


Abstract
PET has seen rapid progression in recent years, with applications in oncology leading the way. The glucose analog 18F-FDG is the most commonly used PET radiopharmaceutical and has been shown to accumulate avidly in several different neoplasms, including cancers of the lung. The following discussion will review the physiologic basis for the uptake of 18F-FDG in lung neoplasms and demonstrate the utility of 18F-FDG PET in lung cancer. A brief review of other PET radiopharmaceuticals in lung cancer imaging, and dual-modality PET/CT scanners, will be presented. Upon completion of this article, the reader should be able to describe the pharmacokinetics of 18F-FDG and discuss the efficacy of 18F-FDG PET scans in the evaluation of solitary pulmonary nodules, disease staging, and monitoring response to therapy. Additionally, the reader should be able to compare 18F-FDG PET with conventional anatomic imaging and describe some of the technical challenges of PET/CT fusion imaging.
PET has seen rapid progression in recent years, from a research tool to routine clinical use. Much of the increased use of PET can be attributed to applications in oncologic imaging and the increased availability of the radiopharmaceutical 18F-FDG, which is the most extensively used PET radiopharmaceutical (1). 18F-FDG has been shown to be taken up by several neoplasms, including cancers of the lung.
Lung cancer has the regrettable distinction of being the most common cause of death by malignancy in both men and women (2,3). Approximately 3 million new cases arise each year (4). The mean survival time for untreated lung cancer is a mere 6 mo, with a 5-y survival rate of 13% (5). Even after surgical resection of tumor tissue, the 5-y survival rate is <40% (6). Common metastatic sites in lung cancer include the liver, bone, and adrenal glands (7,8).
Non–small cell lung cancer (NSCLC) accounts for 80% of bronchogenic malignancies and is often amenable to surgery, especially in patients with stage I and stage II disease (9). Conversely, small cell lung carcinomas have a more dismal prognosis, as they generally present with widespread disease that is not amenable to surgical resection. The mean survival is <1 y even when treated aggressively (2).
The vast majority of the literature surrounding 18F-FDG PET of the lungs has focused on patients with NSCLC, in whom local and distant spread of disease can change staging and therapy. The uptake of 18F-FDG in NSCLC has been shown to be severalfold greater than that of normal tissue (7). Small cell lung cancer also exhibits high 18F-FDG uptake, and preliminary studies have shown 18F-FDG to be of use in this imaging as well.
Despite the high cost of 18F-FDG PET, it has been proven to be an economical tool in the evaluation of lung cancer. 18F-FDG PET has the potential to alter the staging of disease, reduces the number of futile thoracotomies, and thus may be cost-effective in this indication. The following discussion will focus primarily on the utility of 18F-FDG PET in NSCLC. The role of 18F-FDG PET in diagnosis, staging, and evaluating response to treatment as well as some of the limitations of this technique will be discussed. Finally, a brief look at new developments and future directions of PET in lung cancers will be presented.
TECHNIQUE
Pharmacokinetics
The glucose analog FDG is the most commonly used PET radiopharmaceutical for the investigation of lung cancer. FDG uptake in cells is directly proportional to glucose metabolism. As with endogenous glucose, intravenously injected FDG is transported into cells by means of glucose transporter proteins and then phosphorylated to FDG-6-phosphate via the enzyme hexokinase. FDG-6-phosphate does not act as a substrate for the next step in the glycolytic pathway and, as such, the radiopharmaceutical is sequestered within the cell. Malignant cells demonstrate an increased number of glucose receptors, upregulation of hexokinase action, and diminished phosphatase activity, which all serve to facilitate FDG uptake and retention (8). Viable lung cancer cells exhibit a particularly high accumulation of FDG compared with normal lung tissue, which can be exploited for imaging purposes and, in particular, to differentiate benign from malignant lesions. The degree of FDG accumulation has been shown to correlate well with cell dedifferentiation, disease aggressiveness, and tumor grade (10).
