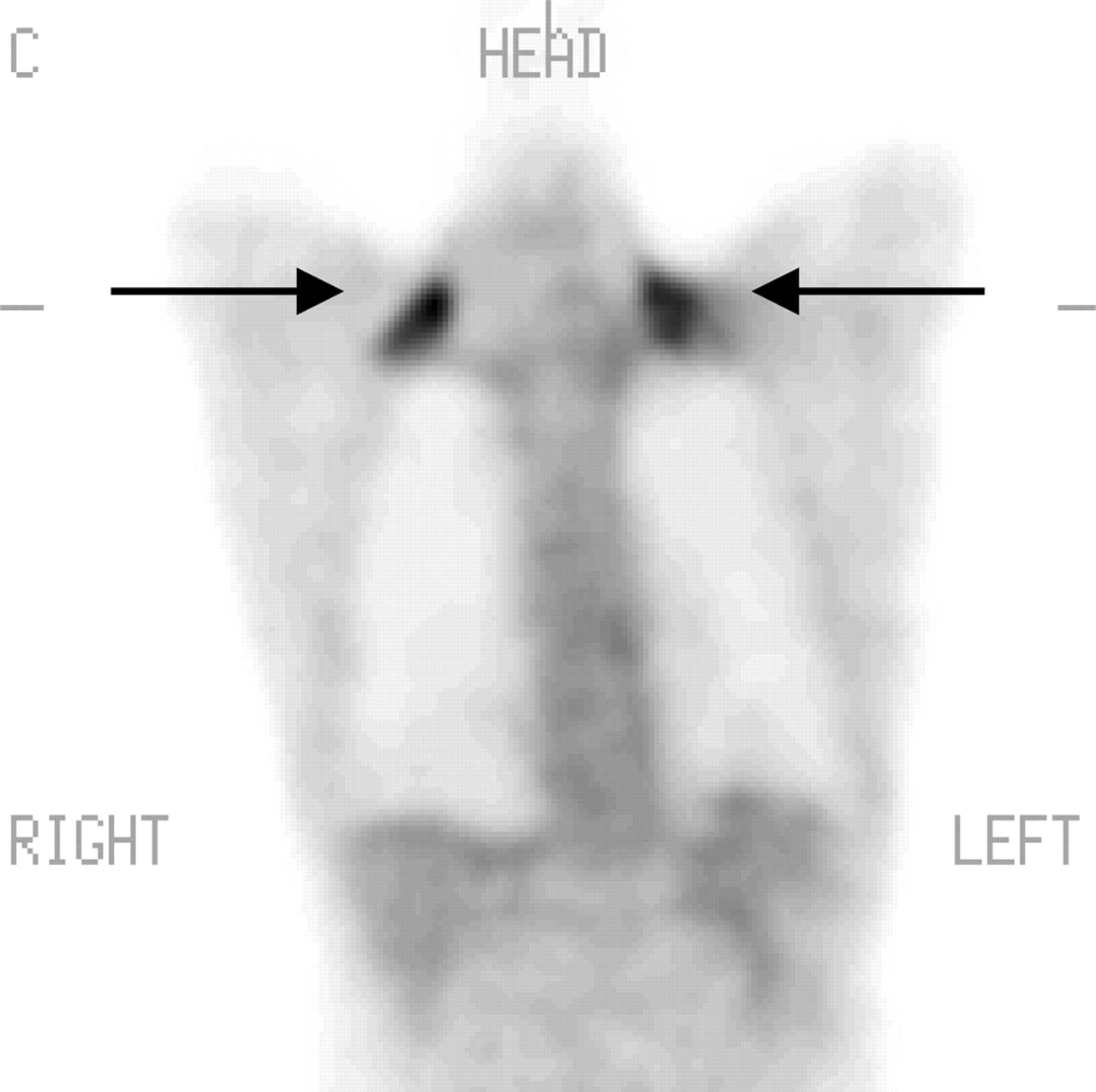
- FIGURE 2.
Symmetric salivary gland uptake (projection view; arrows) shows mild uptake.
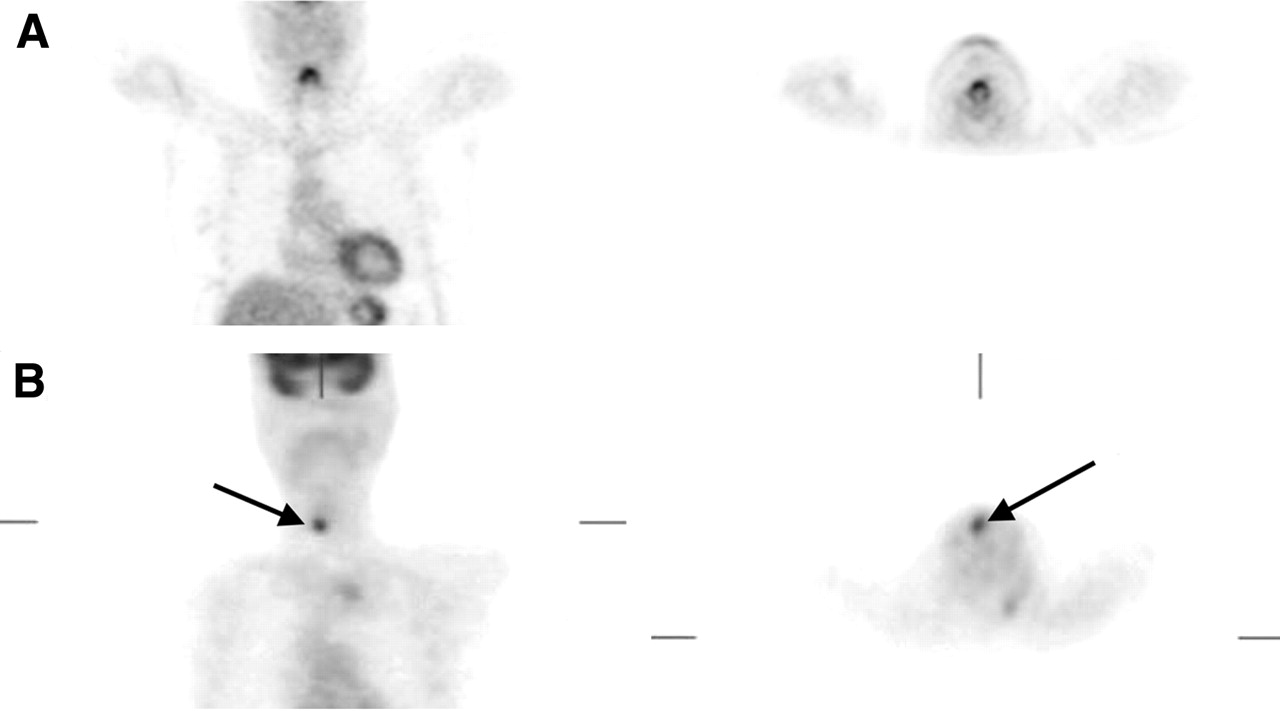
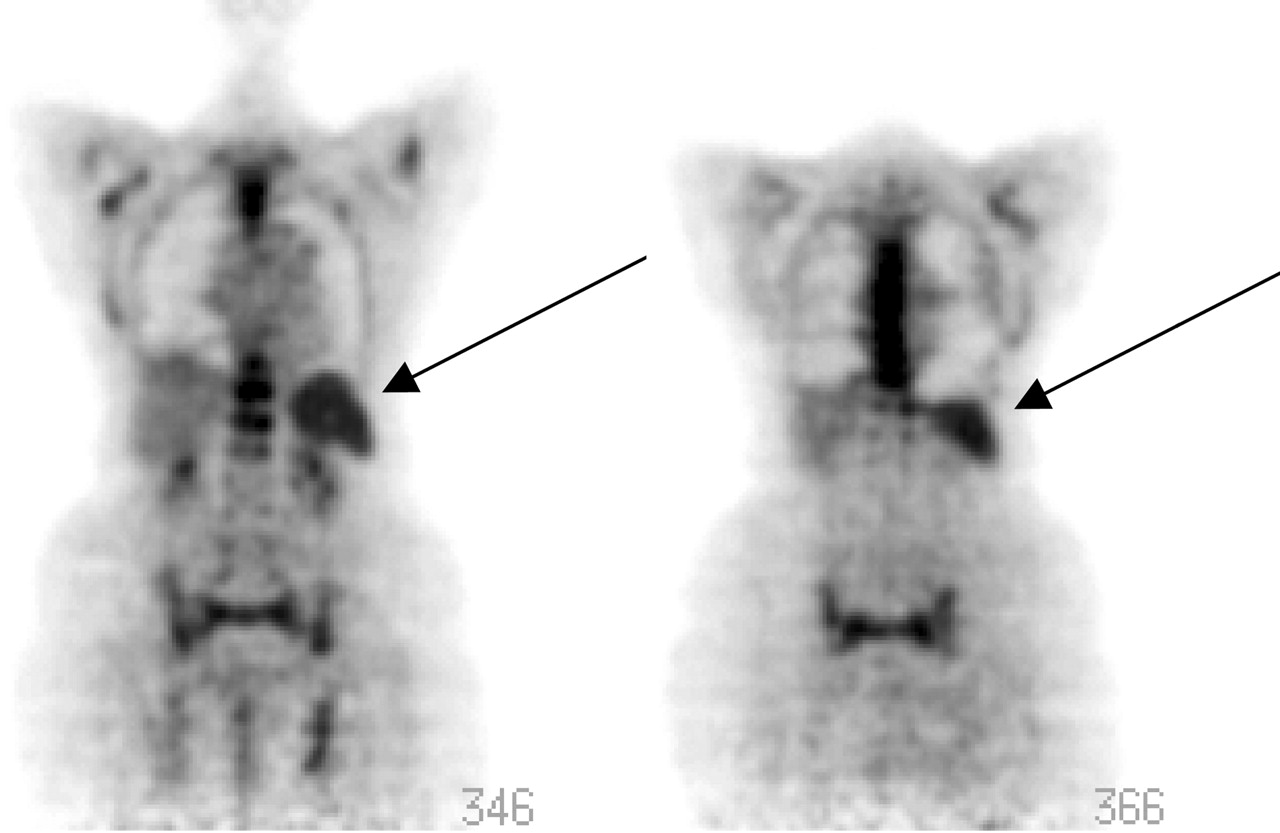
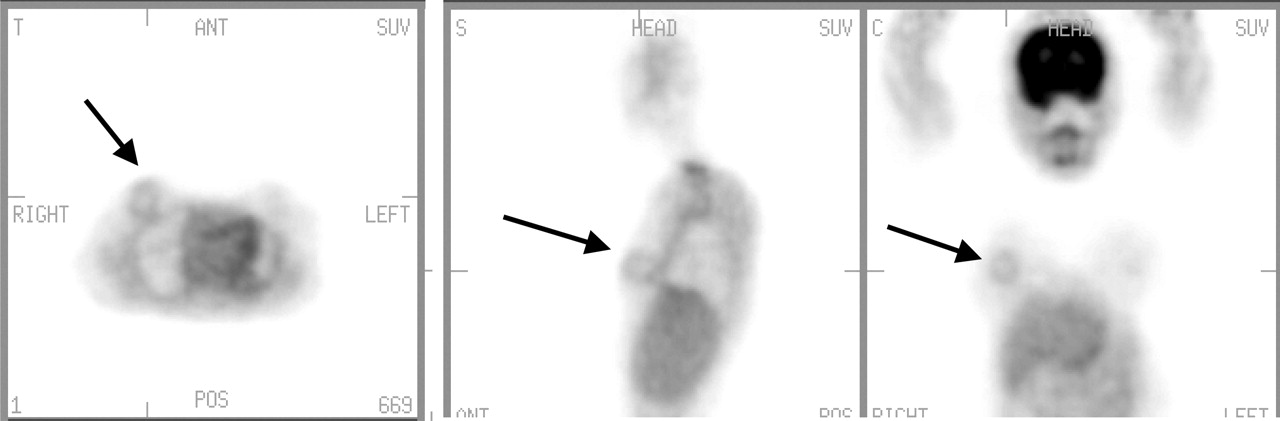
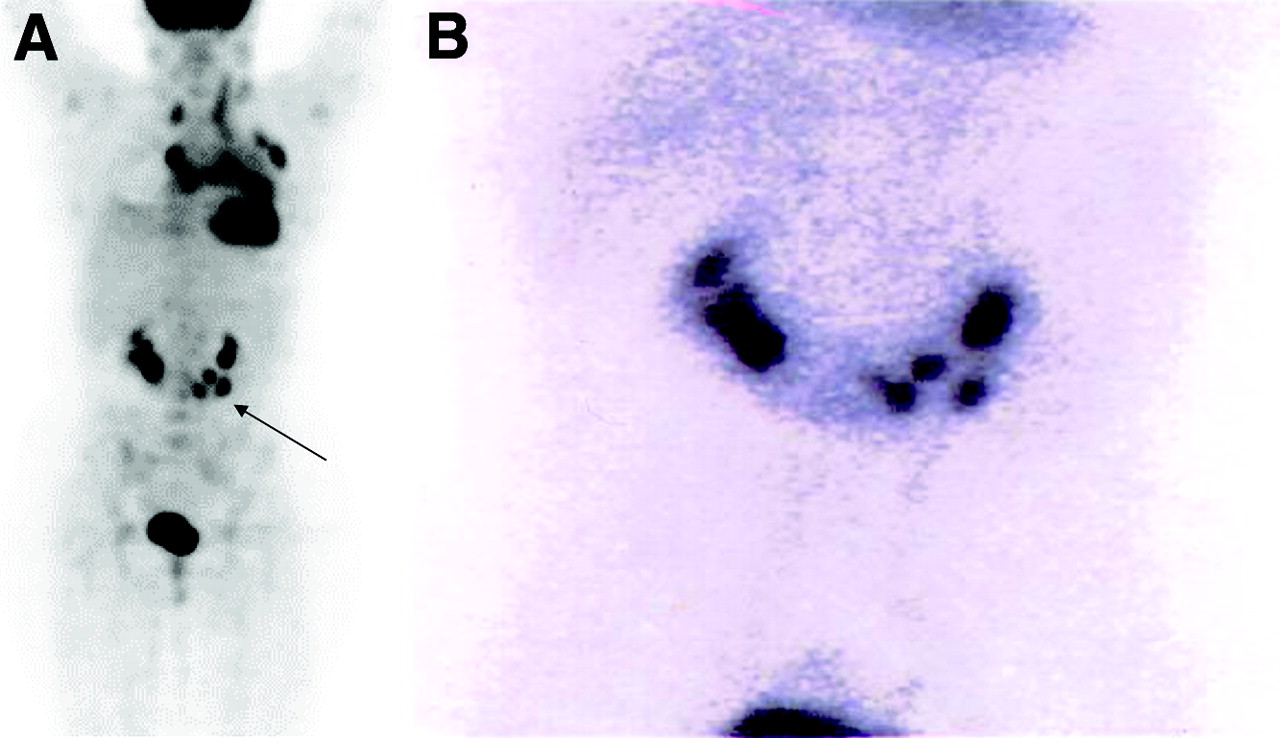
- FIGURE 3.
