


Abstract
Objectives: In diabetes, extended adrenergic receptor stimulation with hyperglycemia and insulin deficiency is associated with cardiac autonomic dysfunction. Clinically evident diabetic cardiac autonomic neuropathy (CAN) is associated with a poor prognosis. Research studies indicate that autonomic function tests, which are traditionally used to diagnose diabetic CAN, are less sensitive than 123I-metaiodobenzylguanidine (MIBG) imaging, particularly in the early stages of the disease. This established imaging technique makes use of the noradrenaline analog MIBG, which is radiolabeled with 123I to assess the noradrenaline uptake-1 mechanism of the sympathetic nervous system. Although scintigraphic studies indicate that long-standing cardiac autonomic dysfunction is permanent, some authors have shown partial reversibility with early metabolic intervention. 123I-MIBG imaging could therefore have an important clinical role to play in the early diagnosis and treatment monitoring of diabetic CAN.
Methods: A PubMed/MEDLINE Internet search was performed using MIBG, diabetes, and cardiac autonomic neuropathy as key words.
Conclusion: The general expense of 123I-MIBG imaging, together with the lack of commercial availability of this radiopharmaceutical in the United States, has limited the clinical use of this technique. As such, the clinical role of 123I-MIBG imaging in the early diagnosis of diabetic CAN has yet to be validated and defined in most regions of the world, and further study is required.
Cardiac autonomic neuropathy (CAN) is a common complication of diabetes and is associated with resting tachycardia, postural hypotension, painless myocardial ischemia or infarction, arrhythmias, and sudden cardiac death (1). It is believed that the progression of CAN can be halted and perhaps even reversed with early metabolic intervention (2–4). In clinical practice, CAN is most commonly assessed by indirect autonomic function tests, which are believed to underestimate early autonomic dysfunction (3,5). 123I-Metaiodobenzylguanidine (MIBG) imaging is a direct, noninvasive in vivo method of assessing autonomic function, allows for objective semiquantitative assessment (5), and has been shown to detect diabetic CAN even in the early stages of the disease (6). This technique has been widely used in research to assess diabetic CAN but, with the exception of Japan, has had limited clinical use.
This paper reviews the relationship between diabetes and CAN to establish the importance of early diagnosis. 123I-MIBG imaging in diabetic CAN is also reviewed, highlighting the advantages and disadvantages in comparison with other diagnostic techniques. Obstacles that have inhibited the widespread clinical implementation of this technique are discussed to possibly explain the disparity between clinical use in Japan, Europe, and the United States, and areas of possible future study are identified. Publications were identified by a PubMed/MEDLINE Internet search using MIBG, diabetes, and cardiac autonomic neuropathy as key words.
CARDIAC SYMPATHETIC INNERVATION
The autonomic nervous system, which includes the parasympathetic and sympathetic systems, plays an important role in the regulation of myocardial function, heart rate, and myocardial blood flow (7). The sympathetic system innervates the myocardium via sympathetic nerve fibers that traverse the subendocardium along the path of the coronary vessels, from the base to the apex of the heart (6,8). Noradrenaline (norepinephrine) is the main neurotransmitter of the sympathetic nervous system, and activation of this system or an increase in catecholamine level results in an increased heart rate (chronotropic effect), enhanced contractility (inotropic effect), and improved atrioventricular conduction (dromotropic effect) in the normal heart (6,9). Noradrenaline is synthesized from tyrosine in adrenergic neurons and is stored in membrane-bound adrenergic granules (10). During neurotransmission, the granule contents are discharged by exocytosis (10). Noradrenaline binds to postsynaptic β1-receptors located mainly in the synaptic cleft (6). The neuronal uptake-1 mechanism is the sodium- and energy-dependent homeostatic system responsible for reuptake of noradrenaline (6). Extended increased stimulation of cardiac adrenergic receptors results in desensitization and downregulation of the receptors, as well as increased receptor degradation and decreased receptor synthesis (6,9).
PATHOPHYSIOLOGY OF CAN IN DIABETES
The sympathetic nervous system is stimulated in the early stages of diabetes (6,11), and extended exposure of the adrenergic receptors to increased catecholamine levels, together with hyperglycemia and insulin deficiency, is believed to cause diabetic CAN (6). The advent of direct imaging techniques, including 123I-MIBG scintigraphy and PET neurotransmission studies, has allowed researchers to explore the natural progression of diabetic CAN.
