


Abstract
A 47-y-old woman with chronic liver disease, who had previously undergone placement of a peritoneal venous shunt without ascites, presented with a chronic right pleural effusion. The first attempt at radionuclide injection resulted in an accidental small-bowel injection with consequent intraalimentarily induced nuclear small-bowel followthrough. I have not read of this interesting complication in the literature. She did not have a bowel obstruction. A repeated study 2 d later demonstrated an obstructed peritoneal shunt and right hemidiaphragmatic pleural leak best seen with the patient upright.
Peritoneography is an uncommon study and has been performed for evaluation of peritoneal shunt function and peritoneal leaks. I present a complication of peritoneography—accidental small-bowel puncture—that I could not find previously reported in the literature.
CASE REPORT
A 47-y-old woman with chronic liver disease, who had previously undergone placement of a peritoneal venous shunt without ascites, presented with a chronic right pleural effusion. Peritoneography was ordered to determine the location of a suspected right hemidiaphragmatic leak.
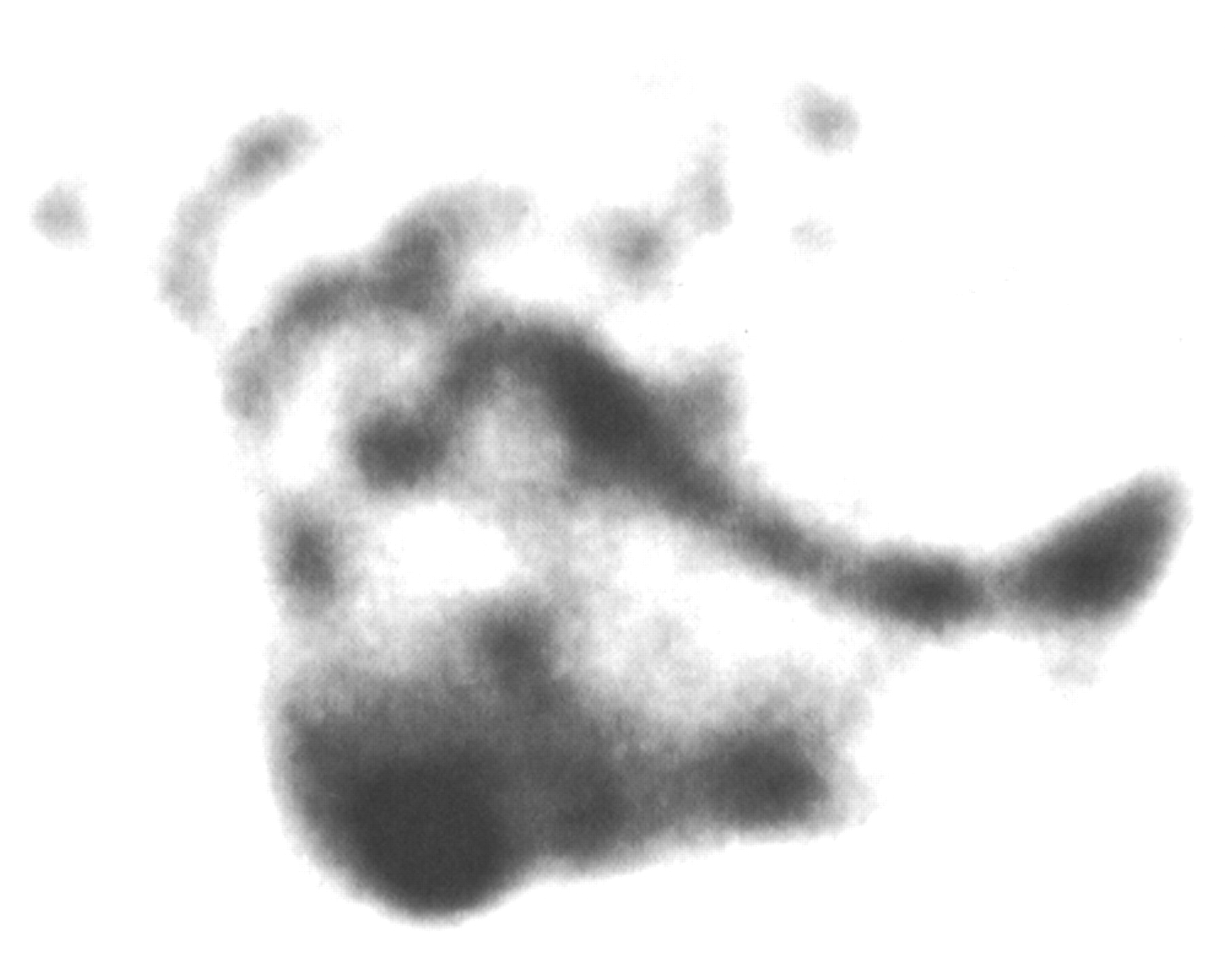
The patient was prepped in a sterile manner, and 37 MBq (1 mCi) of 99mTc-macroaggregated albumin (MAA) were injected into the abdomen at the midline below the umbilicus (1,2). The patient was rocked back and forth and immediately imaged. There was no peritoneal activity, but activity of a small-bowel–like pattern was present (Fig. 1). An accidental small-bowel injection had occurred. There was no evidence of peritonitis or gastrointestinal bleeding.

First 99mTc-MAA administration produces accidental small-bowel followthrough without intraperitoneal activity.
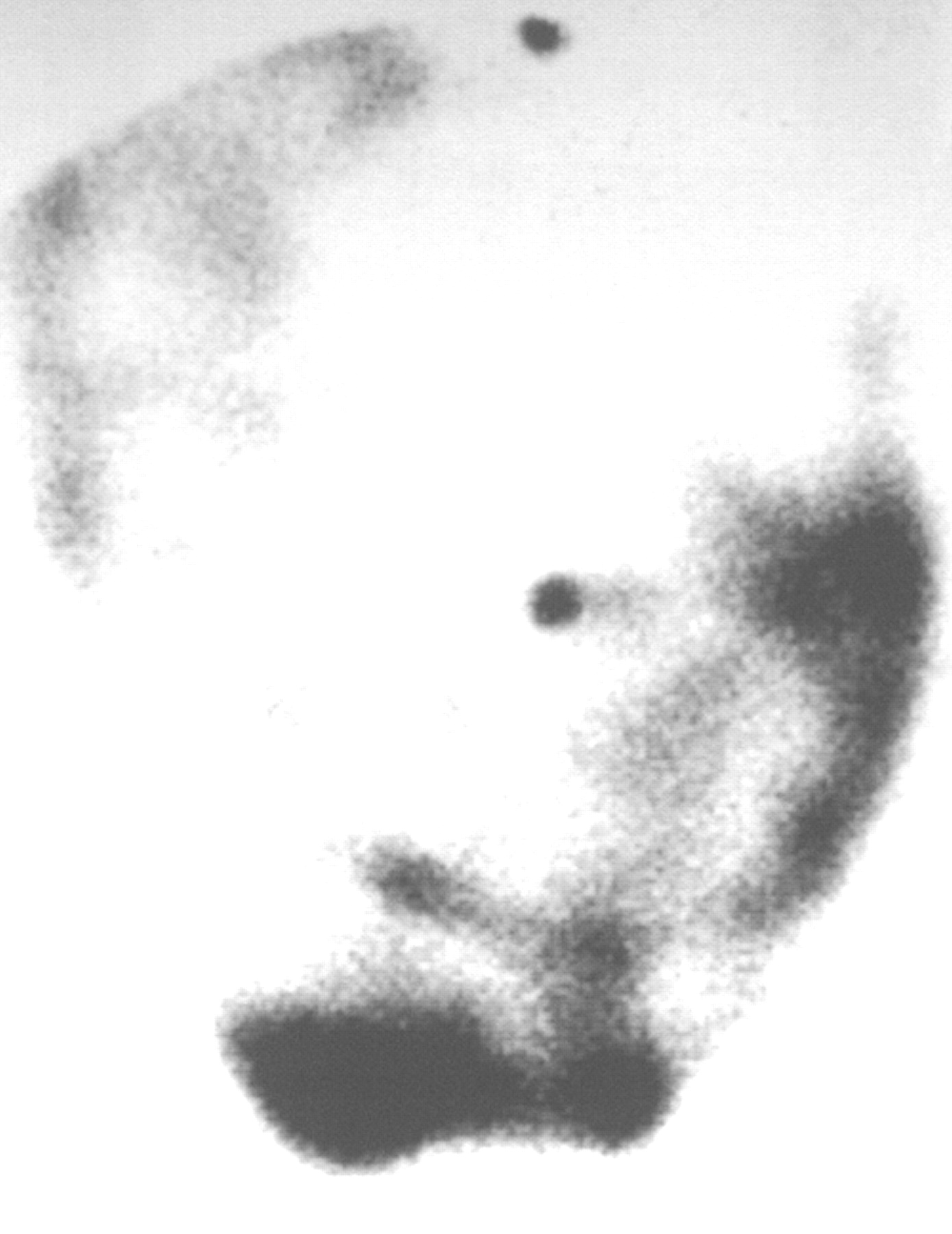
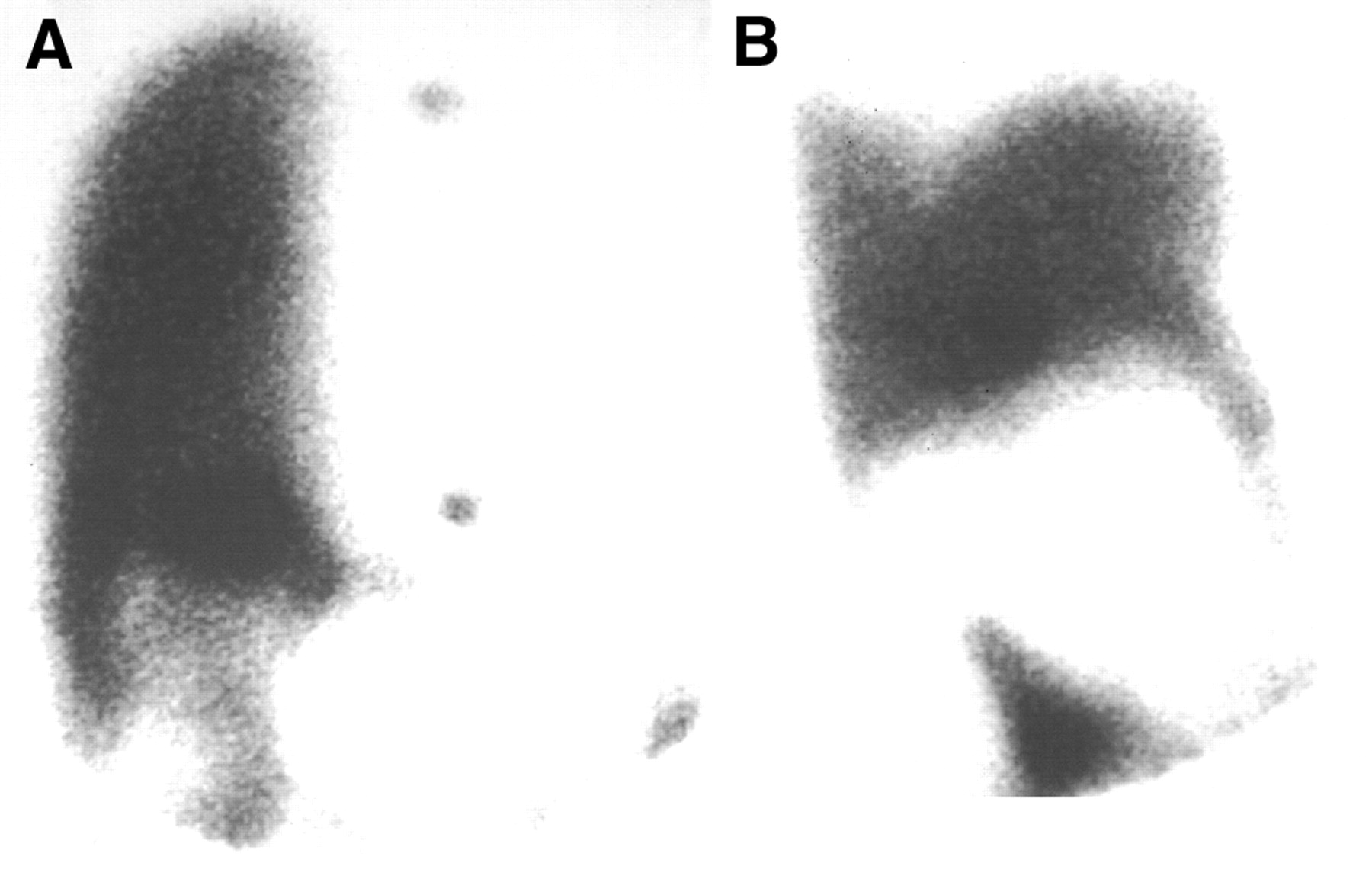
Two days later, 99mTc-MAA was reinjected using a similar technique. The images demonstrated diffuse peritoneal-cavity activity without a small-bowel pattern (Fig. 2). The supine view showed diffuse activity in the right hemithorax that could represent a patent peritoneal shunt with unilateral pulmonary artery perfusion or a unilateral right pleural effusion (Fig. 3A). The upright view clearly demonstrated a right unilateral pleural effusion, not a patent shunt with unilateral right pulmonary artery perfusion (Fig. 3B) (3).