Laryngeal uptake. (A) Normal symmetric uptake in larynx. (B) Focal unilateral (arrows). Coronal view on left; transaxial view on right.
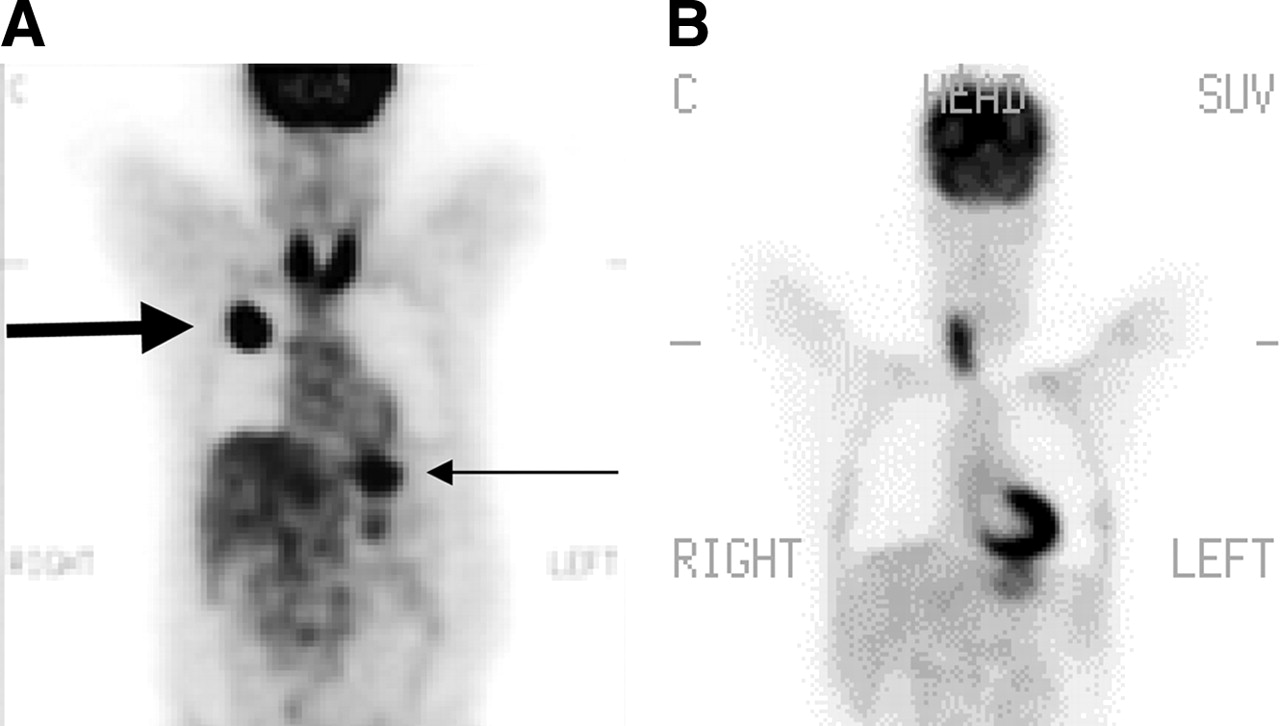
- FIGURE 4.
Thyroid inflammation. (A) Patient with known squamous cell carcinoma of upper lobe of right lung (thick arrow) who was being evaluated for initial staging. Note intense thyroid uptake due to Hashimoto’s thyroiditis. Also note normal stomach uptake (thin arrow). (B) A 57-y-old woman with history of breast carcinoma and left thyroidectomy who was being evaluated because of rising levels of tumor markers. Neck uptake was due to Hashimoto’s thyroiditis, which could easily have been mistaken for nodal uptake. C = coronal.
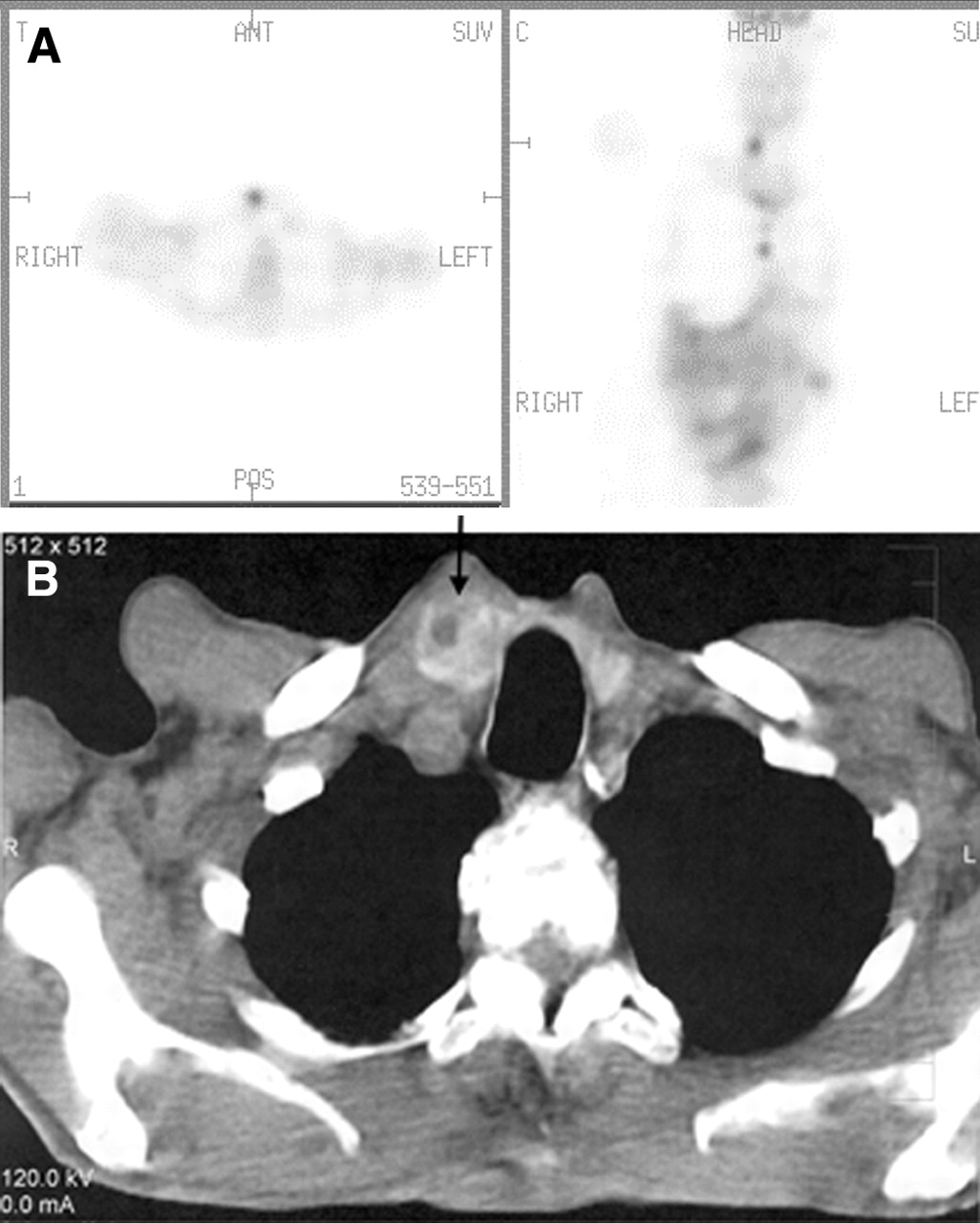
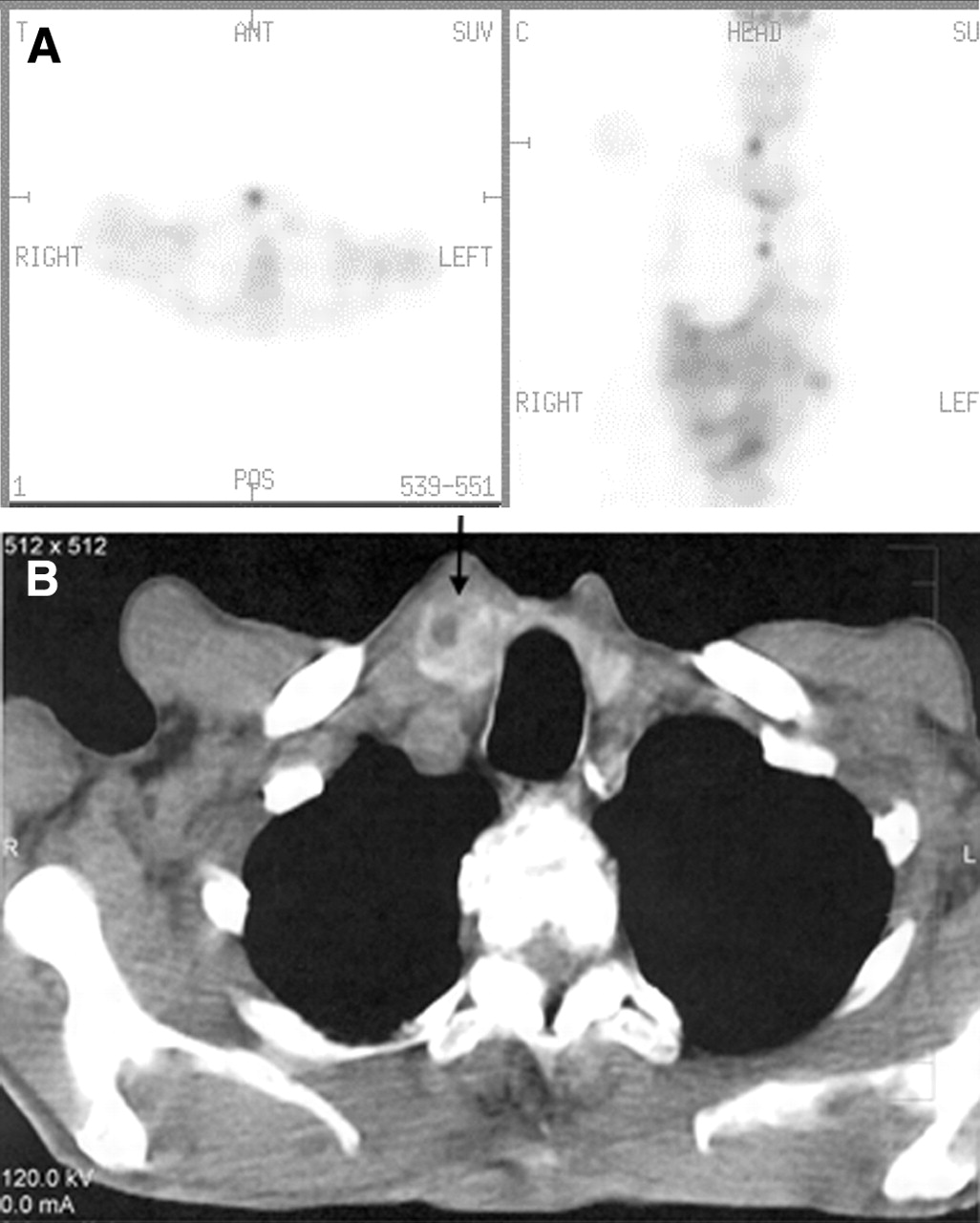
- FIGURE 5.