123I-MIBG AND THE SYMPATHETIC NERVOUS SYSTEM
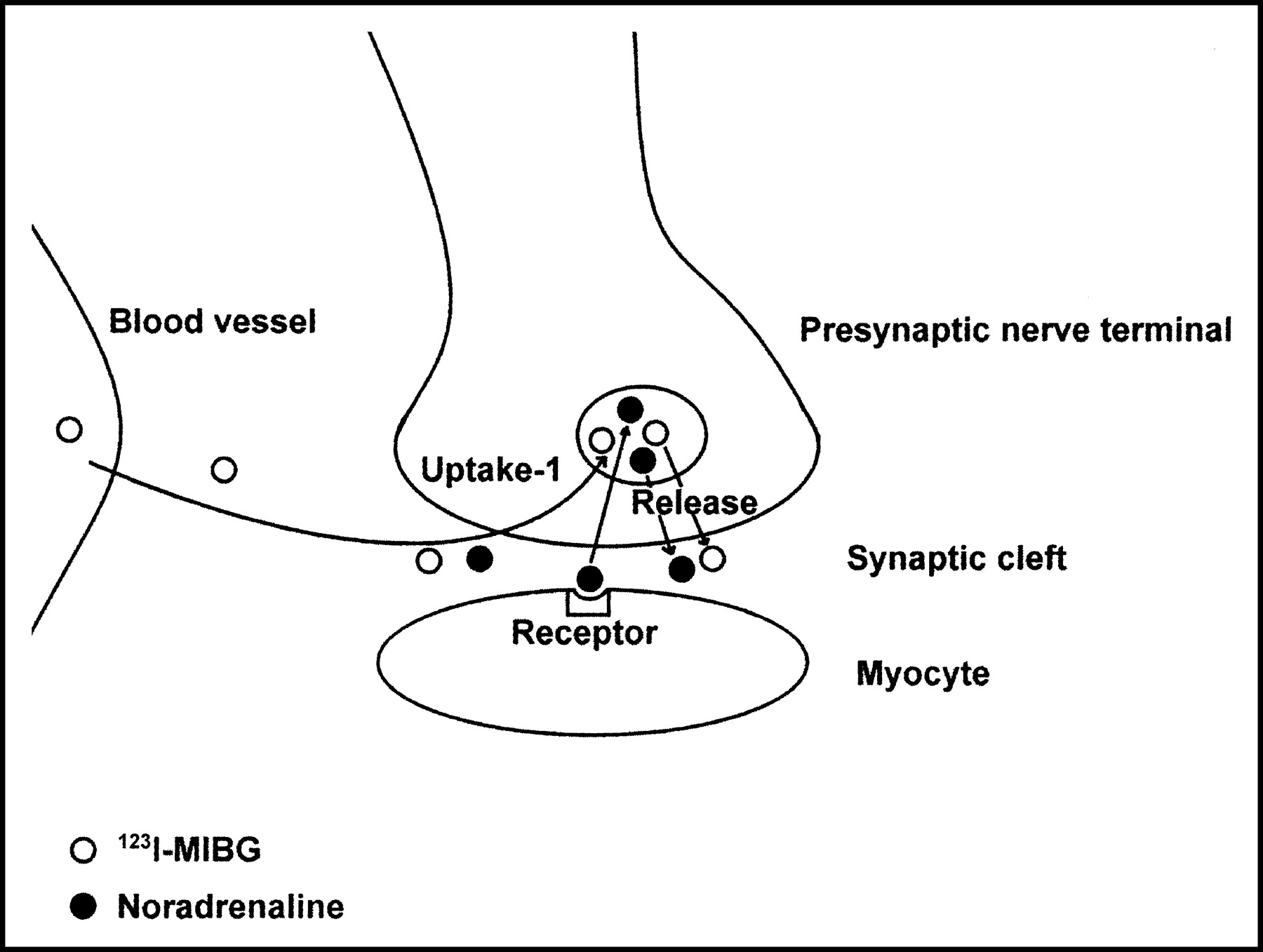
MIBG is a noradrenaline analog that is produced through a modification of guanethidine (9) and is labeled with 123I to allow for imaging. 123I-MIBG presynaptic neuronal uptake is predominantly through the uptake-1 mechanism (Fig. 1) (6,11). Although studies have shown that nonneuronal uptake (uptake-2 mechanism) of 123I-MIBG by the myocardium is not significant (12), this uptake mechanism has been shown to be significant at high plasma 123I-MIBG concentrations, likely because of passive diffusion (6). However, the uptake-1 mechanism predominates in 123I-MIBG imaging because of the small quantity of 123I-MIBG injected (6). The normal heart has dense sympathetic innervation and shows good uptake of 123I-MIBG (6). 123I-MIBG does not undergo intracellular metabolism (7). However, studies have shown that 123I-MIBG follows the same active uptake, storage, and release pathways as does noradrenaline. Thus, quantitative 123I-MIBG imaging is believed to allow assessment of global and regional sympathetic integrity by measurement of uptake, and assessment of function by measurement of washout (10,13).