Quantitation
In addition to visual qualitative evaluation, 18F-FDG accumulation in lesions can also be assessed via semiquantitative means, most often with standard uptake values (SUVs). In general, pulmonary nodules with an SUV of >2.5 are considered malignant (3,11). The ability to calculate the 18F-FDG avidity of lesions can prove beneficial in assessing response to therapy by helping differentiate residual malignancy from benign posttherapeutic changes.
Instrumentation
The explosion of PET in cancer has necessitated the development of cost-effective imagers. Attempts at 18F-FDG imaging with conventional SPECT cameras fitted with ultra-high-energy collimators have been undertaken in the past but were found to be unsatisfactory because of the poor sensitivity and lower spatial resolution compared with dedicated PET scanners (12). Subsequently, dual-head γ-cameras with thallium-activated sodium iodide crystals have been modified for true coincidence detection. These “hybrid” systems can be operated in either coincidence mode for imaging PET radiopharmaceuticals or single-photon mode for routine nuclear medicine studies. These systems are less costly than dedicated PET scanners, offer greater versatility due to the ability to perform routine single-photon imaging, and have spatial resolution comparable to that of dedicated PET scanners. Unfortunately, the instrumentation of these hybrid systems has a limited counting rate capability compared with dedicated PET scanners, and the reduced sensitivity often leads to count-poor, noisy images, with diminished contrast resolution. A 1998 study comparing the 2 devices found that hybrid scanners detected 93% of lung nodules, 65% of malignant mediastinal lymph nodes, and only 42% of distant metastases observed on dedicated PET (13). A more recent study found that, on visual analysis of lesions of >2 cm in diameter, the techniques showed equal utility, but for smaller lesions dual-head coincidence systems were inferior to dedicated PET scanners (12). In semiquantitative analysis, the tumor-to-background ratio of pulmonary lesions was also lower on the coincidence systems.
Recent advances have seen the direct integration of CT capability with PET scanners. The use of this dual-modality imaging (PET/CT) has been found to significantly improve the number of correctly staged patients with NSCLC (9). PET/CT is further discussed later in this review.
Acquisition
Patient preparation is important in performing an oncology PET scan, to maximize FDG uptake in tumors and limit uptake in normal structures. Patients should fast for at least 4 h before the scan to limit serum glucose and insulin levels. Some institutions check the serum glucose level before administration of 18F-FDG. Between injection of 18F-FDG and imaging there is an uptake period of 30–60 min. During the uptake period patients lie quietly to limit muscle uptake of 18F-FDG and are kept warm to prevent shivering and resultant uptake of 18F-FDG in muscles and brown fat. The dose of 18F-FDG varies depending on the type of scanner and institutional preference, but typically it is in the range of 370 MBq (10 mCi). More detailed information on patient preparation for oncology PET scans is available in the literature (14).
Because PET scanners have a limited field of view, imaging is required at several bed positions to cover the entire area of interest, which is usually from skull base to pelvis. At each bed position a transmission scan is obtained using a rotating rod source for purposes of attenuation correction. This is followed by an emission scan, in which the activity from the 18F-FDG itself is imaged. The duration of the acquisition also depends on the type of scanner and, in particular, the type of crystal and institutional preference; emission scans are typically in the range of 6–15 min per bed position, whereas transmission scans are typically 2–3 min per bed position. With PET/CT scanners, the CT replaces the transmission scan, and the entire transmission map is acquired at the beginning of the scan in a matter of seconds. This discussion serves only as an overview of 18F-FDG PET acquisitions. Further details and guidelines for tumor imaging with 18F-FDG are available in the literature (15).
INTERPRETATION
Evaluation of Solitary Pulmonary Nodules (SPNs)
The finding of a SPN on routine chest radiographs is quite common, with the differential diagnosis including malignant and benign neoplasms as well as the sequela of infections (8). An important determination must be made promptly: Is the lesion malignant or not? Approximately 30%–50% of these nodules will turn out to be malignant (2,5), though this range has varied between 20% and 70% in various studies (8). This large variability may be a consequence of regional differences in the relative incidence of lung cancer and benign pulmonary disease—for example, in areas where histoplasmosis or coccidiomycosis are endemic.