Focal thyroid uptake. (A) Focal thyroid uptake seen in right lobe of thyroid gland corresponding to focal density (arrow) seen on CT scan (B). ANT = anterior; POS = posterior; C = coronal.
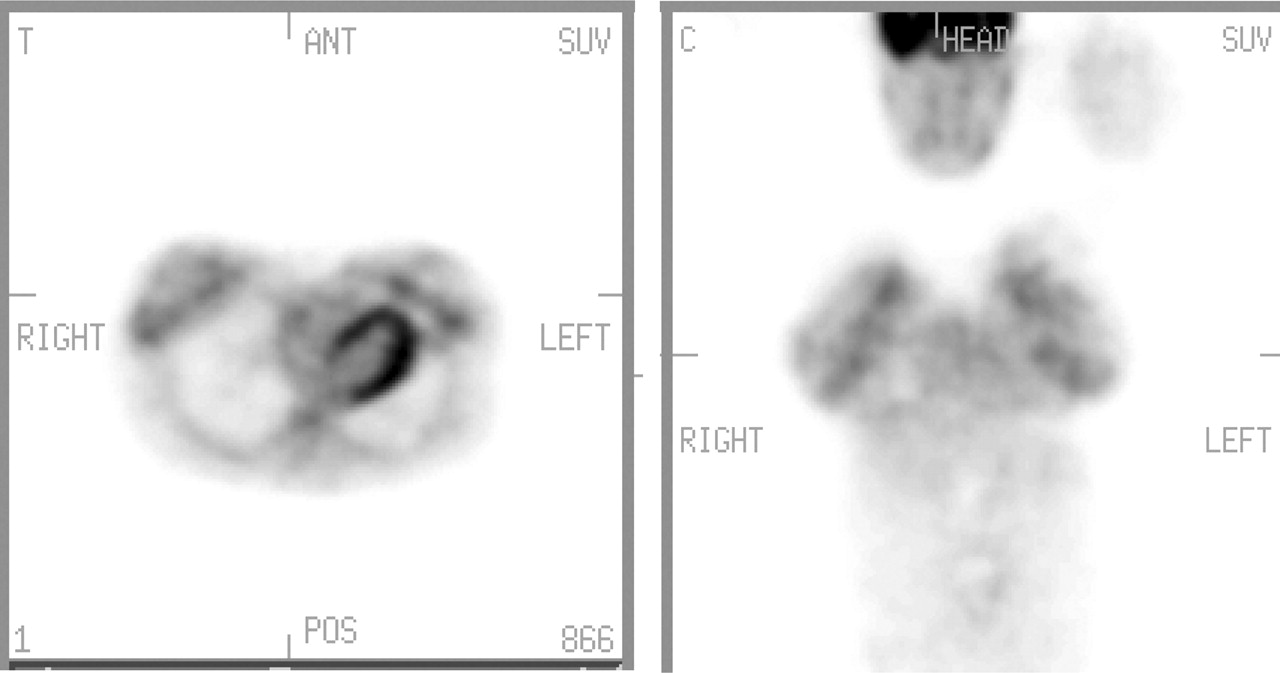
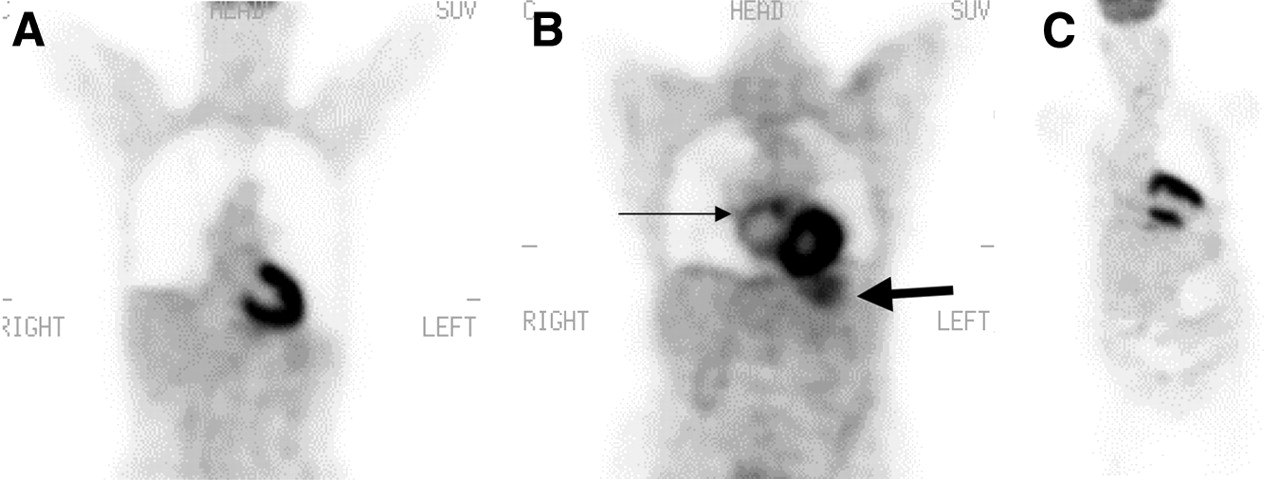
- FIGURE 6.
(A) Cardiac uptake: Normal physiologic intense 18F-FDG uptake throughout myocardium. (B) Atrial uptake: Note inhomogeneous mild 18F-FDG uptake in enlarged right atrium resembling abnormal mediastinal nodal tissue uptake. Thick arrow points out normal stomach uptake. (C) Cardiac uptake: Apical scar with aneurismal formation.
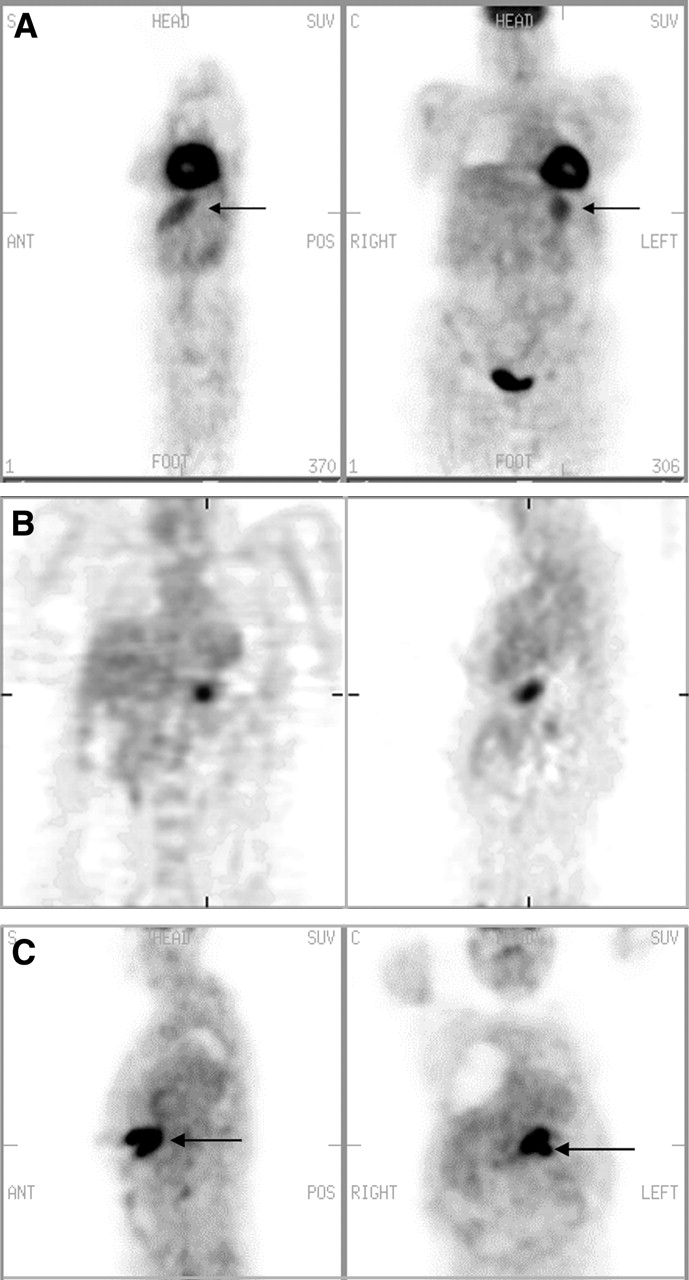
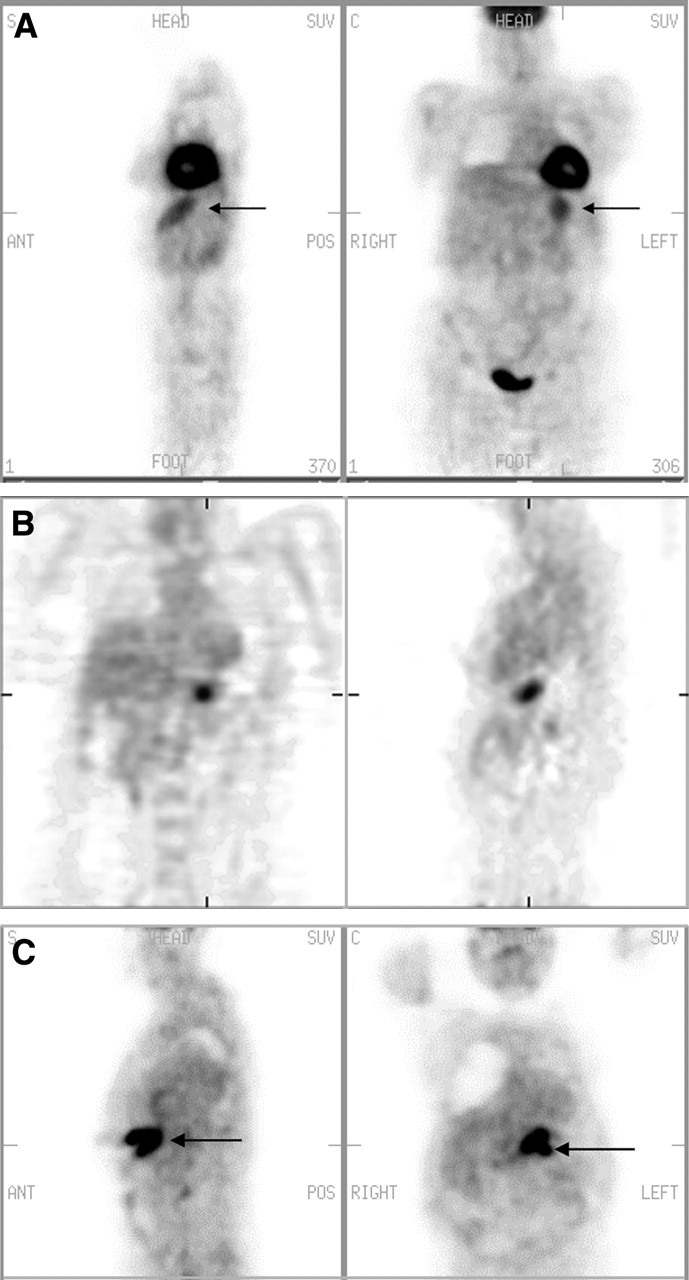
- FIGURE 7.
Stomach uptake. (A) Normal uptake: mild diffuse uptake (arrows) conforming to stomach configuration. (B) Adenocarcinoma of stomach: focal uptake in region of stomach. Coronal view on left; sagittal view on right. (C) Stomach lymphoma: intense focal uptake (arrows). S = sagittal; C = coronal; ANT = anterior; POS = posterior.
