


Abstract
Technologists working in nuclear medicine departments in sub-Saharan African countries do not have access to formal training in nuclear medicine and have been recruited mostly from related fields of radiologic technology. Because of the nature of the specialty, the numbers that require training are small, and it is therefore not cost-effective for higher-education institutions in these countries to set up training programs. There is also a lack of expertise in this field in Africa. Assessing the feasibility of running a distance assisted training program to provide training where none exists was undertaken as part of a project sponsored by the International Atomic Energy Agency and the African Co-Operative Agreement for Research, Development, and Training related to Nuclear Science and Technology. Seven countries were nominated, but only 3 centers in 2 countries, Sudan and Tanzania, had the infrastructure to support training. Twenty-one students received the first modules in November 1999, and 13 completed the course in December 2001. All students except one were examined in their own departments. Students received an IAEA Certificate of Achievement at the end of the course, at which time the program was evaluated. Analysis of the data indicated that the conceptualization and design of the material were excellent. There were, however, some problems with the implementation of the program, notably the lack of preparedness of the supervisors, limited departmental resources, and a range of nuclear medicine investigations inadequate for clinical competency. The course was seen to have a positive impact, as it not only allowed technologists to develop skills necessary for the profession but also encouraged critical thinking, reflection, and problem solving. One third of untrained nuclear medicine technologists working in sub-Saharan Africa have now received cost-effective, structured on-site training.
The intergovernmental organization African Co-Operative Agreement for Research, Development, and Training related to Nuclear Science and Technology (AFRA) comprises 27 member states and is a branch of the International Atomic Energy Agency (IAEA). Its aim is to fully exploit regional capabilities by facilitating collaboration and technical cooperation among developing countries. Although resources in Africa are limited, 18 member states do engage in nuclear medicine activities.
The IAEA has helped to establish nuclear medicine departments in African countries that are signatories to the African Regional Agreement. This has created a need for qualified personnel in all categories of multidisciplinary nuclear medicine practice, particularly nuclear medicine technologists. Only 5 countries (Algeria, Egypt, Morocco, Tunisia, and South Africa) have established training programs for nuclear medicine technologists (Fig. 1). South Africa is the only country offering a de novo course in nuclear medicine technology; in the North African countries, nuclear medicine is offered as a component of a related qualification. The greatest need for training is in the sub-Saharan countries that have no indigenous training. The lack of structured training led the IAEA to support fellowship training for short periods outside the countries, causing a loss of departmental personnel during the fellowship and, in many instances, a permanent loss afterward as many of the trained staff emigrated. To reach as many untrained technologists as possible, an IAEA project was planned using the concept of distance training.

Distribution of countries in Africa with training programs for nuclear medicine technologists.
PILOT STUDY
Course material for a distance assisted training (DAT) program was developed in Australia under the auspices of the IAEA and sponsored by the Australia Agency for International Development. The course was initially tested in countries of Asia belonging to the Regional Cooperative Agreement for Research, Development, and Training Related to Nuclear Science and Technology in Asia (RCA). The design of the training material was such that it could be used either for coordinated in-service training or as a formal training course. Subjects were grouped into modules allowing for a logical learning sequence covering basic sciences and clinical applications of nuclear medicine techniques. Clinical applications were arranged progressively from static planar imaging to more complicated emission CT.
The Anglophone countries in Africa with nuclear medicine facilities were invited to participate in the pilot study, which was coordinated from the Groote Schuur Hospital campus of the Peninsula Technikon, Cape Town, South Africa, as that hospital had expertise on training programs for nuclear medicine technology. Seven countries applied to be included in the pilot study. Precourse teams were sent to these 7 countries to assess whether the nuclear medicine facility had the infrastructure and capacity to support the training. Only 3 of the 7 countries had centers that could be included in the pilot study. The criteria for inclusion were that the departments have a functioning γ-camera with associated computer, a dose calibrator, a laboratory area designated for working with radioactive materials, survey meters, access to a probe or well counter, a regular supply of radionuclides, and the availability of essential nonradioactive kits. The final participating centers and student numbers at the start of the course are shown in Table 1. The participants were qualified mostly in related fields of radiologic technology, except for 1 participant who was qualified in medical laboratory technology and 1 who had a science degree. English was the second language of all participants. The first language was Shona for 1 participant, Swahili for 2 participants, and Arabic for all others.