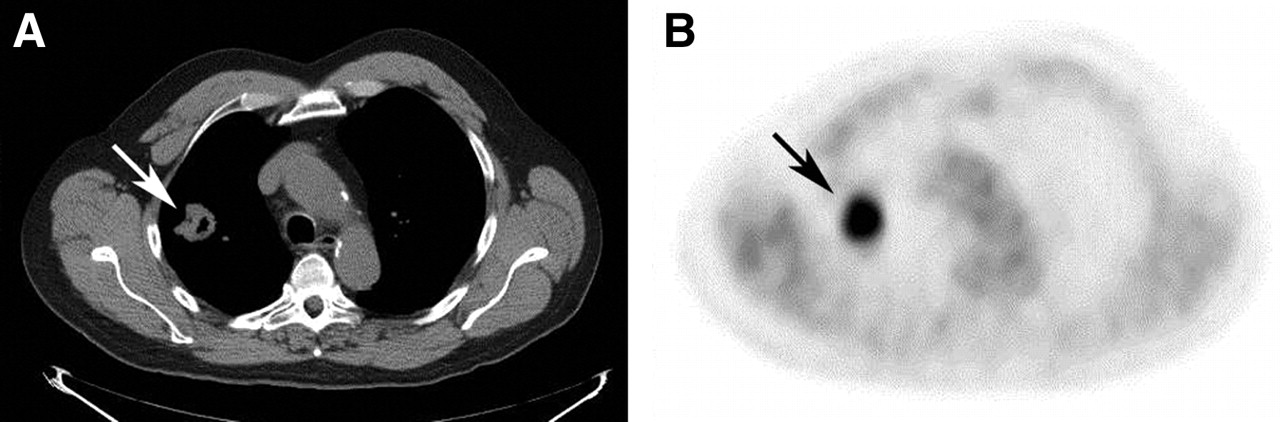
Radiographs and CT scans of the chest are limited in their ability to differentiate benign from malignant nodules. Recently, MRI has been used in the evaluation of lung masses as well, but this technique is suboptimal (16). Such anatomic imaging is useful for localization of nodules and can differentiate one third of SPNs based on image characteristics, including size (17). Percutaneous biopsy of these lung nodules has a yield of 90%, but negative results still cannot definitively exclude the possibility of malignancy (2). Additionally, some invasive tests to diagnose lung cancer are associated with a morbidity rate of 1%–10% (18). Accurate, noninvasive methods to evaluate SPNs that are indeterminate on anatomic imaging would be extremely advantageous. Figure 1 depicts the CT scan of a 62-y-old male patient demonstrating a nodule in the right lung. The corresponding PET scan shows marked increased uptake of 18F-FDG, indicating a high likelihood of malignancy. Indeed, this turned out to be a NSCLC.