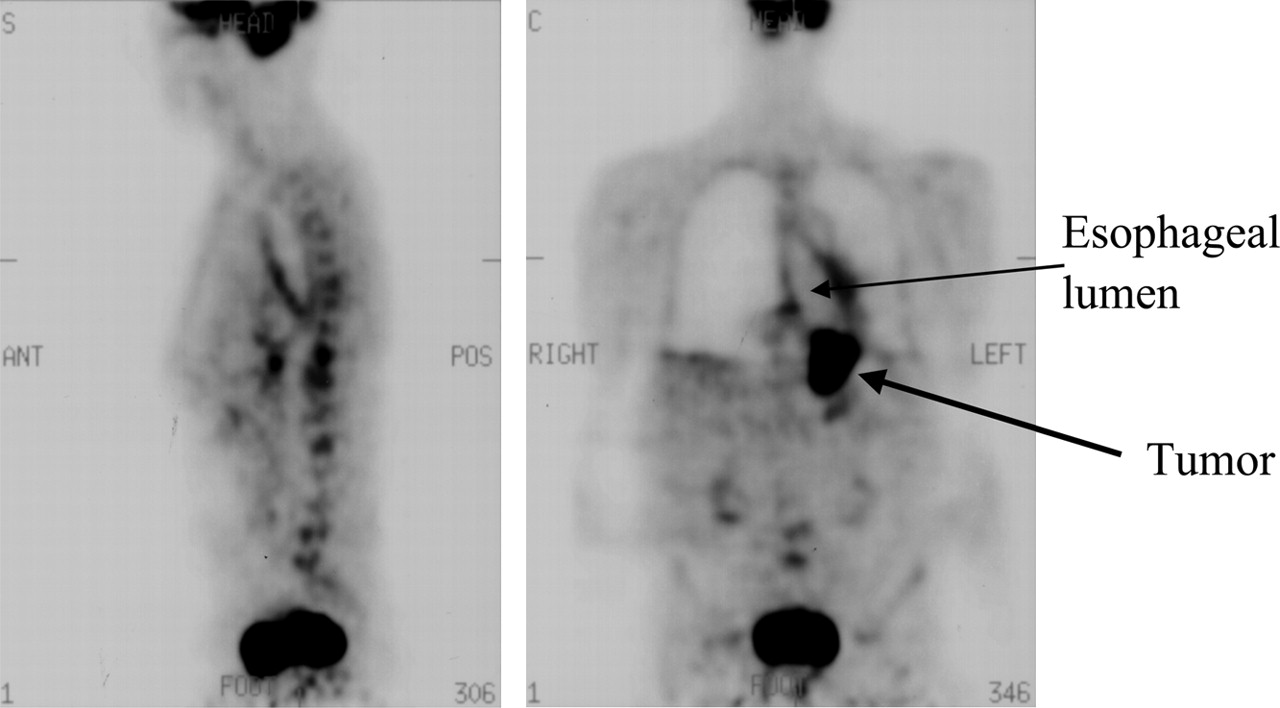
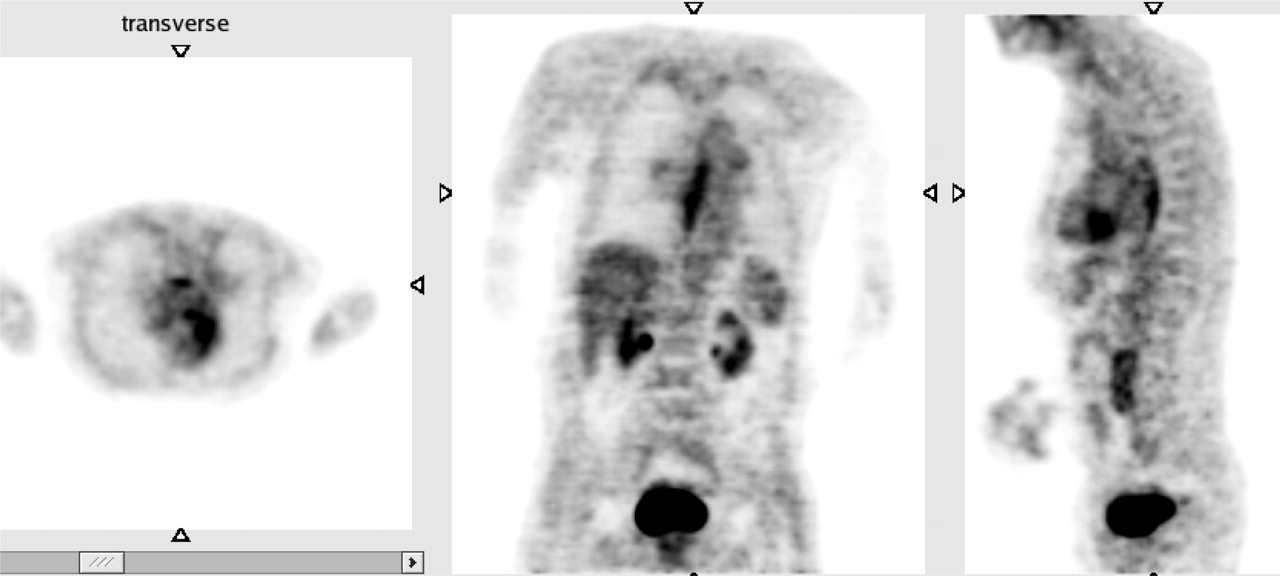
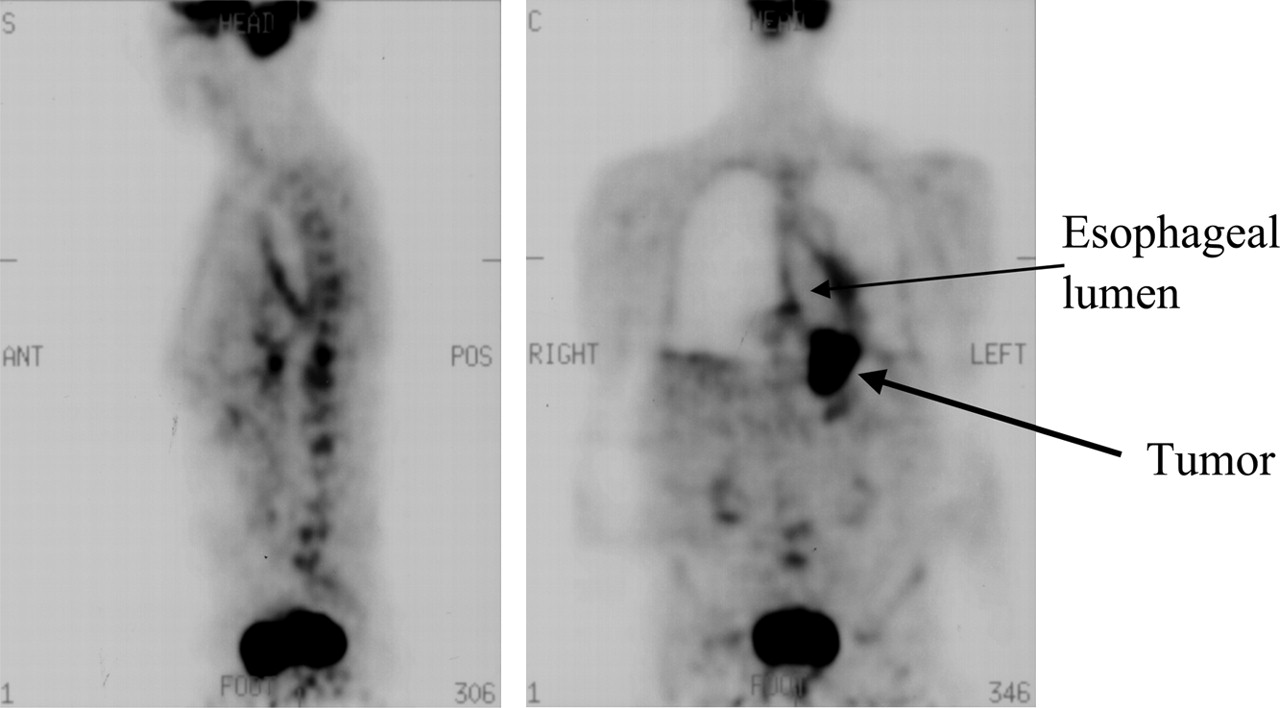
- FIGURE 8.
Dilated esophagus. A 72-y-old man with known esophageal carcinoma. Note dilated esophagus with linear increased uptake on both sides. Chronic dilation is due to distal obstruction by tumor mass. Linear uptake is due to reactive inflammation. ANT = anterior; POS = posterior; S = sagittal; C = coronal.
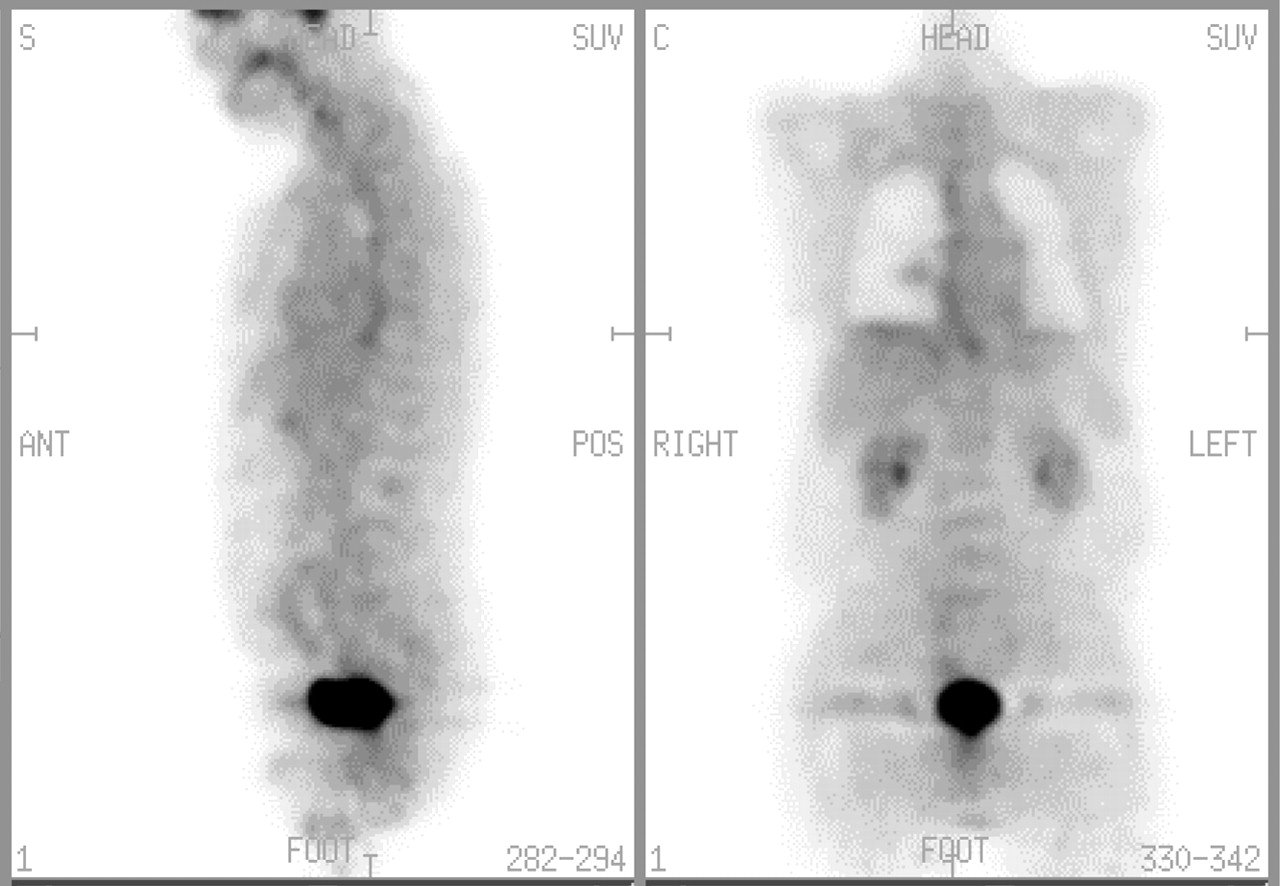
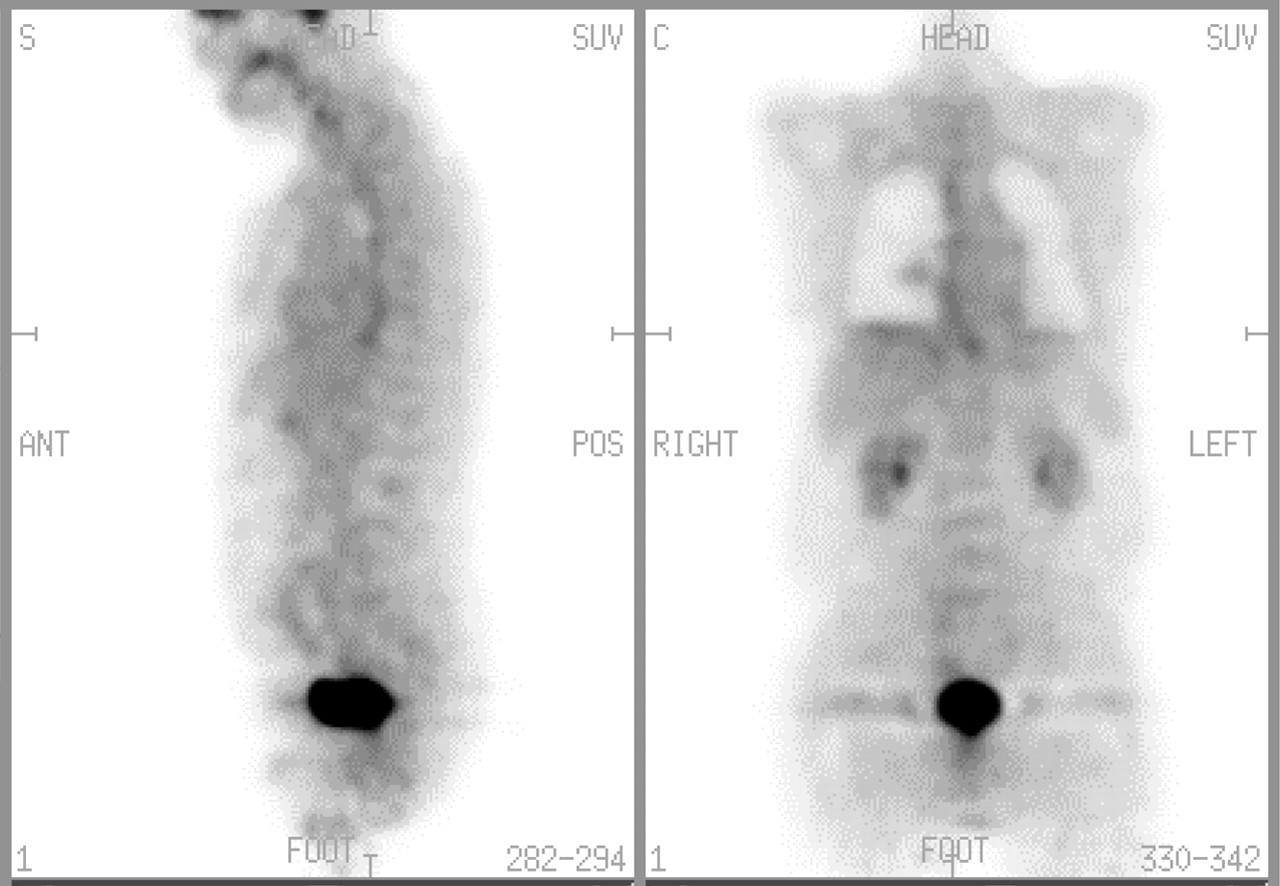
- FIGURE 9.