Participating Locations and Students
After completion of the first module, the course in Zimbabwe was discontinued because of γ-camera breakdowns and cessation of radiopharmaceutical supply. The economic problems in that country had resulted in a lack of foreign currency to purchase 99mTc generators. Thus, a continuing nuclear medicine service could not be guaranteed and the practical objectives of the course could not be met. The center in Harare sent 1 student to Cape Town on a fellowship to complete the course there.
The aim of the pilot study was to determine the feasibility of using the DAT program for nuclear medicine technologists in Africa, to develop criteria for future use of DAT in the region, and to compare the cost-effectiveness of DAT with that of training outside the country.
Students completed the basic course of 7 modules (approximately 216 h of study and 84 practical exercises) in 2 y. Modules were distributed in sequence as hard copies. All students attended a midcourse workshop held in Cape Town, South Africa, and were assessed continually with workbooks and end-of-module assignments. Final practical assessments took place in the students’ own departments. All students received an IAEA Certificate of Achievement.
Program Limitations
The training program was hoped to establish a basic standard of professional practice in developing countries; however, the unique problems of Africa had to be considered. Debt and resulting health budget cuts in Africa lead to constraints in the nuclear medicine service that individual countries can provide. Most countries in Africa, with their limited resources for health, consider primary health care a priority and nuclear medicine a tertiary health care service, and nuclear medicine languishes in many because of lack of equipment, specialists, and training programs (1). The lack of expertise in maintenance of equipment causes camera downtime and interruption of service. Radionuclides essential to nuclear medicine practice can be imported only from South Africa or Europe, and countries not on a direct flight path experience delivery problems exacerbated by poor customs handling at the country of destination. During the program, poor telecommunications limited the ability of the coordinator in South Africa to provide support; all study materials had to be sent by courier, as the postal systems were unreliable. Nuclear medicine practice is not well known by the medical community in Africa, and referral patterns therefore do not offer the student the range of investigations needed to establish good practice. Students lack support by medical physicists and radiopharmacists.
Program Evaluation
A questionnaire was sent to both students and supervisors as an end-of-program evaluation. The same questionnaire was used in the Asian countries, which provided data for comparison. Although efficient when used in large numbers, questionnaires are lacking in that they obtain only broad information. Therefore, 2 types of question were asked: those requiring a ranked response and those requiring a free-form response. For the ranked responses, participants responded to a statement using the Rensis Likert scale (2): strongly disagree, disagree, agree, strongly agree, or don’t know. These data were captured and analyzed quantitatively. The free-form responses, in contrast, required participants to answer an open-ended question in their own words. These answers were analyzed qualitatively and, together with transcripts from interviews of 2 students and 1 supervisor, provided more-detailed feedback.
Four basic questions needed to be addressed to evaluate the process, outcome, and efficiency of the pilot study (2): Did the concept and design of the DAT program meet the needs of the beneficiaries? Was the DAT program implemented in Africa in a way that ensured future sustainability? What did the impact and outcomes of the pilot study reveal about the relative success of the program? Were the outcomes achieved most cost-efficiently?
While asking these questions, the survey also explored the extent to which the perceived challenges in this type of work-integrated learning (3) affected the program as a whole. The first of these challenges was cost-effectiveness; the concern of the evaluation was the quality of the learning experience and the extent to which it helped the learners develop into reflective practitioners (4). A second challenge was control, because of the higher risk of unpredictability when distance learning takes place in a variety of settings. The role of the supervisor as a resource (5) is important in ensuring a stable process rather than a fixed outcome (6). Mapping the type of supervision offered was necessary to gauge its effectiveness. A third challenge was collaboration across occupational and organizational boundaries (7) by the IAEA, the DAT management team, regional coordinators, hospital management, and national bodies. A fourth challenge was capacity: Did the educative potential of the workplace match the needs of the learner and the curriculum? Were there sufficient equipment, radiopharmaceuticals, and patient referrals? A final challenge was customization with regard to the experience and social positions of the learners (8). Mapping the participants’ profiles was important in discovering whether their educational backgrounds had prepared them for learning in this way. Home language was an important issue because all students completed the course in a second language.