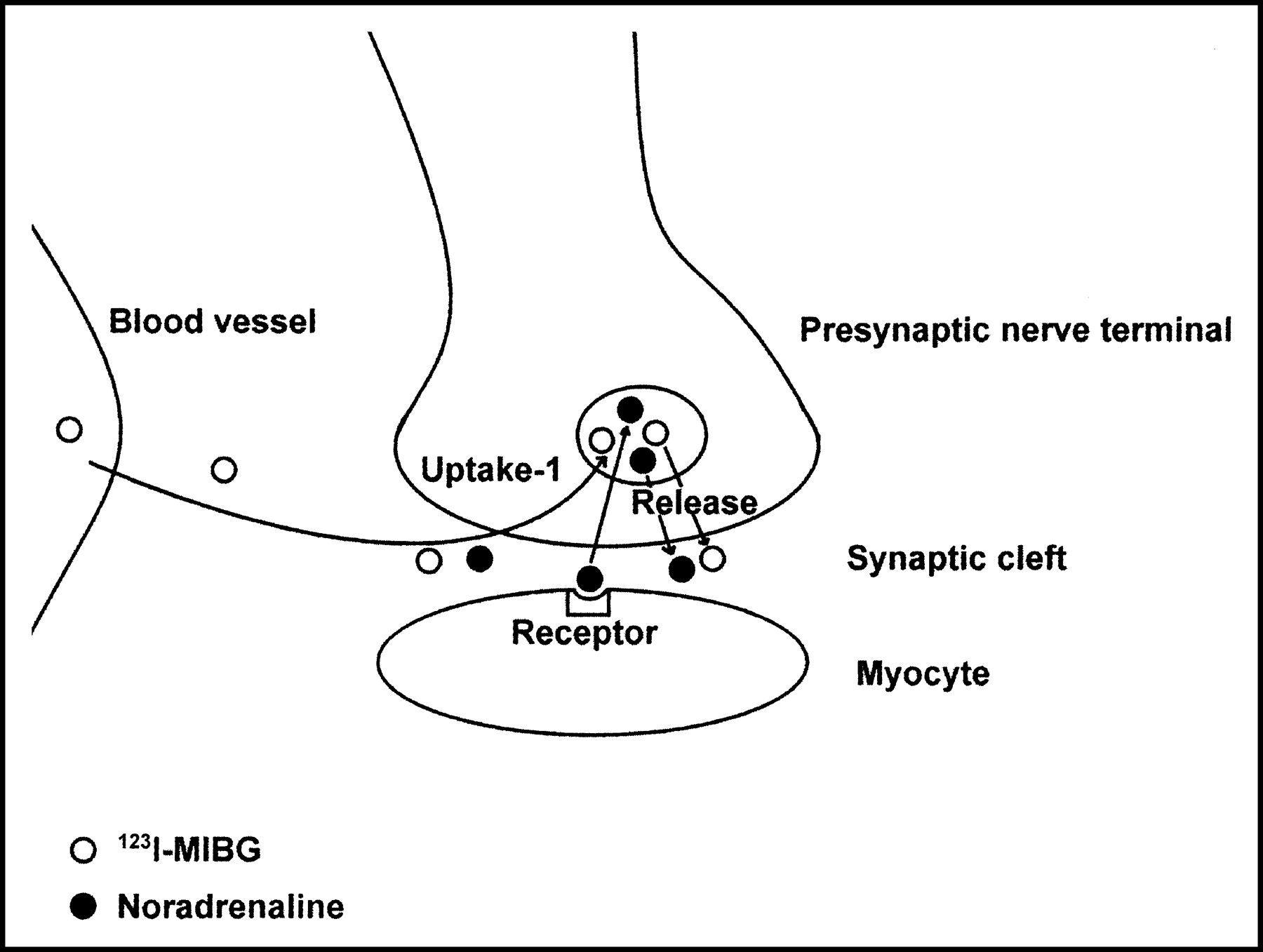
Schematic representation of the 123I-MIBG uptake mechanism.
PHARMACOLOGIC INTERACTIONS WITH MIBG
Studies have shown that some medications and physiologic states interfere with the biodistribution of 123I-MIBG (10). Cocaine and the tricyclic antidepressant desmethylimipramine specifically inhibit the type-1 catecholamine reuptake system and have been shown to reduce 123I-MIBG uptake (10,14). Although conventional α- or β-blocking medications do not affect 123I-MIBG uptake, there is evidence that labetalol, which has combined α- and β-adrenergic receptor-blocking properties, reduces 123I-MIBG uptake and may cause release of 123I-MIBG from neurosecretory vesicles (14). Reserpine depletes endogenous catecholamines from granular stores by blocking uptake and has been shown to reduce uptake and increase washout of 123I-MIBG (10,14). Phenylpropanolamine and related sympathomimetics displace intracellular stores of catecholamines and may compete for uptake with 123I-MIBG (10). Hypoglycemia results in a central nervous system-mediated discharge of catecholamines and has been shown to produce rapid washout of 123I-MIBG (10). Because exocytosis is dependent on calcium flux, calcium channel blockers may reduce the neuronal release of 123I-MIBG (10). Reduced 123I-MIBG uptake may be seen with high circulating catecholamine levels as a result of competition for the type-1 uptake mechanism (10). Platelets have an active amine uptake mechanism, and platelet uptake has been reported (10); however, in the literature reviewed, no problems associated with cardiac imaging have been documented.