Esophageal uptake. Esophageal uptake in patient with gastroesophageal reflux disease. S = sagittal; C = coronal; ANT = anterior; POS = posterior.
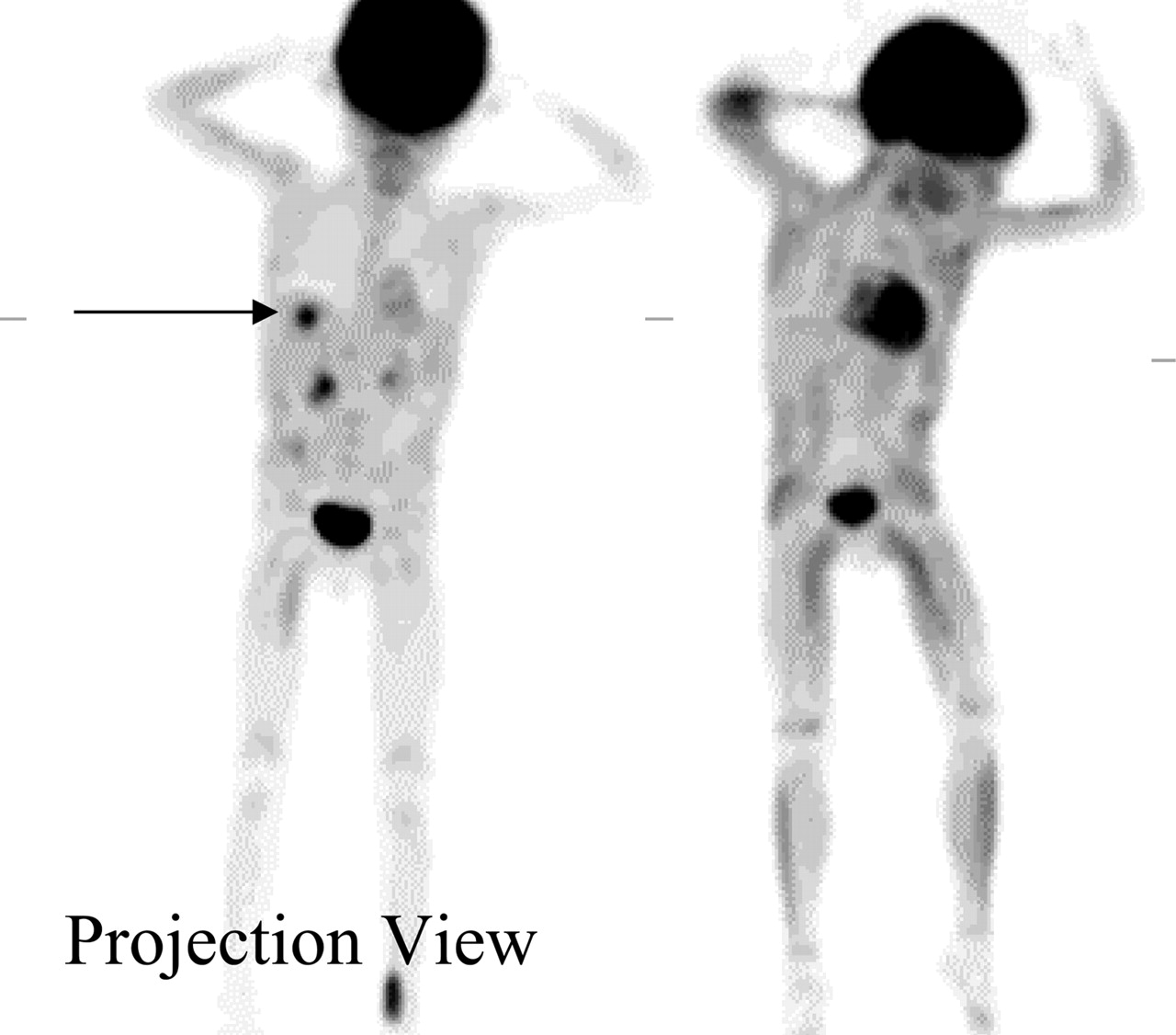
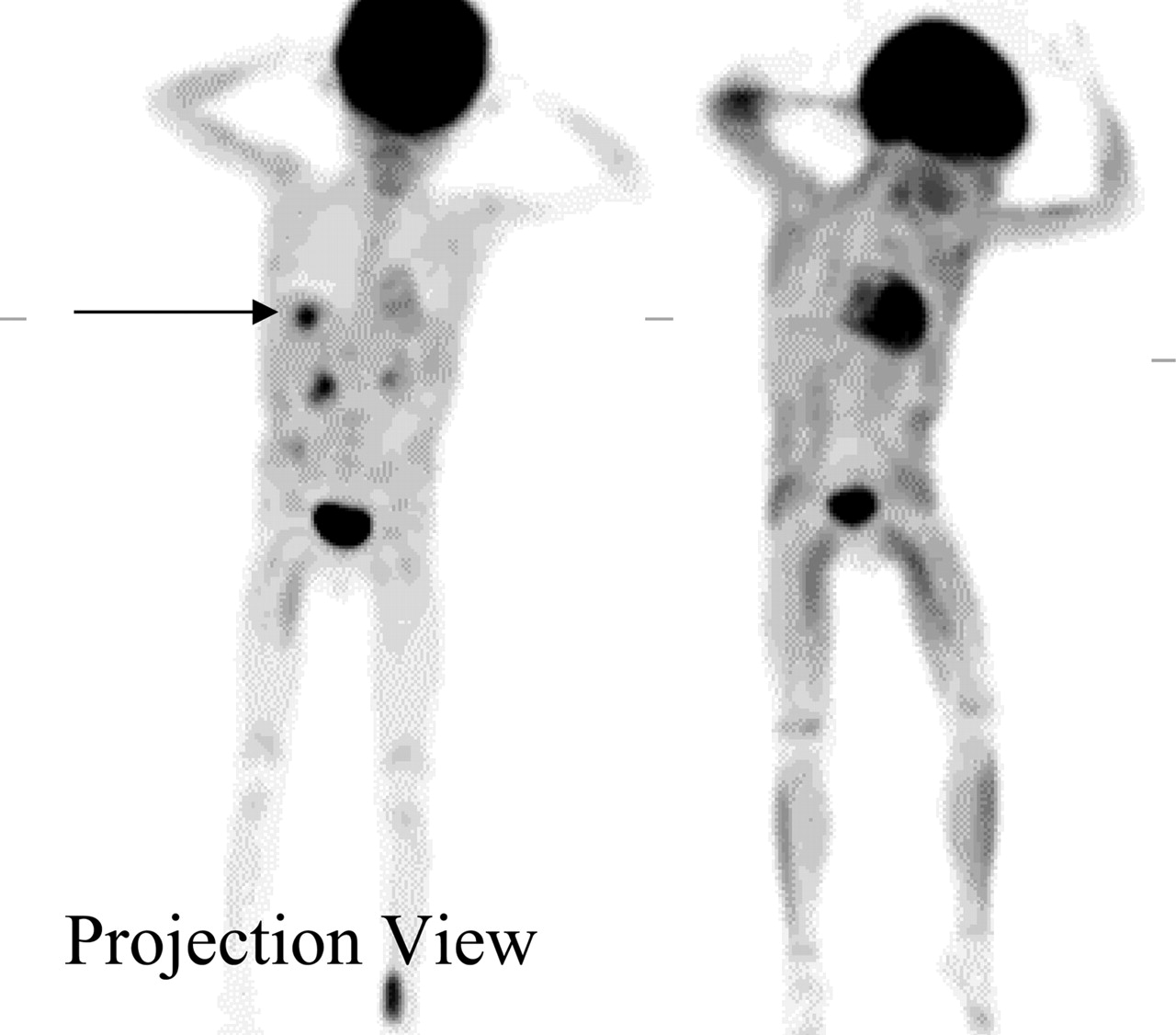
- FIGURE 10.
Colonic activity (projection view). Patient had bladder cancer, status post cystostomy, and ileal conduit. PET was done to rule out pelvic recurrence. Note nonspecific diffuse colonic activity (a), ileal conduit (b), urinary bag (c), and area of recurrence (d).
- FIGURE 11.
Cecal uptake. (A and B) Normal diffuse physiologic uptake (arrow) in cecum. C = coronal.