RESULTS
The results of the rated responses to statements on the questionnaire showed that overall, both students and supervisors had a positive opinion on the concept and design of the DAT course.
Seventy percent of students (n = 7) strongly agreed that the course added value to their original qualification. Ninety percent (n = 9) responded positively to the statement that the course material had helped them to develop professional skills needed in the field of nuclear medicine, and 80% (n = 8) strongly agreed that the course material had encouraged them to reflect on their clinical practice and to work independently.
Supervisors were even more strongly positive, perceiving that the course was well designed and well organized and encouraged students to reflect on their clinical practice. Supervisors believed that the material helped students to link theory to practice and that the workbooks and presentation of materials at workshops greatly assisted student learning.
Figure 2 compares the distribution of the rated responses from students and supervisors. Statements on issues of course design, implementation, and impact were grouped, and the mean scores for 10 students and 3 supervisors are shown in the figure. The rated responses were scored as follows: strongly agree = 4, agree = 3, disagree = 2, strongly disagree = 1, and don’t know = 0.
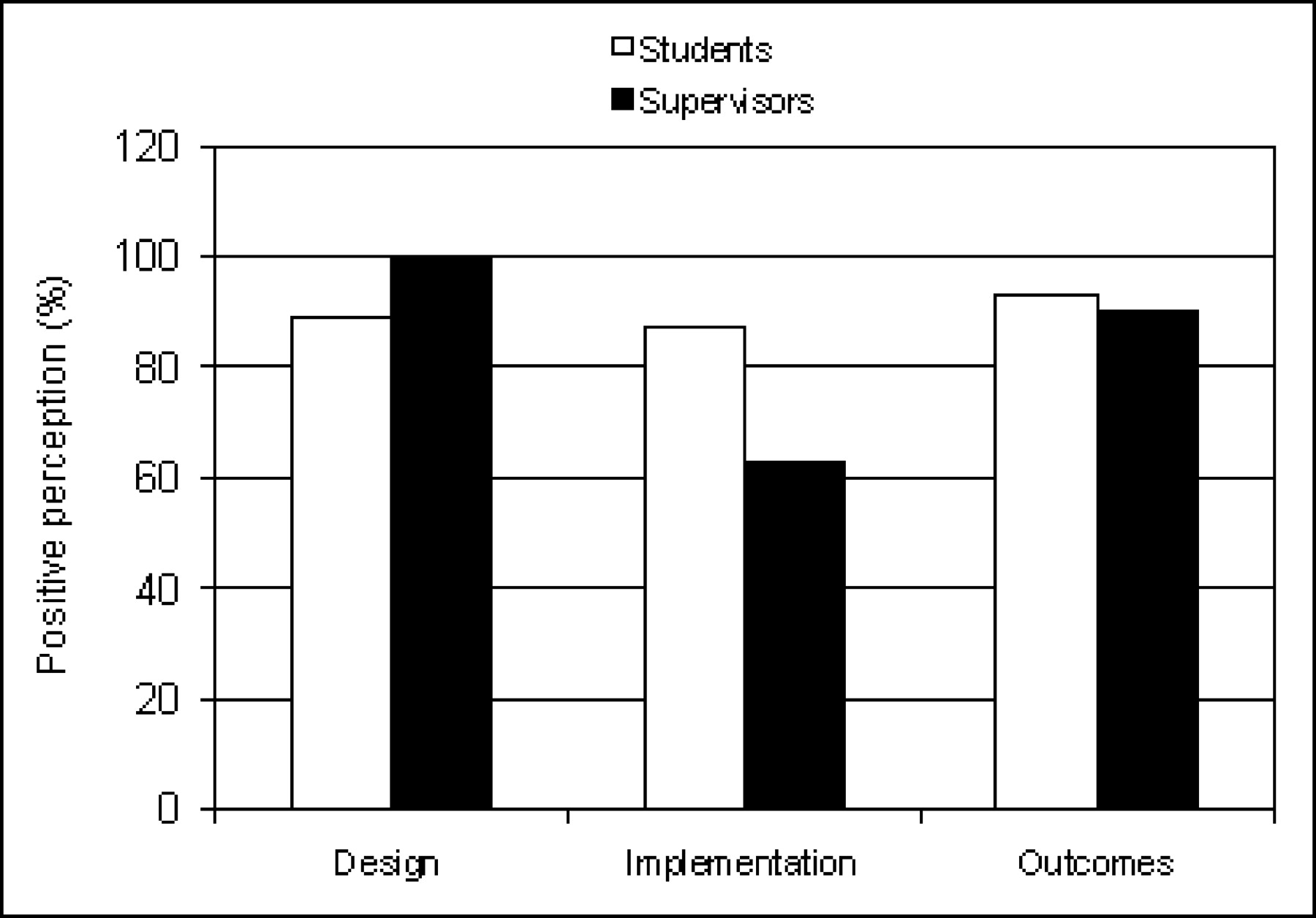
Student and supervisor perceptions of the design, implementation, and outcomes of the DAT program in Africa.
DISCUSSION
The concept of the course was commendable, offering nuclear medicine technologists who did not have a qualification the opportunity, which would not otherwise have existed, to study and acquire professional skills within their own departments in their own countries. The educational gains were evident from the test scores, with half the students scoring >80% and only 1 student scoring <60%. The aims of the course to provide training where none exists and to improve quality were therefore met. However, successful participants in the program received a certificate of achievement from the IAEA and not a recognized qualification. Thus, parity of esteem (9) with a higher-education qualification becomes an issue. The certificate does nonetheless provide a basis for a competency standard for nuclear medicine practice not only within Africa but also throughout the developing world. Because the IAEA is regarded highly by the countries of Africa, regulatory bodies might recognize or accredit the certificate. The participants in Tanzania were promoted on the strength of the certificate awarded.