123I-MIBG CARDIAC IMAGING
Standard Protocol
The standard protocol for 123I-MIBG cardiac imaging requires that drugs that interfere with 123I-MIBG uptake be withheld. A comprehensive listing of prescription and over-the-counter drugs that interfere with 123I-MIBG biodistribution, and the time for which they should be withheld, has been published (14). Thyroid uptake of unbound 123I is blocked with 500 mg of potassium perchlorate given orally 30 min before 123I-MIBG injection (6).
Between 148 MBq (7) and 370 MBq (6) of 123I-MIBG are injected intravenously at rest. Both planar and SPECT images are acquired 15 min after injection (early) and 4 h after injection (delayed). A 20% window is usually centered over the 159-keV photopeak of 123I for imaging (6). Anterior and 45° left anterior oblique planar images of the chest are acquired using a 128 × 128 matrix (6). SPECT images are acquired using a 64 × 64 matrix over 180°, from the right anterior oblique position to the left posterior oblique position (6). Planar imaging allows for global assessment of cardiac innervation, whereas SPECT allows for regional evaluation (15). A recent study suggested that the use of a medium-energy collimator, rather than a low-energy collimator, for planar imaging may improve the quantitative accuracy and reliability of 123I-MIBG cardiac imaging (16) by reducing scatter from the 0.529-MeV photons that make up 1.4% of the disintegrations of 123I (13,16).
Other Techniques
Dual-isotope imaging techniques, using 123I-MIBG and 99mTc-sestamibi or 201Tl, that allow 123I-MIBG quantitative analysis to be corrected for the presence of perfusion defects have been described (17–20). These techniques add to the diagnostic value of the study by excluding or compensating for coronary artery disease as a mechanism of reduced uptake (15).