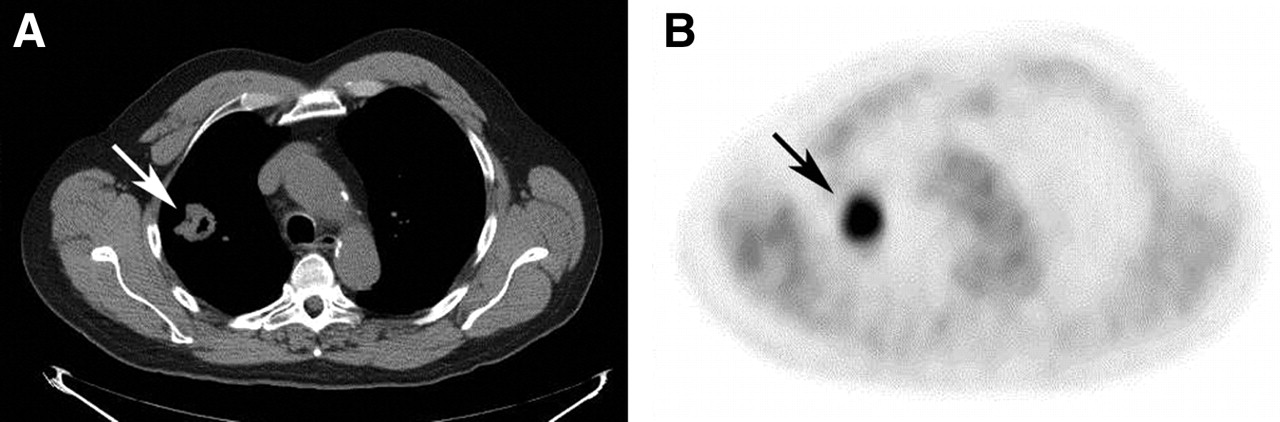
(A) CT scan identifies a nonspecific nodule in right lung (arrow). (B) Axial view at same level from the PET scan demonstrates markedly increased 18F-FDG uptake in lung nodule (arrow), which proved to be lung cancer.
A recent meta-analysis found 18F-FDG PET to be highly accurate in differentiating benign from malignant lesions with a very high sensitivity of 97% and specificity of 78% (19). Specificity is reduced as significant 18F-FDG uptake is noted in many inflammatory conditions such as bacterial pneumonia and in tuberculosis and other granulomatous diseases (2,3,20). Such false-positive examinations are of concern as they may subject patients to unnecessary invasive procedures, but the number of patients undergoing such procedures will still be significantly reduced through the use of PET.
Although rare, false-negative 18F-FDG PET results are also possible. The sensitivity of PET is diminished in small lesions. A phantom study suggested that nodules <0.7 cm in diameter are unlikely to be localized due to partial-volume effects that result from the limited scanner resolution or, possibly, respiratory motion during imaging (21). False-negative 18F-FDG PET results have also been shown in low-metabolism neoplasms, such as primary pulmonary carcinoids and bronchoalveolar cell carcinomas (8,14,22), and in patients with elevated serum glucose levels (2). Some PET-negative nodules, as defined by an SUV of <2.5, may in fact be malignant. Though a negative 18F-FDG PET scan makes it very unlikely that a SPN is malignant, particularly if it is >1 cm, it is probably prudent to follow such lesions with noninvasive imaging. Serial CT examinations have been suggested for this purpose (3). In patients with negative 18F-FDG PET studies, but a high pretest likelihood of cancer, histologic diagnosis may still be warranted. Definitive diagnoses can only be obtained through invasive procedures, including bronchoscopy, biopsy, and mediastinoscopy (23).
Staging
After the diagnosis of lung cancer has been made, accurate staging is necessary to appropriately manage the patient. The most standardized system for staging NSCLC is the TNM system, where T denotes the size of the primary tumor, its location, and level of invasion; N indicates the status of regional lymph nodes; and M refers to the presence or absence of more distal metastases (2,3). These parameters are used in defining the overall disease stage. PET alone cannot establish T status as it lacks sufficient resolution and anatomic delineation. For example, PET may fail to detect invasion of the bronchial wall, pleura, or local vasculature (2). Although PET cannot accurately perform the staging of the tumor alone, it is useful in evaluating the tumor in that the semiquantitative SUV in patients with NSCLC has proven to be of prognostic value. In NSCLC, patients with tumor SUVs of >10 had a survival rate less than half that of patients with an SUV of <10 (24). CT is useful in T staging and, consequently, a combined PET/CT study, if available, would be useful in T staging. The true utility of PET in staging, however, lies in staging local and distant spread of the disease.
In staging the mediastinum, 18F-FDG PET is increasingly being used in lieu of more invasive methods to differentiate benign versus malignant pathology. Traditionally, noninvasive staging was performed with CT and, to a much lesser extent, MRI. These techniques are limited as they use size as their primary criterion for malignant lymph nodes. As such, any nodes greater than 1 cm are typically noted as malignancies, whereas those that fall below this size are reported as not having tumor involvement. False-positive and false-negative findings in assessment of these nodes can lead to erroneous staging and inappropriate therapeutic management. 18F-FDG PET uses a criterion based on increased glucose metabolism, not size, and has been shown to be superior in both sensitivity and specificity to CT staging of the mediastinum (25). In a recent test performance study of PET and CT for overall mediastinal staging of NSCLC, PET was shown to be more accurate (25). Analysis of pooled data from several studies showed CT to have a sensitivity of 57% and a specificity of 82%, whereas PET had a sensitivity of 84% and a specificity of 89% for staging of the mediastinum (26).
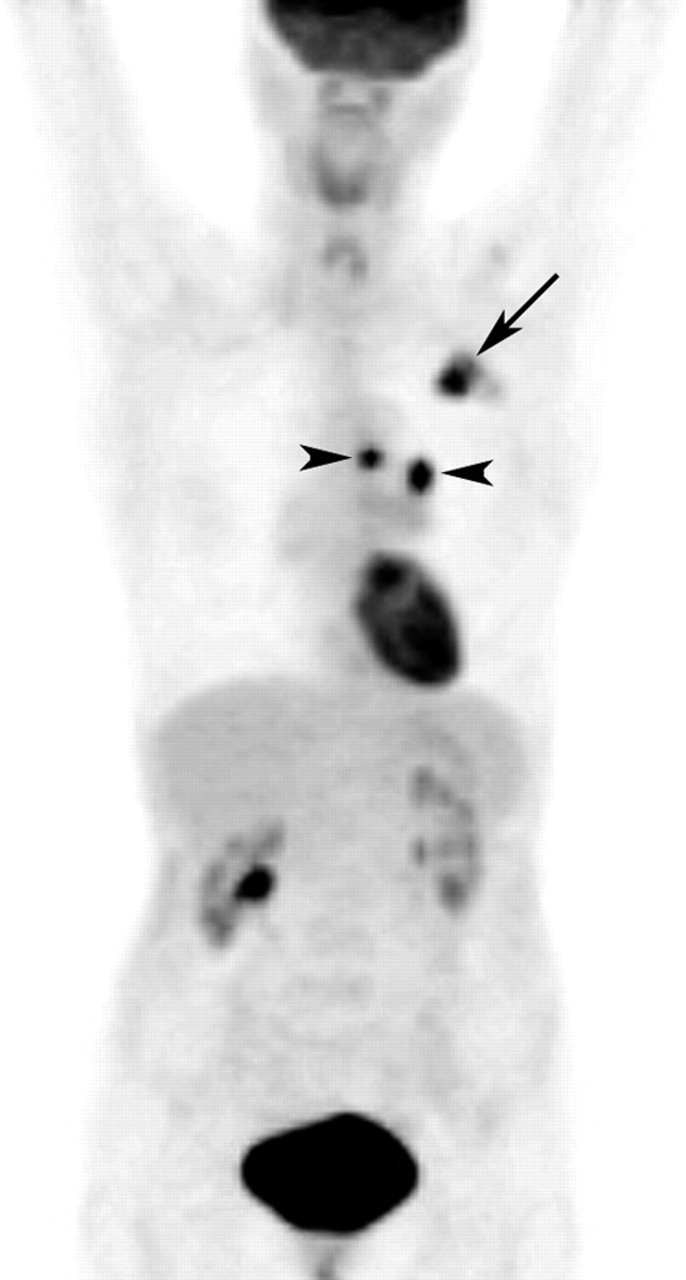
Figure 2 is the PET scan of a 57-y-old woman with a known lung cancer in the left upper lobe undergoing staging evaluation. The PET scan demonstrates intense uptake in the known cancer as well as in 2 mediastinal lymph nodes on the left. Importantly, there is no abnormal uptake in the contralateral mediastinum, or elsewhere in the body, indicating the cancer is unlikely to have spread beyond the left side of the mediastinum. As a result of the PET staging, the patient is considered a candidate for surgical therapy.