Both the content and the design of the course were highly acclaimed by all participants. The structure and style effectively enabled learning and skill development essential to the profession. The constructivist-orientated (10), self-directed learning approach (11,12) cultivated reflective practitioners (4) and introduced them to nuclear medicine of an international standard. The downside of this approach was student frustration with the limited resources of their departments, despite the fact that the course materials had been designed for less developed countries and, whenever possible, had provided alternative perspectives to accommodate all situations.
The nuclear medicine physicians who acted as supervisors played a key role, providing a human resource (5) for the students. Supervisors were available for consultation when needed, assisting and generally facilitating the learning process. The inherent weakness of this type of corridor mentor (10) approach was that regularly scheduled meetings and tutorials for extra support were not planned but only ad hoc. The supervisors were extremely busy and willingly undertook this task in addition to their normal workload.
Necessity of Collaboration
Although an objective of the pilot study was to empower countries to develop their own indigenous training, the lack of significant infrastructure for this small specialty in sub-Saharan Africa necessitates the support of international organizations such as the IAEA. Assistance is needed to establish the network for conducting the course, and projects eligible for grant funding need to be identified. Because of the lack of resources and expertise in the region, countries with greater strength in these areas need to coordinate and assess the courses.
Workshops were an important and integral part of the DAT program and provided students with the opportunity to interact with cohort learners. As with any distance learning program in which students are apart from instructors, students benefit from this type of social and integrated process of learning (13).
The impact of the pilot study alone is that one third of untrained nuclear medicine technologists working in sub-Saharan Africa have now received structured on-site training. They have joined the more than 400 students in 24 countries across 3 continents who have been trained in this way, thus bringing Africa in line with international standards. The cost of producing the learning material aside, training was more cost effective by distance than by sending students outside the country: $6,533 average cost per distance student versus $18,841 for a student completing a fellowship in Cape Town. Nuclear medicine departments benefited because the training did not result in loss of staff. Improved nuclear medicine service of an international standard will ultimately benefit patients.