Normal Cardiac Uptake Pattern
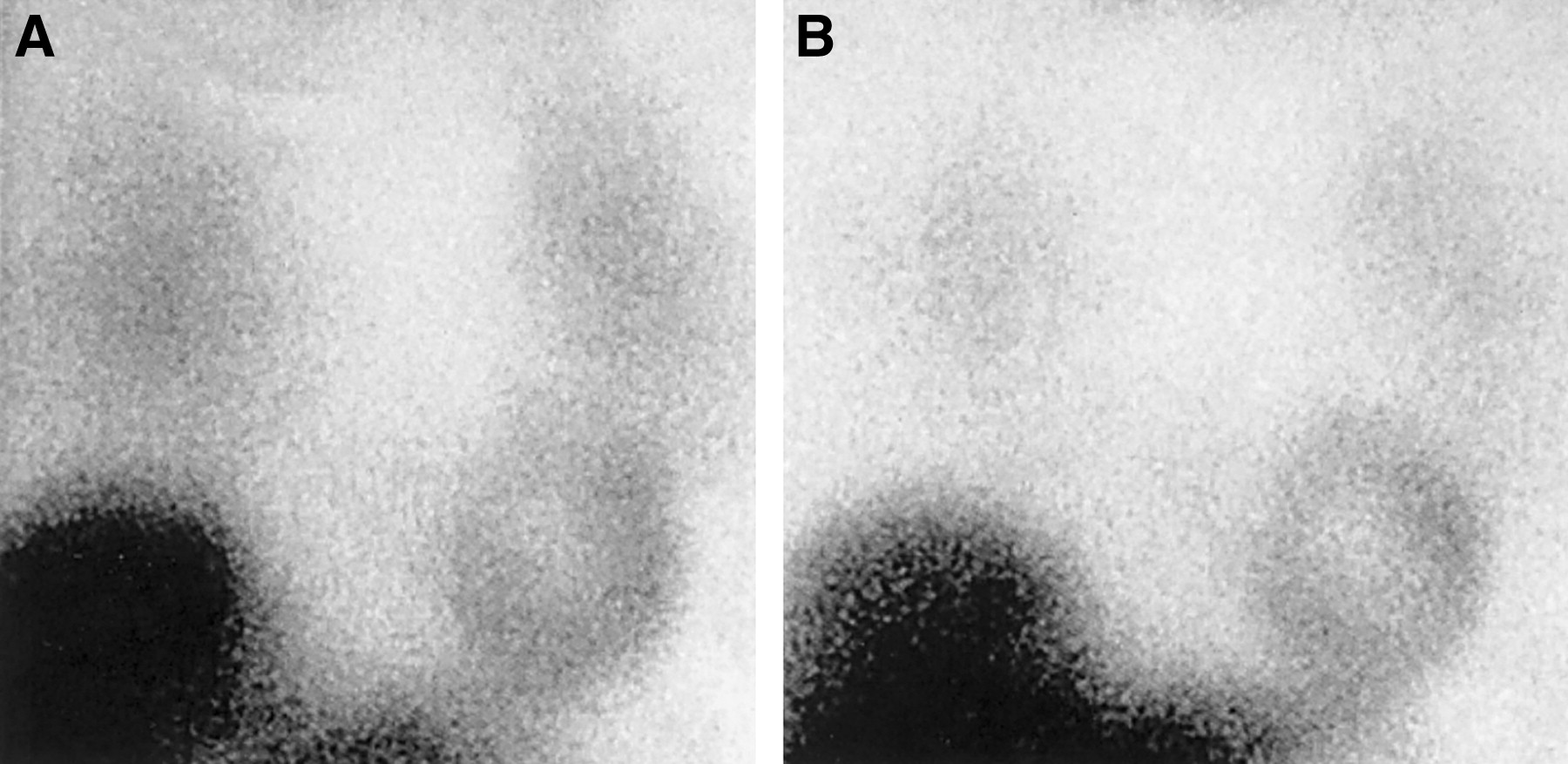
Healthy patients normally show good uptake of the radiotracer (Fig. 2). However, uptake may be heterogeneous and be slightly lower in the inferior wall (17,18), most likely because of attenuation (6,7). Activity may also be lower at the apex of the left ventricle than at the base because of the partial-volume effect (7) and, possibly, an imbalance of sympathetic and parasympathetic fibers (15). Homogeneous uniform uptake has also been reported (3). Cardiac function decreases with age, and decreased cardiac responsiveness to β-adrenergic stimulation is one of the most prominently seen changes (6). Decreased cardiac uptake has been shown in elderly patients, and age should likely be considered when assessing 123I-MIBG uptake (21).
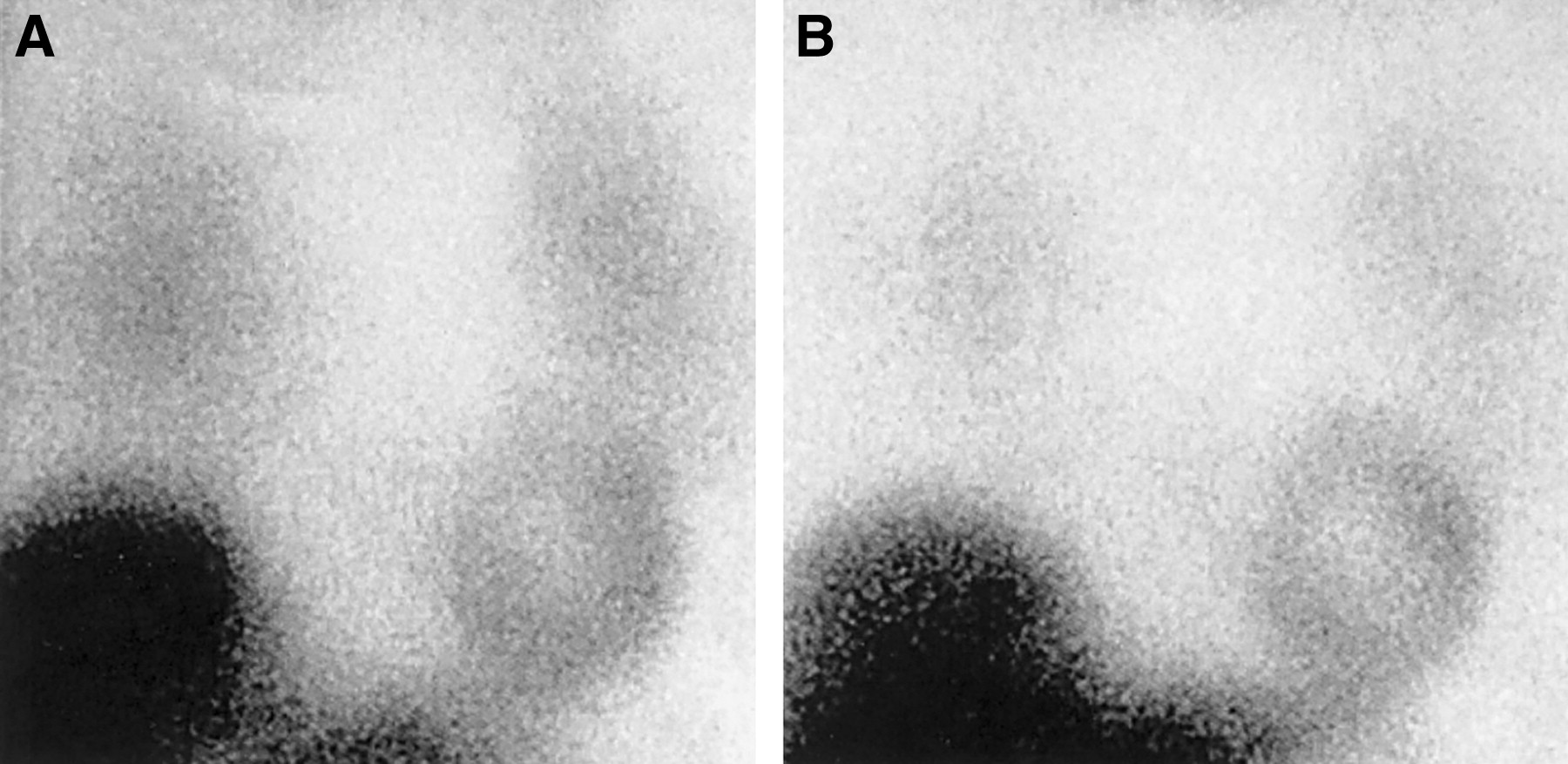
Normal 123I-MIBG uptake on early (15 min) planar images (A) and delayed (4 h) planar images (B). (Courtesy of Ignasi Carrió, MD, Barcelona, Spain.)
Image Markers
Cardiac 123I-MIBG uptake is commonly assessed by viewing the planar images (6). Initial uptake is considered to be a measure of the number and function of norepinephrine transporters in the heart (22). In addition, semiquantitative measures of uptake and washout have been used. The heart-to-mediastinum ratio is obtained from both the early and the delayed planar images (7) and is calculated by taking regions of interest over the myocardium in the anterior view and over the mediastinum in the left anterior oblique view and dividing the average counts per pixel in the myocardium by the average counts per pixel in the mediastinum (6). A high ratio is expected in normal hearts, indicating predominant localization of 123I-MIBG in the myocardium (7). Symptomatic autonomic neuropathy has been