Maximum-intensity-projection image from 18F-FDG PET scan demonstrates intense uptake in known lung cancer in left upper lobe (arrow) as well as within 2 small ipsilateral mediastinal lymph nodes (arrowheads). Importantly, PET scan does not show abnormalities more distally.
Whole-body 18F-FDG PET has the advantage of being able to detect distant metastases that are not observed on more conventional anatomic imaging (10,16). Such findings allow for more accurate staging of disease and can have consequences for treatment planning. Alterations in therapeutic management have been described in up to 41% of patients based on pretherapy whole-body 18F-FDG PET findings (27). In patients being considered for surgical intervention, PET findings result in staging changes in almost 50% of patients, with upstaging being twice as prevalent (7). Thus, the foremost impact of PET is that it leads to less aggressive therapy (7) and a significant reduction in the “futile thoracotomy rate” (28).
A recent study of 202 patients with NSCLC suggested that, despite the utility of PET in this regard, mediastinoscopy with lymph node biopsy should remain the standard for staging of the mediastinum in patients with SPNs because of the potential, though rare, of erroneous PET findings (29). However, the general recommendation is that a negative PET scan obviates the need for invasive mediastinoscopy, whereas, in the case of a positive PET scan, mediastinoscopy and lymph node sampling should still be pursued because of the possibility of false-positive PET scans (30).
Monitoring Response to Therapy
The management of NSCLC is truly multidisciplinary in nature, with roles for surgical intervention, radiotherapy, and chemotherapy. In patients with early-stage NSCLC, surgery is the most appropriate course of treatment. Patients with stage I–stage II disease, and potentially resectable masses, demonstrate a low rate of distant metastases, on the order of 5%–10% (7). In patients in whom surgery is not indicated, either because of locoregionally advanced disease or contraindications to surgery, radical radiotherapy may prolong survival (7). In patients undergoing therapy, imaging can play a crucial role and may aid in predicting the outcome of treatment regimens (31). 18F-FDG PET is clearly advantageous in the monitoring of response to treatment. Anatomic imaging alone is of limited utility after radiotherapy, as tumor sites may be concealed by atelectasis and fibrosis or inflammatory infiltration related to radiation pneumonitis (7). 18F-FDG PET uses metabolic criteria to assess tumor residual and, as such, can help differentiate tumor from scarring. It has also been shown that changes in 18F-FDG uptake precede any change in lung tumor volume (5). With CT alone, even in the presence of reduced tumor size, an accurate assessment of response to therapy is difficult. Often reduced tumor size on CT is only representative of partial, not complete, response to therapy (3) and, as such, CT has been shown to be suboptimal in restaging the mediastinum after therapy (8). In assessing for residual disease or recurrence after intervention, 18F-FDG PET is more sensitive and as specific as conventional imaging (32).
A decrease in 18F-FDG uptake after therapy is generally thought to be a sign that the tumor is responding to therapy. Such changes in 18F-FDG uptake can be assessed qualitatively, but also have the potential to be quantitated, which may aid in predicting the success of the current treatment. Patients in whom therapy achieves complete resolution of prior 18F-FDG uptake have been shown to have a good prognosis when compared with those with residual 18F-FDG uptake after treatment (3). Additionally, in patients who do not initially respond to therapy, as shown by 18F-FDG PET, the therapeutic regimen can be altered to try to deliver a more favorable outcome.
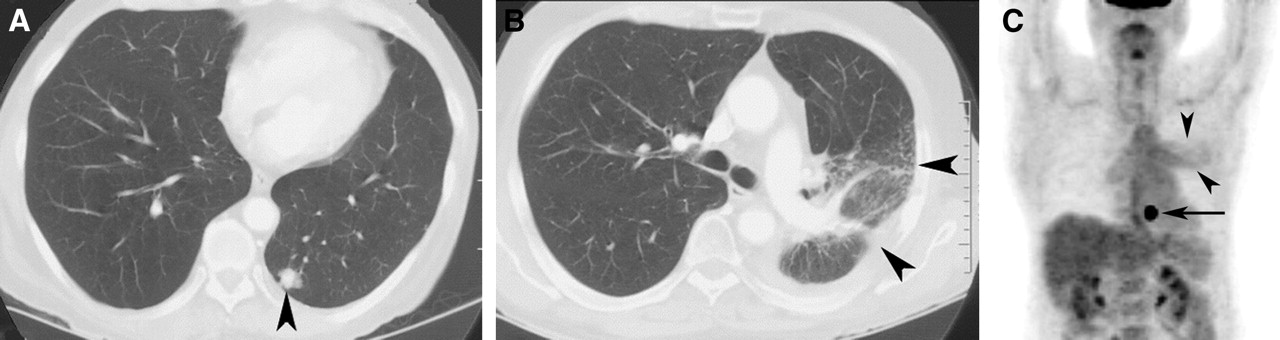
Figure 3 depicts a 72-y-old man who was previously treated with radiation therapy for lung cancer, with a new nodule discovered on a follow-up CT scan. The CT also demonstrated a larger ill-defined area of increased opacity more superiorly in the left lung. The PET scan shows intense uptake in the nodule, consistent with recurrence of the cancer. However, the larger abnormality demonstrates only mild 18F-FDG uptake, consistent with benign postradiation change. Despite the demonstrated utility of 18F-FDG PET in assessing therapeutic response, some care must be taken in assessing uptake during or immediately after therapy. Radiotherapy especially has been shown to incite inflammatory reactions that can be highly 18F-FDG avid (3). Despite successful treatment, increased 18F-FDG activity at tumor sites may be evident for several weeks after chemotherapy, and several months after radiotherapy (2).
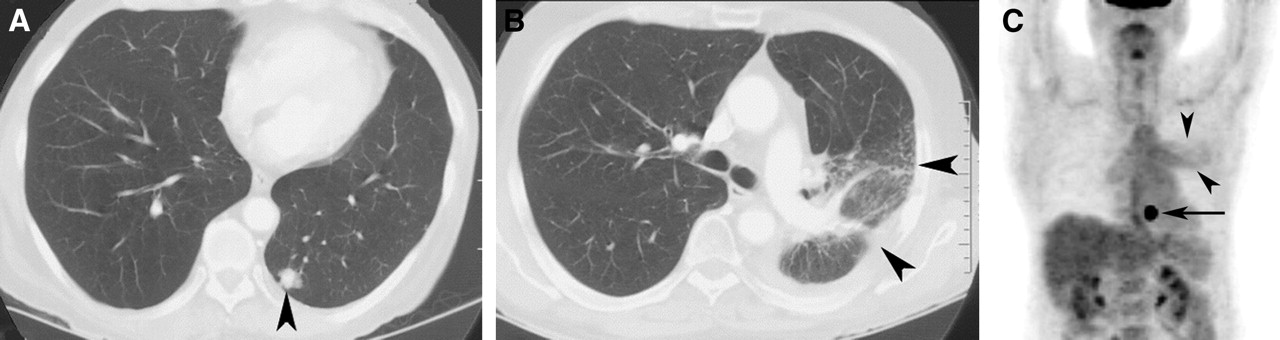
(A) CT scan demonstrates new nodule in left lower lobe (arrowhead). (B) CT scan also demonstrates a larger area of more ill-defined opacification in left lung (arrowheads). (C) Maximum-intensity-projection image from PET scan shows intense 18F-FDG uptake in nodule at left base (arrow), consistent with recurrent cancer. Larger abnormality has only mildly increased 18F-FDG uptake (arrowheads) and is consistent with radiation change.