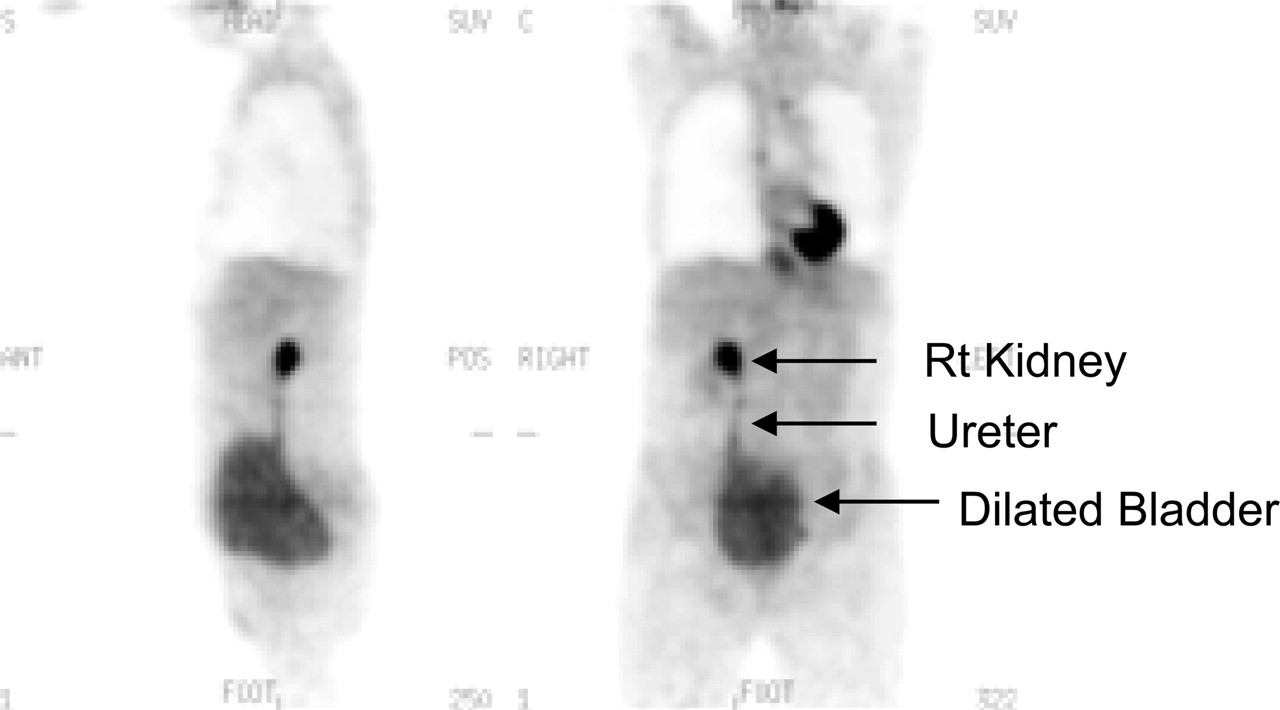
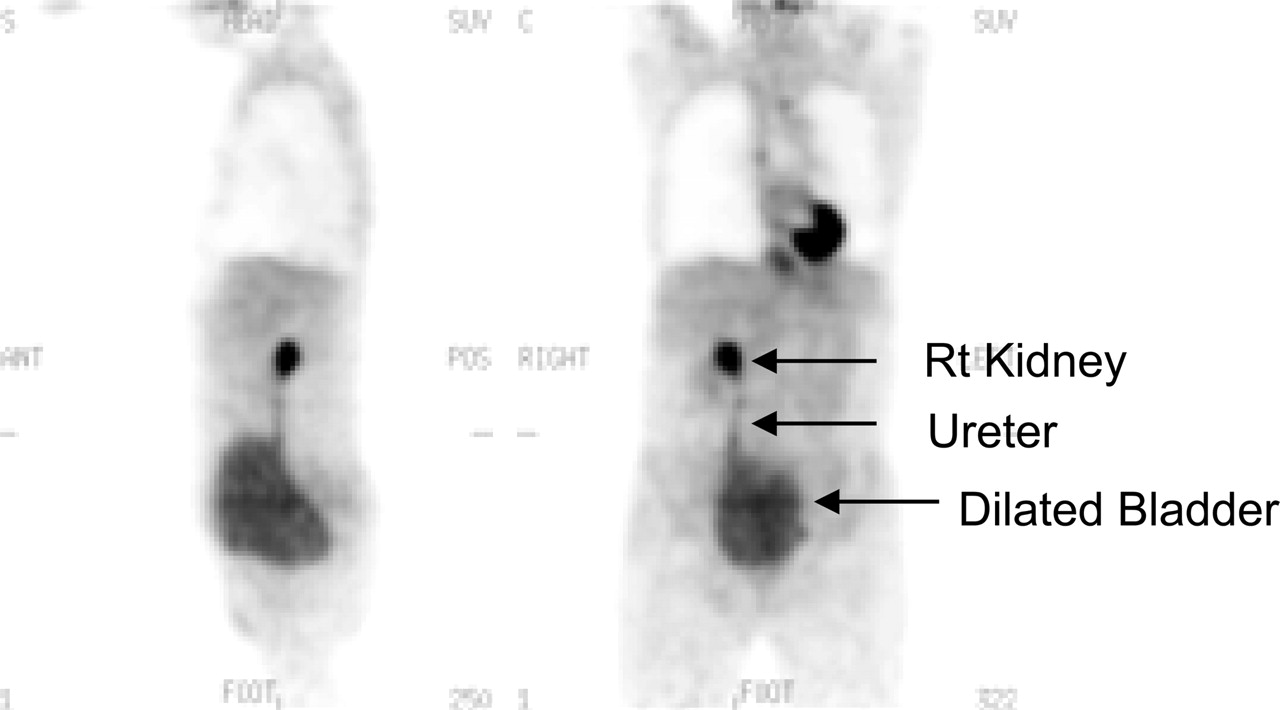
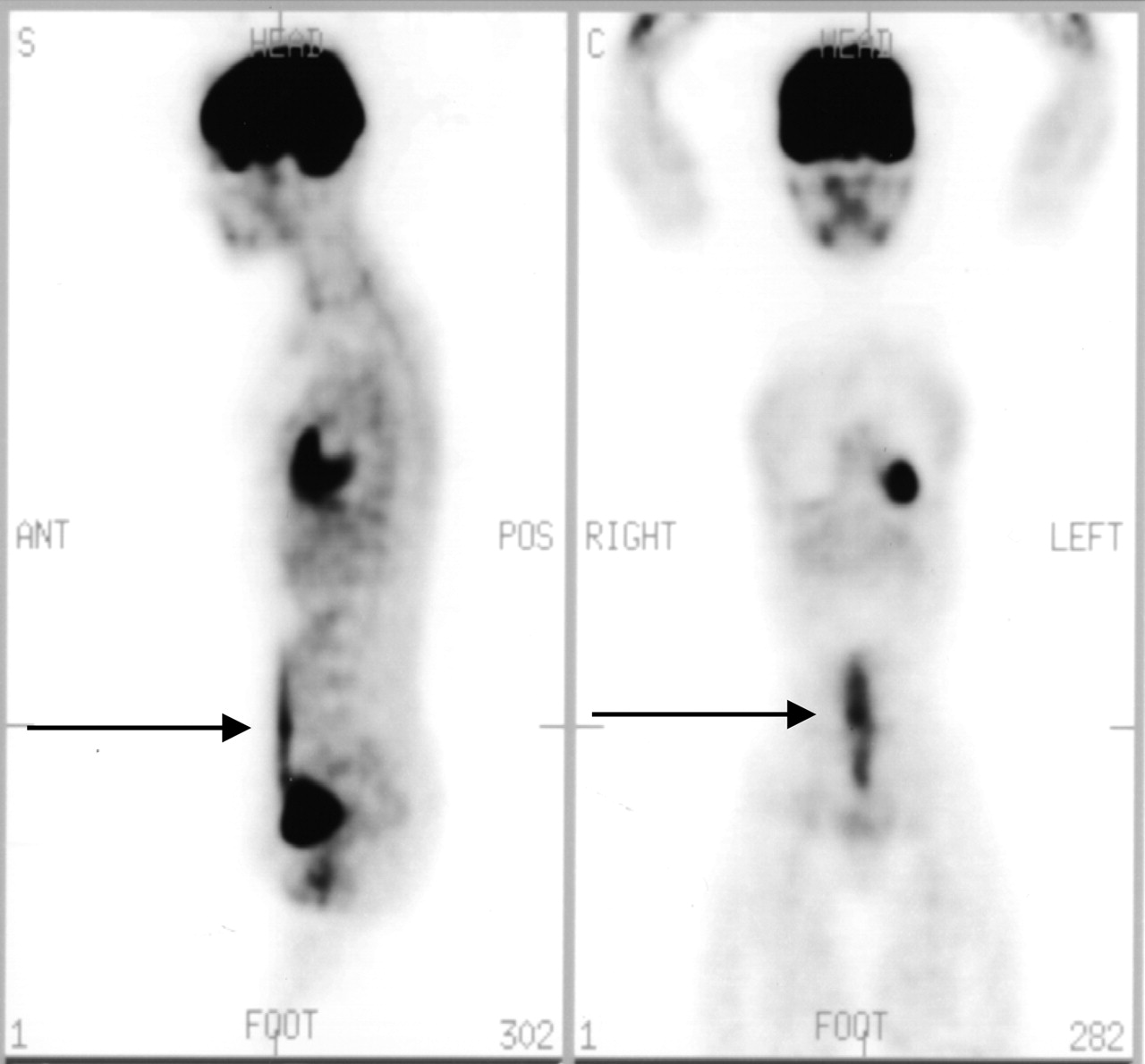
- FIGURE 12.
Dilated urinary bladder. Note prominent right (Rt) kidney collecting system, right ureter, and dilated urinary bladder.
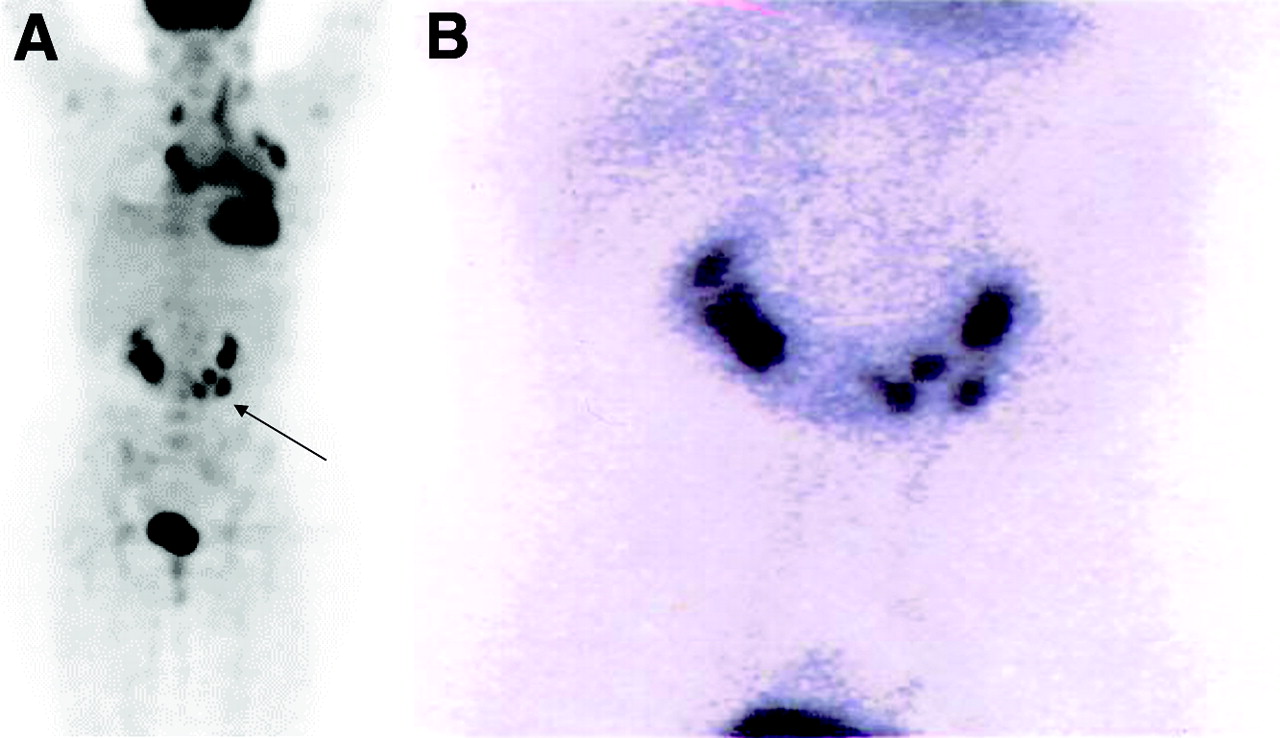
- FIGURE 13.
Horseshoe kidney. (A) Horseshoe kidney (arrow) seen on 18F-FDG PET scan (projection view on left). Patient with Hodgkin’s lymphoma. (B) 99mTc-Glucoheptonate scan confirms presence of horseshoe kidney.
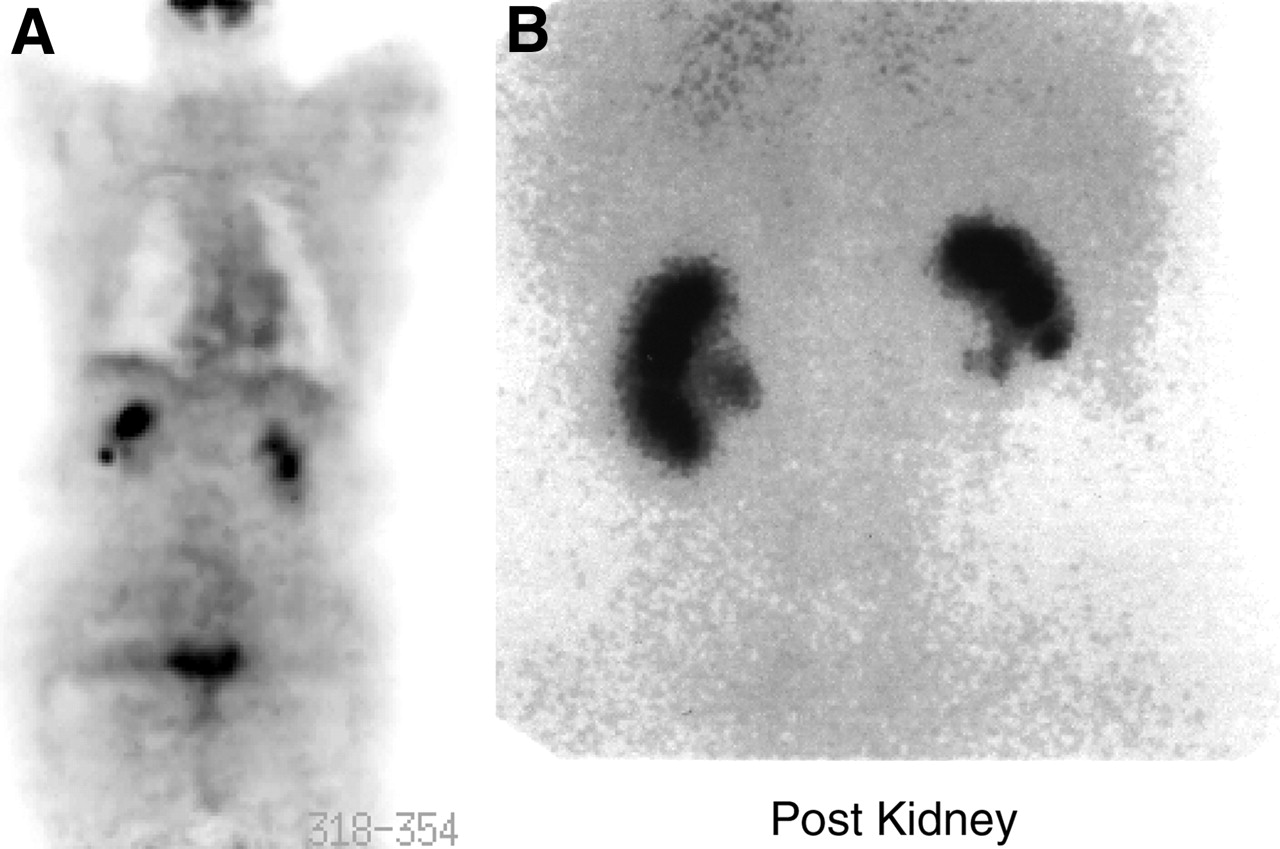
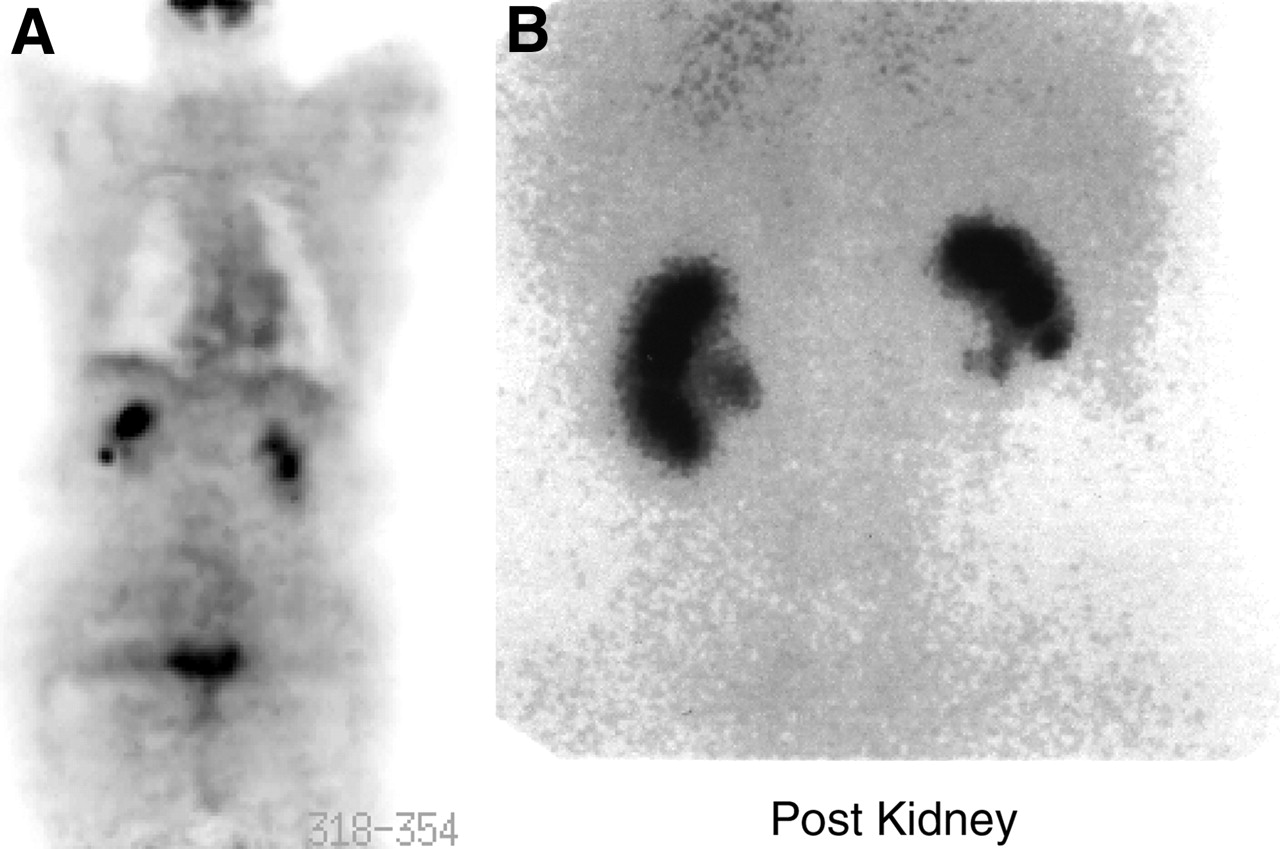
- FIGURE 14.
Renal activity. (A) Intense activity in right kidney collecting system overlapping right lobe of liver, simulating a liver lesion. (B) 99mTc-Dimercaptosuccinic acid image of same patient confirms that right kidney is slightly higher than left. Post = posterior.
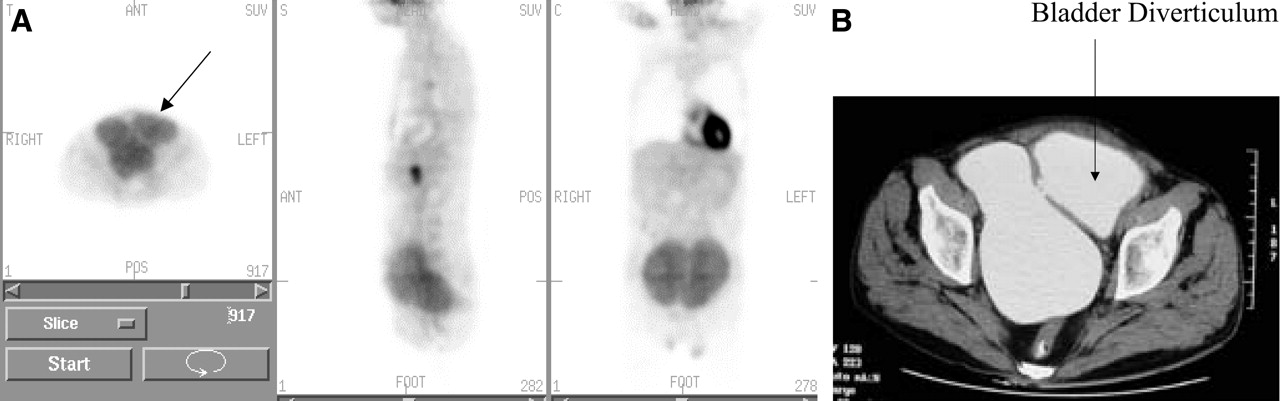
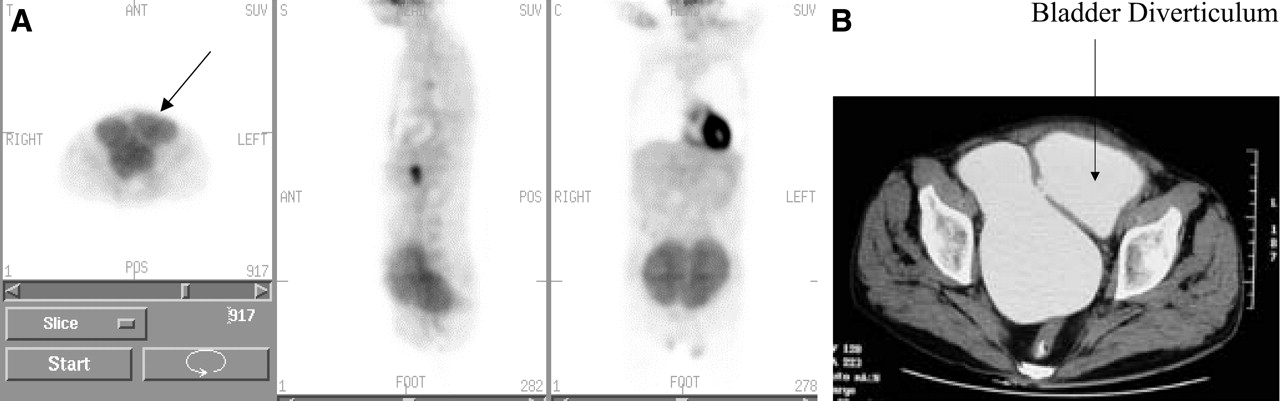
- FIGURE 15.
Bladder diverticulum. (A) Bladder diverticulum caused by chronic bladder outlet obstruction by hypertrophied prostate. (B) Corresponding CT scan. ANT = anterior; POST = posterior; S = sagittal; C = coronal.
- FIGURE 16.
(A) Nephrostomy tube (arrow). (B) Diaper artifact. POS = posterior.
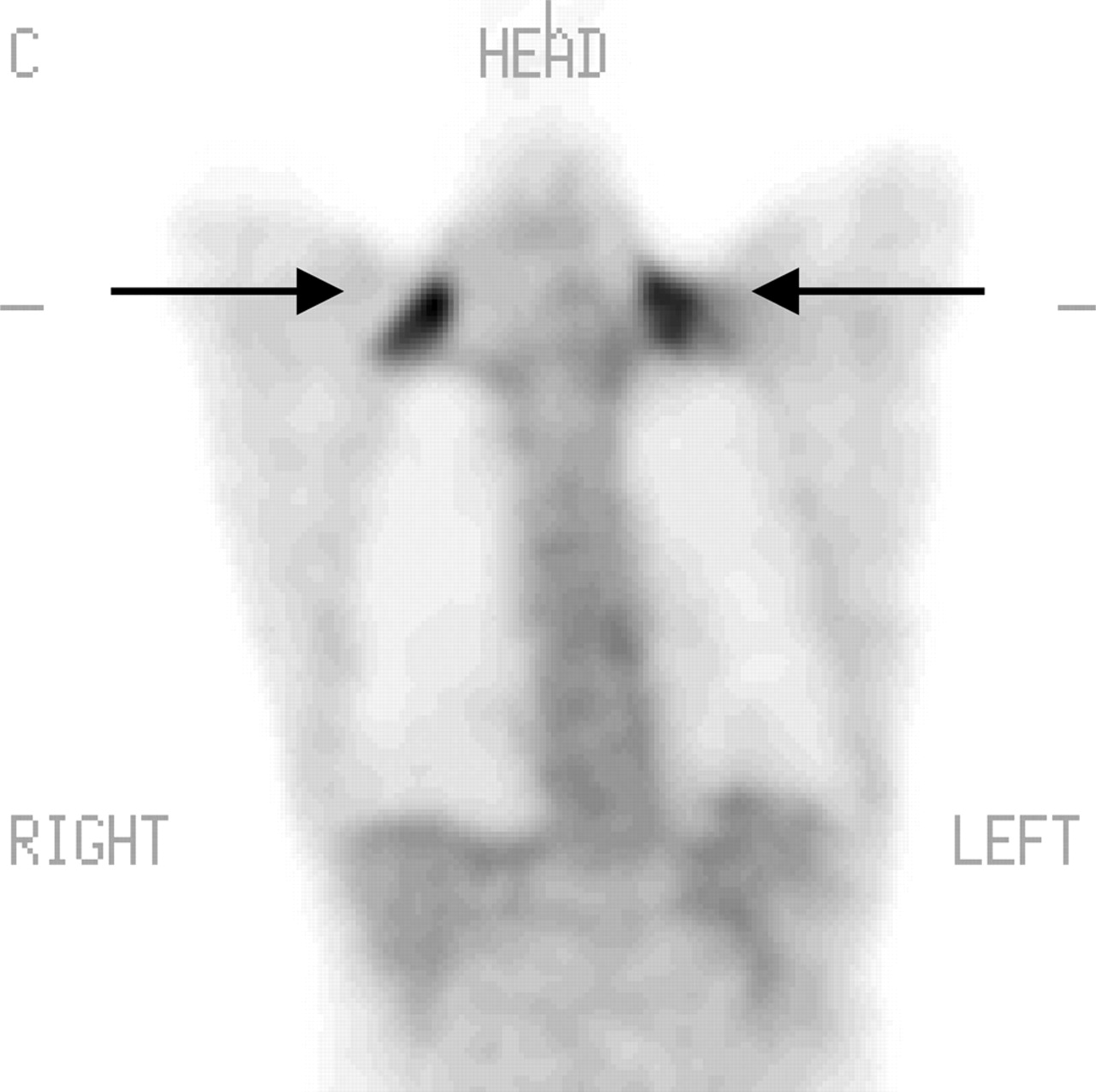
- FIGURE 17.