associated with profound loss of myocardial uptake (13,22). A recent review has reported an average heart-to-mediastinum ratio of 2.5 ± 0.3 for 96 healthy subjects (7). The washout rate is calculated from the decrease in myocardial counts between the early and the delayed images, normalized to the mediastinal counts (7). The washout rate is believed to reflect adrenergic activity, with increased adrenergic activity being reflected as increased washout (7). Average washout rates of 20% ± 10% have been found in healthy subjects (7). Although increased washout has been observed in diabetic patients (23,24), the clinical importance of this index in diabetes is not clear (25). Planar imaging has limitations, including the superimposition of surrounding structures on cardiac images, which may result in suboptimal images, and possible motion artifacts (6). SPECT overcomes some of these disadvantages (6).
The SPECT data are reconstructed along the short axis, horizontal long axis, and vertical long axis (6). SPECT images are analyzed visually, with regional uptake being scored on a point scale (6). Polar maps are generated from short-axis SPECT images and can be compared with known files of healthy patients (Fig. 3) (6). Studies have shown that sympathetic autonomic neuropathy normally presents in the inferior wall in the early stages of diabetic CAN and then progresses to adjacent segments (3,4,23,26,27). Regional myocardial evaluation using an inferior-to-anterior ratio may therefore be a sensitive index when assessing early diabetic CAN (23). To improve image noise and contrast with SPECT, the dose and imaging time should be maximized (6). SPECT images may be suboptimal if uptake is severely reduced (6). Differing terminology has been used in the literature to describe the same myocardial region.