ADJUNCTS TO 18F-FDG PET
Other PET Radiopharmaceuticals in Lung Cancers
Despite the proven utility of 18F-FDG in assessing lung cancer, other radiopharmaceuticals have been proposed for this purpose. 18F-FDG does have some limitations for this indication. False-positive results may be seen in inflammatory lung processes (2), and false-negative 18F-FDG results are possible in low-grade tumors (7). New tracers have been developed that may help offset some of these limitations or play a complementary role to 18F-FDG.
18F-Fluorothymidine has been shown to have a higher degree of uptake in highly proliferative lung cancers (33) and is not thought to accumulate in inflammatory lesions. Fluorinated choline analogs have been shown to concentrate in some low-grade adenocarcinomas, which could be of use in suspicious cases with negative 18F-FDG results (7). Lung tumors also take up 11C-acetate, but the degree of uptake does not correlate with the grade of disease (34). Thus, 11C-acetate may be of some use in identifying low-grade malignancies that show low avidity for 18F-FDG. S-methyl-11C-Methionine had been proposed as a tracer for lung cancer but, despite the advantage of having lower uptake in inflammatory lesions, it has been reported to be inferior to 18F-FDG (5).
New Technologies
Despite the utility of 18F-FDG PET, anatomic imaging is still necessary in assessment of NSCLC. Visual correlation with separately acquired CT scans, at the time of PET, has been the norm in the past. Several image coregistration techniques have been attempted with fiducial markers and complex computer software (7). Such techniques are often time-consuming and are subject to both positional and motion-induced misregistration of images (9). Of late, the commercial availability of integrated PET/CT scanners has seen much growth. They are advantageous in that patients remain in a fixed geometry for both scans, allowing for fairly accurate coregistration of the PET and CT images. As a result of differences in respiration patterns between the 2 studies, however, the registration of the PET and CT images may be less than ideal. Images from the PET/CT scan of a patient with lung cancer are shown in Figure 4. The PET images indicate the cancer has spread to both sides of the mediastinum. There are many distinct structures within the mediastinum, and the coregistered CT images help accurately differentiate the involved lymph nodes from nearby normal structures. Several early studies have shown this dual-modality imaging to more accurately stage patients with NSCLC (9,21). More accurate staging will allow for more appropriate treatment and, thus, may have prospects in reducing the number of invasive and futile interventions.

CT (A), PET (B), and fused PET/CT (C) images of patient with lung cancer. There is avid 18F-FDG uptake within lymph nodes on both sides of mediastinum (arrowheads). Fusion with CT scan helps accurately localize abnormal 18F-FDG activity, distinguishing malignant lymph nodes from normal structures in region.
CONCLUSION
The accumulation of the glucose analog 18F-FDG in lung neoplasms has been well documented. 18F-FDG PET is a highly advanced molecular imaging technique that has been shown to be of great utility in lung cancer and can facilitate noninvasive, in vivo quantification of tumor status. 18F-FDG PET has a significant role to play in the diagnosis, staging, and evaluation of response to therapy in lung carcinoma. PET has the advantage of better identifying locoregional and distant metastases than conventional anatomic imaging such as CT or MRI. This has the potential to change both the staging and therapeutic management of lung carcinoma and, in the case of upstaging, decreases the number of futile and invasive interventions.
Though it is not without limitations, the advantages of 18F-FDG PET over invasive and surgical assessment of lung cancer and the anatomic imaging modalities have already been shown to alter the management strategies of many patients with lung cancer. 18F-FDG PET is now a widely accepted imaging modality for the evaluation of patients with lung cancer. The rapid technologic advances in PET, including research with new PET radiopharmaceuticals and the advent of integrated PET/CT scanners, will serve to keep PET at the forefront of lung cancer imaging in the future.
Footnotes
For correspondence or reprints contact: Matthew Acker, BHSc, Department of Nuclear Medicine, Queen Elizabeth II Health Sciences Centre, Room 3352, Halifax Infirmary Site, 1796 Summer St., Halifax, Nova Scotia, Canada, B3H 3A7.
E-mail: mracker{at}dal.ca
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH JUNE 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}