Muscle uptake. Symmetric muscle uptake in neck (arrows). C= coronal.
- FIGURE 18.
Intercostal muscle uptake due to persistent coughing (projection view).
- FIGURE 19.
Brown fat uptake. (A) Asymmetric neck uptake (arrows). (B) Intense symmetric uptake in adipose tissue (arrows). Brown fat can cause difficulty in scan interpretation. C = coronal.
- FIGURE 20.
Thymus uptake (coronal views). (A) Diffuse thymus uptake (arrow). (B) Focal thymus uptake (arrow).
- FIGURE 21.
Bone marrow. Intense 18F-FDG uptake in bone marrow is attributed to hematopoietic growth factor.
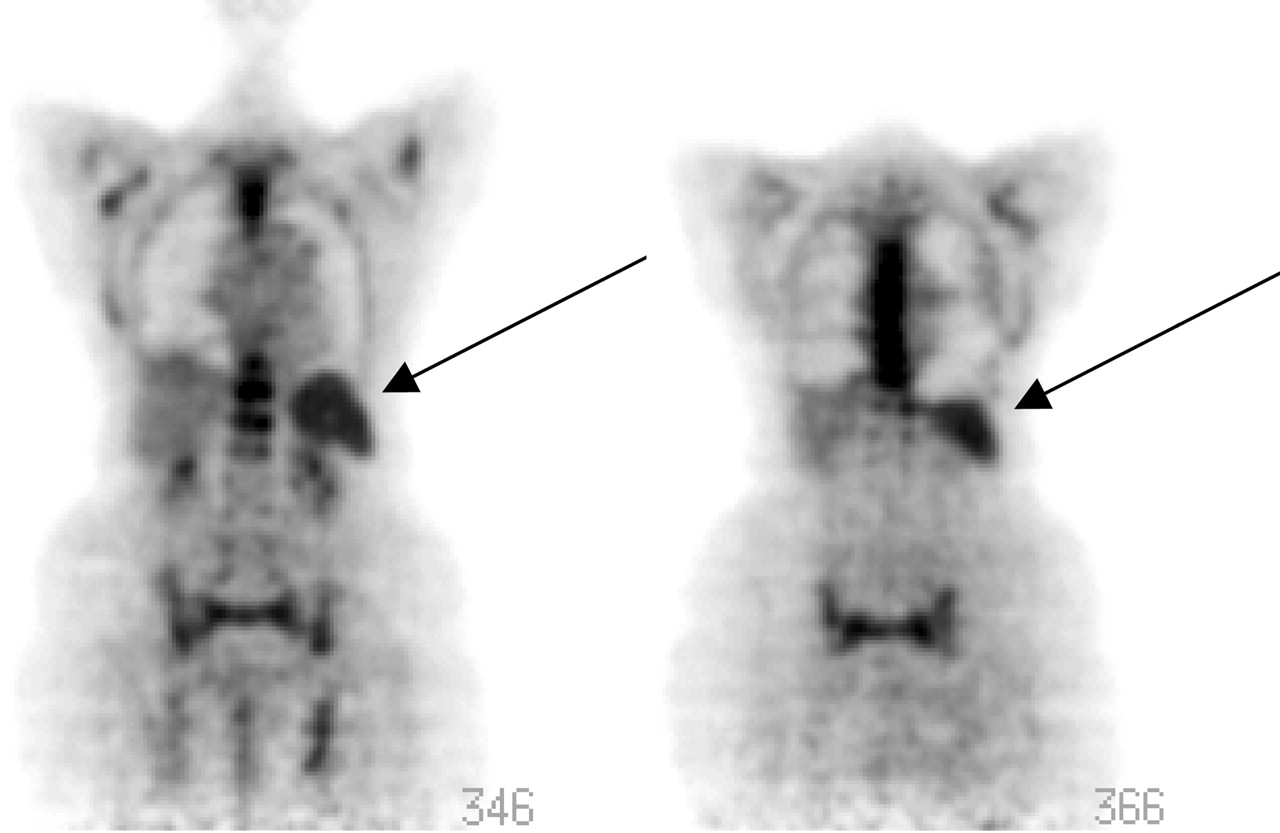
- FIGURE 22.
Spleen uptake (arrows) due to hematopoietic growth factor.
- FIGURE 23.
18F-FDG uptake in lymph nodes attributed to tuberculosis (projection view).
- FIGURE 24.
Fungal infection in liver of pediatric patient. (A) Before therapy (arrow). (B) Infection resolved on image after specific antifungal therapy.
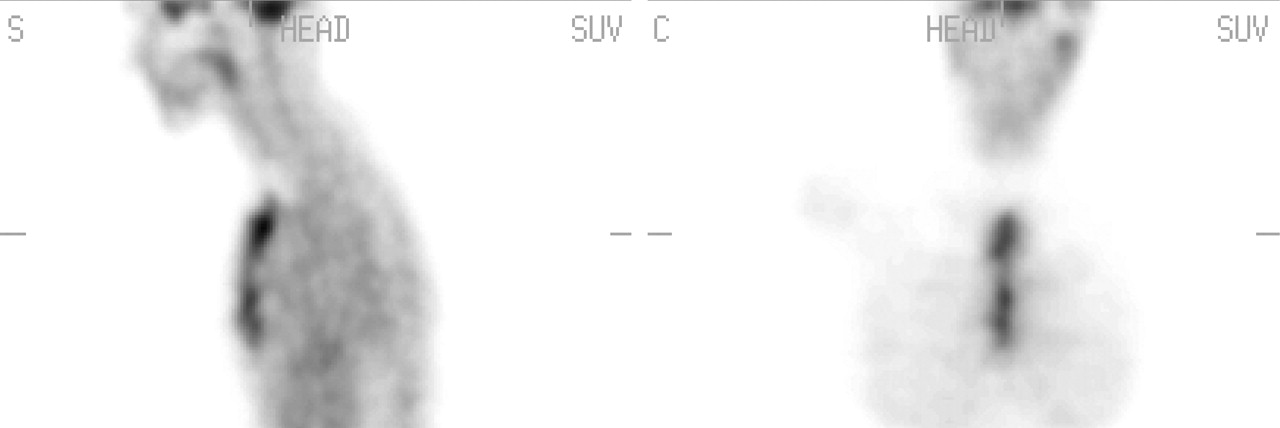
- FIGURE 25.
Scar tissue from recent surgery. Patient underwent recent abdominal surgery for hernia repair. Note linear superficial increased 18F-FDG uptake along anterior abdominal wall conforming to abdominal scar tissue (arrow). S = sagittal; C = coronal; ANT = anterior; POS = posterior.
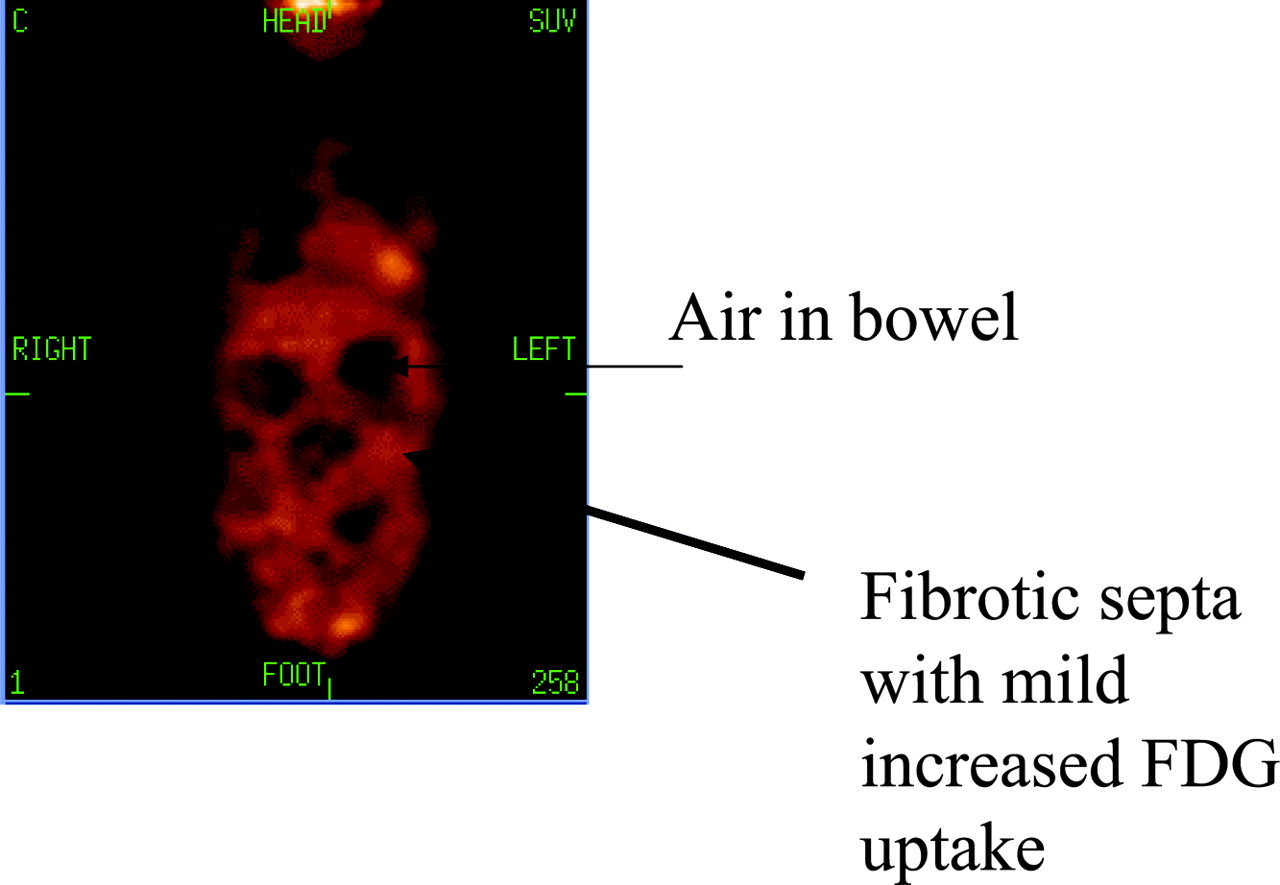
- FIGURE 26.
Abdominal fibrosis, honeycomb appearance. Patient had history of multiple abdominal surgeries leading to scattered segmental fibrosis. Image shows mild 18F-FDG uptake between dilated loops of bowel forming the honeycomb appearance. C = coronal.
- FIGURE 27.
Uptake in sternum after coronary artery bypass grafting. Patient had open-heart surgery 1 wk before 18F-FDG study. S = sagittal; C = coronal.
- FIGURE 28.
Postsurgical hematoma (arrows). Patient had excisional breast biopsy 10 d before 18F-FDG scan. ANT = anterior; POS = posterior; S = sagittal; C = coronal.
- FIGURE 29.
Intense aortic uptake due to inflammation (unstable plaque formation).
- FIGURE 30.
Breast uptake, lactating female. ANT = anterior; POS = posterior; C = coronal.










Tables
Fasting—nothing by mouth for 4–6 h
No strenuous exercise 24 h before PET
Check blood glucose level (ideally between 120 and 150 mg/dL)
Start intravenous line for 18F-FDG administration
During circulation time, the patient should rest on a cart or recliner
Patient should void before scanning
Remove any metallic objects
Make the patient comfortable under the scanner—that is, use head and arm support
Surgical history: type, site, date of previous surgery or biopsy, site and types of stomas if present
Clinical history: complaints, type and site of tumor, date of diagnosis
Current therapy: chemo/radiotherapy, bone marrow-stimulating factors—for example, granulocyte colony-stimulating factor
Previous therapy received
History of trauma or recent falls
Results of previous radiologic investigations; review the patient’s film (CT, MRI, and so forth)





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}