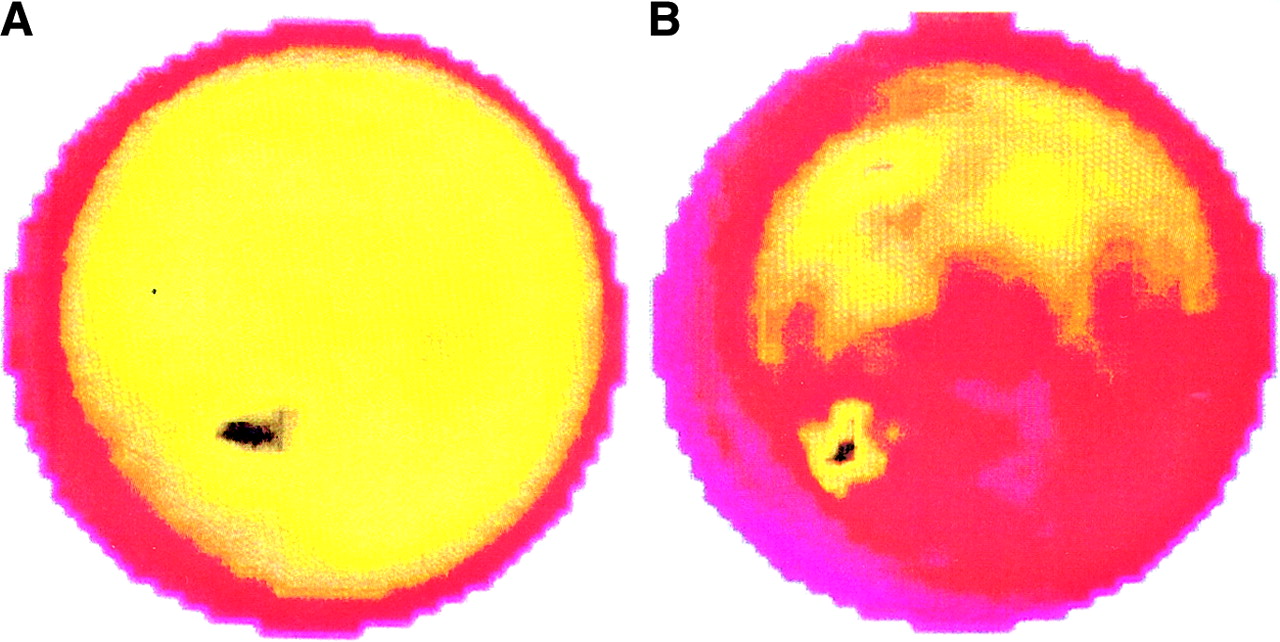
Polar map showing normal sympathetic innervation (A) and diabetic sympathetic dysfunction (decreased posterior/inferior uptake) (B). (Courtesy of Oliver Schnell, MD, Munich, Germany.)
Quantitative analysis by these methods is not absolute. With the advent of recent SPECT methods to correct attenuation, more accurate quantification may be possible (6,7,28). Scatter correction may also be of value (6). Despite the factors complicating 123I-MIBG imaging, this technique is believed to reliably detect sympathetic nerve damage in CAN (22).
OTHER METHODS OF EVALUATING CAN
Electrocardiograph-based autonomic function tests have traditionally been used to assess CAN (5,11). These indirect bedside methods include the Valsalva maneuver, heart rate variability, heart rate response to standing, postural fall in blood pressure, and the sustained handgrip test (1,7). Assessed results rely on heart rate or blood pressure responses (20), and autonomic dysfunction is usually defined as an abnormal response to at least 2 of these maneuvers (5,17,29). These methods are noninvasive; however, research has shown that they likely underestimate CAN (5,7,27,29) and reflect changes in parasympathetic function with more sensitivity than they do changes in sympathetic function (7,30). Compared with 123I-MIBG imaging, autonomic function tests are believed to be less sensitive (5,7,11,27,29,30), are nonquantitative, and are unable to evaluate specific anatomic regions (3,11).
The noradrenaline spillover technique can infer noradrenaline release (sympathetic activity) in the heart by using a radioactive noradrenaline infusion and sampling the coronary sinus (6,31). This technique is invasive, requires cardiac catheterization, and is unable to differentiate between increased neuronal release and reduced neuronal uptake (6,31).
PET-based neurotransmission imaging techniques offer a noninvasive, direct, objective, and quantitative way to assess myocardial autonomic function using tracer kinetic modeling (6). Although these techniques are more technically demanding than 123I-MIBG imaging, they can provide more accurate quantitative information on neurotransmitter synthesis and transport, and on receptor density (6,7). However, the clinical utility of these indexes has yet to be determined. The need for an on-site cyclotron is a major factor limiting the routine clinical use of PET to assess autonomic function (31). 11C-Hydroxyephedrine, also an analog of noradrenaline, is commonly used in studies in the United States (32–34). PET research studies have confirmed 123I-MIBG findings in diabetic patients (15).
RESEARCH FINDINGS
The mechanism by which diabetic CAN causes silent myocardial ischemia, infarction, and sudden cardiac death is not fully understood (32) and has been linked to a variety of factors (14). Studies do, however, indicate that even early, preclinical, stages of CAN may be associated with cardiac sympathetic dysfunction that can impair the regulation of coronary blood flow in response to stress (32). This vascular dysfunction is thought to play a role in progressive left ventricular dysfunction in diabetic patients, even in the absence of angiographically assessed coronary artery disease (32). CAN has also been linked to an abnormal left ventricular response to exercise in the absence of ischemic heart disease; such a response may contribute to left ventricular dysfunction before the appearance of irreversible damage and overt heart failure (11,35). Diabetic patients with silent myocardial ischemia have been found to have 123I-MIBG uptake abnormalities suggesting a link between abnormal perception of pain and diabetic CAN (14,18). Stevens et al. (33) have suggested that proximal hyperinnervation together with distal denervation may be associated with arrhythmias and sudden cardiac death in diabetic patients.