Second 99mTc-MAA injection into peritoneal cavity shows diffuse activity throughout abdominal cavity without small-bowel activity.

Imaging over chest with patient supine and upright demonstrates importance of proper patient positioning. (A) Supine view shows diffuse activity in right hemithorax that could represent patent peritoneal shunt with unilateral pulmonary artery perfusion or unilateral right pleural effusion. (B) Upright view clearly demonstrates right unilateral pleural effusion, not patent shunt with unilateral right pulmonary artery perfusion.
DISCUSSION
The accidental small-bowel puncture that occurred during peritoneography in this patient was unusual. I could not find a single published report of this complication.
Subsequent reimaging of the patient demonstrated the importance of proper patient positioning, as only the images with the patient upright could distinguish between the 2 possible findings. I was not aware of this importance at the time but had performed such imaging out of interest and knowledge of physiology.
Some people prefer to use 99mTc-sulfur colloid (4) rather than 99mTc-MAA for peritoneography. Both techniques use a particulate radiopharmaceutical, and either is acceptable. The possibility of small-bowel puncture and the importance of patient positioning are relevant to both.
Acknowledgments
The author thanks Reference Librarian Barbara A. Bartkowiak, MTS, MLIS, for her help with Medline searches and in formulating key words and Library Assistant Jane A. Konop, AS, for locating articles. Both are from the George E. Magnin Medical Library of Marshfield Clinic. The author also thanks Marshfield Clinic Research Foundation for its support through the assistance of Alice Stargardt in the preparation of the manuscript. Diana M. Spieth, BS, prepared the illustrations.
Footnotes
For correspondence or reprints contact: Michael E. Spieth, MD, Nuclear Medicine Section, Department of Radiology, Marshfield Clinic, 1000 N. Oak Ave., H-1-NM, Marshfield, WI 54449.
E-mail: spieth.michael{at}marshfieldclinic.org





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.