Comparison with Pilot Study in Asia
The questionnaire was also circulated to participants of the DAT program in the RCA region. Although the numbers surveyed in Asia were far higher that those surveyed in Africa, similar recurring themes emerged. The forms were returned by 11 coordinators, 59 supervisors, and 158 students, and the response ratings had a similar spread, as shown in Figure 3. Overall, participants responded more positively on the concept, design, impact, and outcomes of the course and slightly less positively on implementation.

Student, supervisor, and coordinator perceptions of the design, implementation, and outcomes of the DAT program in Asia.
Analysis of the free-form responses from the Asian study showed recurring themes similar to those revealed by the AFRA survey. Factors enabling learning were the content, design, and layout of the course, as well as the workbooks and workshops. Prior experience in nuclear medicine added to student success, and a desire for an international standard was a motivating factor.
Barriers to learning included limited resources, studies not done in the home departments, and lack of work relief for students and supervisors. The concept of self-directed learning (11,12) presented some difficulties, as students were used to the more traditional teaching methods. As in Africa, the supervisor was a key individual in the process and needed to be better prepared. Language was less of a difficulty for students in Africa than for students in some Asian countries, as English was the second language or language of higher learning (14) in the African countries.
Positive feedback on student performance and attitude indicated that what the students learned benefited the nuclear medicine service.
The Way Forward
With the efficacy and cost-effectiveness of the DAT program now having been shown, it remains to be seen whether training of nuclear medicine technologists is sustainable in Africa. The role of the IAEA in many African countries is crucial because of their poor socioeconomic situation. However, the focus of IAEA projects has shifted from capacity building to problem solving, limiting their involvement in future training programs. Once the existing nuclear medicine personnel have been trained, it will be up to the countries themselves to consider how they will train technologists in the future. This training will require a national commitment, and whether training is ad hoc or continuous will depend on the individual needs of each country. The complete training package, including assessment materials and instructions, is freely available to the member states. The DAT program offers an infrastructure that gives the countries an opportunity to sustain training as well as a benchmark for standardization of training. Countries with a continued acute shortage of personnel will still need support from neighboring countries that have the resources and expertise.
It is encouraging that in Algeria, the course has been fully adopted as the national standard for training of all nuclear medicine technologists.
CONCLUSION
There is a pressing need to tackle current and emerging health challenges, both in general worldwide and in particular in Africa. Most governments in Africa focus on primary health care and treatment of infections. Because of the poor socioeconomic situation in most African countries, nuclear medicine facilities are either nonexistent or not funded sufficiently. Nuclear medicine has the potential to benefit health care but has a low priority. Africa is the only region in the developing world with poorly developed nuclear medicine facilities, having only islands of expertise in some areas of the continent. The advantages of nuclear medicine are well established, and there is a drive to fully integrate nuclear medicine techniques into health care to benefit the people of Africa. To this end the commitment of the IAEA to train nuclear medicine personnel, and specifically nuclear medicine technologists, is an important priority. The DAT program is an efficient tool for building the capabilities of nuclear medicine technologists within the AFRA member states. One third of the previously untrained nuclear medicine technologists in Africa have now benefited from this method of training.
Acknowledgments
I am grateful to Peninsula Technikon and Groote Schuur Hospital for endorsing and supporting my involvement in this AFRA/IAEA project, particularly Mokdad Maksoudi, the regional projects coordinator at the IAEA. Input from the AFRA task force helped sustain the project, which could not have succeeded without the motivation and commitment of the students themselves and their supervisors. I acknowledge the interregional support and encouragement of Heather Patterson (DAT coordinator), Brian Hutton (project manager) in Australia, and Margarita Nunez (regional coordinator of the Latin America and the Caribbean Cooperative Agreement) in Uruguay and specially thank my colleague Pat Freedman, who accompanied me on expert missions and assisted with the final assessments.
Footnotes
For correspondence or reprints contact: Geraldine M. Philotheou, M Tech (Rad), Department of Nuclear Medicine, Groote Schuur Hospital, Cape Town, South Africa.
E-mail: gmp{at}curie.uct.ac.za





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.