Long-term poor glycemic control has been identified as a major factor in the progression of diabetic CAN (29). Small PET defects in myocardial innervation progress with poor glycemic control and regress with good glycemic control, suggesting that good glycemic control in patients with early cardiac denervation may prevent the development of cardiac sympathetic dysinnervation (4). Partial reversal of cardiac sympathetic denervation as scintigraphically assessed with 123I-MIBG has been shown in patients with newly diagnosed insulin-dependent diabetes mellitus after intensive insulin therapy (2), whereas patients with long-term insulin-dependent diabetes mellitus generally show neither progression nor regression of 123I-MIBG defects (3). Similar results are found in patients with non-insulin-dependent diabetes mellitus (36) after insulin therapy. These findings support the belief that diabetic CAN has a reversible metabolic component and an irreversible structural component, with the irreversible component increasing over time (2), and emphasize the importance of the early diagnosis of diabetic CAN.
Cardiac defects visualized with 123I-MIBG imaging of diabetic patients have been found to be approximately 40% more common than the detection of diabetic CAN by traditional means (7). 123I-MIBG defects may be associated with autonomic neuropathy, arrhythmogenicity due to abnormal regional flow (flow-demand mismatch), left ventricular dysfunction, and microvascular disease, even in the absence of macrovascular disease (7).
THE CLINICAL ROLE OF 123I-MIBG IMAGING IN DIABETIC CAN
Clinically evident autonomic neuropathy in diabetic patients is associated with a poor prognosis (1,37). The early preclinical detection of CAN that is believed to be possible with 123I-MIBG imaging (6,15,26) may thus have an advantage over the less sensitive indirect autonomic reflex testing that is traditionally used (3,5,27). The increased sensitivity of 123I-MIBG imaging over autonomic function testing may also make this method superior for evaluating the effect of metabolic intervention on CAN (29). These factors could permit more focused management of diabetic CAN (17). However, although widely used to characterize diabetic CAN and improve understanding of the natural progression of this disease process, 123I-MIBG imaging has seen routine clinical use only in Japan (7,28).
Although 123I-MIBG is commercially available in Europe, the cost of this procedure appears to have prohibited its clinical use, and 123I-MIBG imaging is used primarily for research in this region. The lack of commercial availability of 123I-MIBG and the high cost are important factors limiting use of this technique in the United States (7,28). 123I-MIBG is currently labeled on site, which requires an investigative new drug application, or is imported from Canada at greater expense (7).
From the literature reviewed, most 123I-MIBG research studies have been performed in Europe and Japan. Most studies have been of relatively few patients and limited to single centers. The largest study assessed 65 diabetic patients (17), but on average the reviewed studies assessed 28 patients. No cost analysis data were available in the literature reviewed.
CONCLUSION
123I-MIBG imaging appears to promise novel, noninvasive clinical information in the early detection of diabetic CAN. Indeed, this technique is used clinically in Japan. However, further clinical studies are needed if 123I-MIBG imaging is to see widespread clinical use in the United States. The clinical usefulness of this technique needs to be validated by large multicenter trials, and the proper positioning of 123I-MIBG imaging in diagnostic algorithms needs to be established (28). The development of 99mTc-labeled analogues of MIBG (noradrenaline), if feasible, could alleviate the cost and availability issues and lead to greater worldwide clinical use of this technique (6,28). Cost-analysis studies are needed to demonstrate the possible cost-effectiveness of this procedure when total patient outcome is considered (28). 123I-MIBG cardiac imaging continues to be a valuable research tool in diabetes. It remains to be seen whether the cost and availability of this technique will limit the work that still needs to be done to promote it to full clinical status in most regions of the world.
Footnotes
For correspondence or reprints contact: Lynda A. Scott, DipRad (D)(NM)(RT), 5204 Lenoraway Dr., Raleigh, NC 27613-1410.
E-mail: lynda.scott{at}earthlink.net
REFERENCES





{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- CARDIAC SYMPATHETIC INNERVATION
- PATHOPHYSIOLOGY OF CAN IN DIABETES
- 123I-MIBG AND THE SYMPATHETIC NERVOUS SYSTEM
- PHARMACOLOGIC INTERACTIONS WITH MIBG
- 123I-MIBG CARDIAC IMAGING
- OTHER METHODS OF EVALUATING CAN
- RESEARCH FINDINGS
- THE CLINICAL ROLE OF 123I-MIBG IMAGING IN DIABETIC CAN
- CONCLUSION
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics