


Abstract
We report on a high-dose radioiodine therapy after injection of recombinant human thyrotropin (rhTSH) in a 61-y-old woman with compression of the spinal cord caused by metastasis of a follicular thyroid carcinoma. Fourteen years ago, the patient underwent subtotal thyroidectomy because of multinodular goiter without any histologic evidence for malignant disease, and the patient was put on thyroxine substitution (100 μg/d). In April 2000, she developed paralysis of the right leg. Morphologic imaging revealed spinal compression caused by a space-occupying lesion within the thoracic spine. Subsequent biopsy and histology demonstrated metastasis of a follicular thyroid carcinoma. Therefore, high-dose radioiodine therapy was scheduled after 4 wk of hormone withdrawal. Within a few days of being off thyroxine, the patient’s paralytic symptoms worsened rapidly. The patient was again put on thyroxine, 100 μg/d, and high-dose radioiodine therapy under stimulation with rhTSH was performed without any side effects. The second high-dose radioiodine therapy 3 mo later, again performed under stimulation with rhTSH, showed significantly less iodine avidity, and thyroglobulin levels fell from 1,024 μg/L to 361 μg/L, thereby demonstrating therapeutic efficacy. Thus, rhTSH might be used as a tool not only in the diagnostic application but also in the therapeutic application of 131I.
The gold standard of follow-up of patients with differentiated thyroid carcinoma includes radioiodine scanning as well as thyroglobulin measurements under thyrotropin (TSH) stimulation. To achieve adequate TSH stimulation of ≥30 mU/L, patients have to be taken off thyroxine for at least 4 wk. However, this is often associated with severe side effects, such as fatigue, psychic disorders, and possible tumor progression.
Since March 2000, recombinant human TSH (rhTSH) (Thyrogen; Genzyme GmbH, Alzenau, Germany) is available and is licensed for diagnostic radioiodine scanning in European countries. The advantage of rhTSH is that it enables the physician to ensure adequate TSH stimulation without the necessity of coming off hormone medication. Consequently, patients who are treated with rhTSH have less symptoms of hypothyroidism (1,2) compared with the standard regimen. Moreover, when using rhTSH during radioiodine scanning, the same number of metastases has been detected on whole-body scans compared with the standard regimen (3). However, disadvantages of rhTSH are that neither the occurrence of edema at the site of spinal metastases nor a tendency of growth of metastases can be excluded (4).
We report on the application of rhTSH in a therapeutic setting using high-dose radioiodine in a 61-y-old woman with compression of the spinal cord caused by metastasis of a follicular thyroid carcinoma.
CASE REPORT
A 61-y-old woman suffering from follicular thyroid carcinoma with metastases in the thoracic spine was referred to the Department of Nuclear Medicine of the University Clinic Hamburg-Eppendorf, Germany, for high-dose radioiodine treatment.
In 1986, the patient underwent a subtotal thyroidectomy because of multinodular goiter without any histologic evidence for malignant disease, and she was put on thyroxine substitution (100 μg/d). In April 2000, she developed abdominal pain and a progressive paralysis of the right leg. Thorough physical examination did not reveal any other neurologic symptoms. MRI showed a space-occupying lesion in the third thoracic vertebra, leading both to a compression of the 2nd and 4th vertebra and to an edema of the spinal cord (Fig. 1). The paralytic symptoms improved after surgical decompression and stabilization. Subsequent biopsy and histology demonstrated metastasis of a follicular thyroid carcinoma (Fig. 2). According to the standard regimen, high-dose radioiodine therapy was scheduled after 4 wk of hormone withdrawal, and TSH rose to 6.38 mU/L in the following 3 wk. However, within this time period the patient’s paralytic symptoms worsened rapidly, and a CT scan demonstrated both the growth of the metastasis with infiltration per continuitatem into the adjacent parts of the 2nd and 4th thoracic vertebra and the occurrence of a new small osteolytic lesion in the corpus of the 5th thoracic vertebra. For this reason, the patient underwent a second surgical decompression, and the substitution with thyroxine, 100 μg/d, was reestablished.

Sagittal T1-weighted spinecho image of thoracic spine. Note space-occupying lesion in third thoracic vertebra compressing spinal cord. SP = spinal cord.
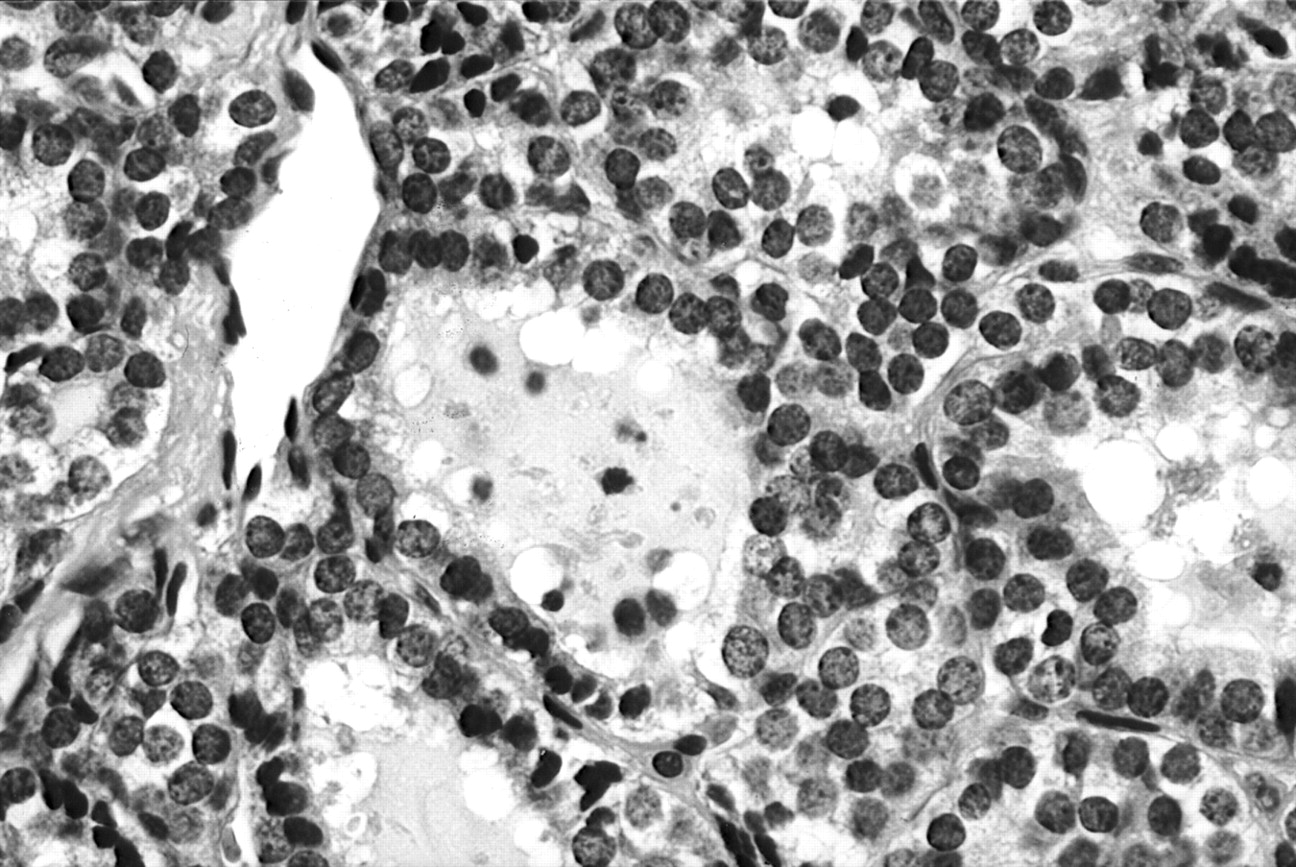
Conventional hematoxylin-eosin staining of space-occupying lesion of Figure 1 shows numerous cells from well-differentiated follicular carcinoma. Original magnification, 400×.
The patient was then referred to our department to evaluate the feasibility of high-dose radioiodine therapy after application of rhTSH within a compassionate-use program. At this time she was in a stable condition under thyroxine substitution, and sonography of the thyroid bed showed thyroid remnants of about 3 mL in volume. After written informed consent was obtained from the patient, rhTSH was injected intramuscularly on 2 consecutive days at a dose of 0.9 mg each. During stimulation with rhTSH, no severe side effects were observed in the patient. When asked for her subjective impression, she gave a description of warmer feet and less pain in the spine.
A standardized radioiodine uptake test was performed by oral application of 10.9 MBq 131I, starting after the first injection of rhTSH, and revealed 4% uptake of 131I in the thyroid bed 24 h later. A whole-body scan acquired contemporarily did not show any pathologic iodine-avid tissue in the remaining body.
Because of the risk of developing an iatrogenic thyrotoxicosis, thyroxine medication was withdrawn for 3 d, starting with the application of rhTSH. Levels of free T4 and the tumor marker human thyroglobulin were measured daily, and maximum levels were reached after 7 d, peaking at 37.8 pmol/L and 1,024 μg/L, respectively. The level of exogenous TSH reached its maximum after 2 d, peaking at 302 mU/L.
To prevent swelling of the metastasis, high-dose radioiodine therapy was performed under prednisolone (Decortin H; Merck, Darmstadt, Germany), 150 mg/d for 10 d, and the prednisolone dose was then halved for 4 d. Moreover, lithium carbonate (Quilonum retard; SmithKline Beecham, Munich, Germany) was given at a dose of 900 mg/d for a total of 10 d to increase the intrathyroidal half-life of 131I. The highest plasma concentration of lithium was measured as 0.81 mmol/L, and no side effects were observed.
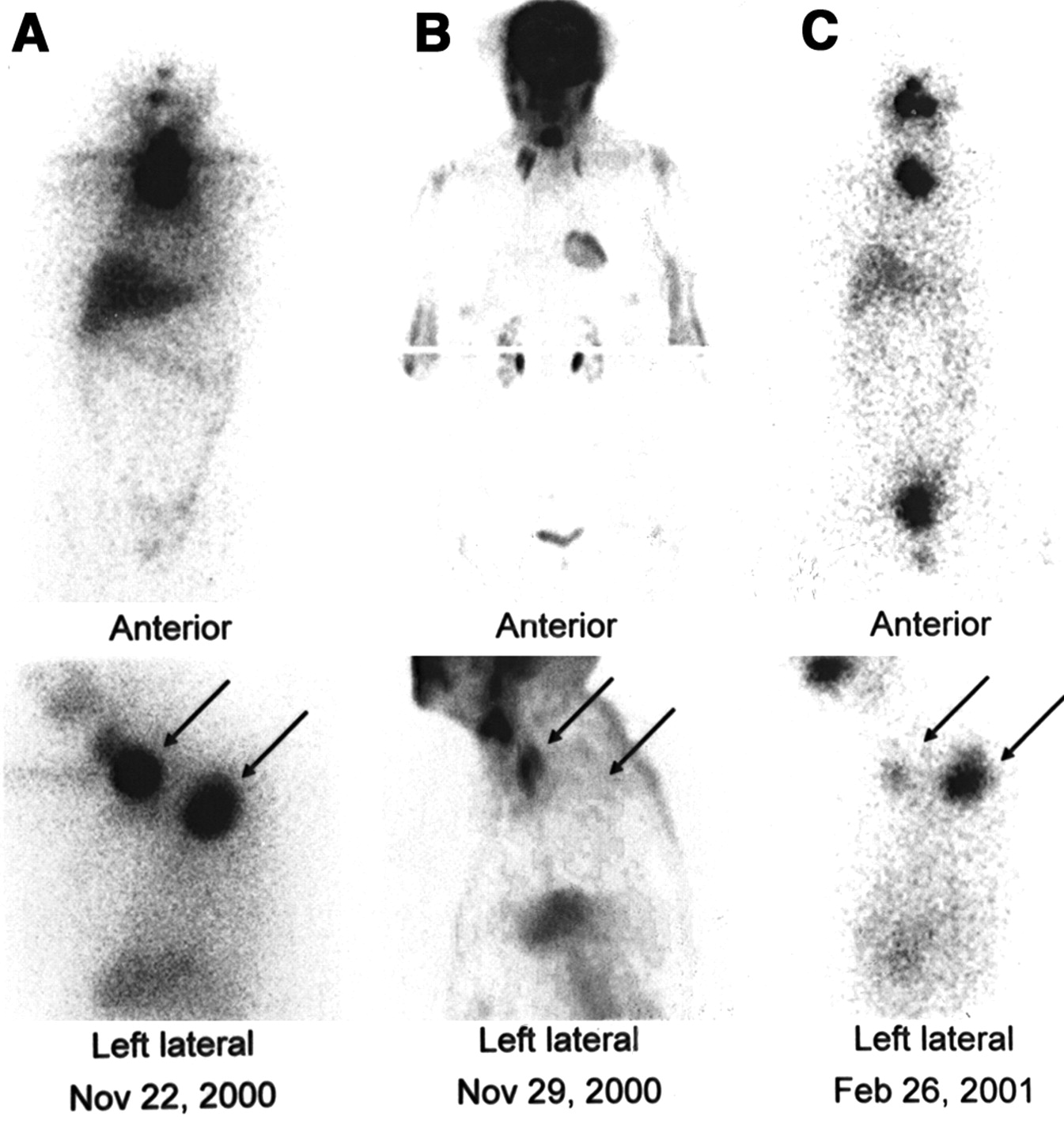
One day after the last injection of rhTSH, 7,480 MBq 131I were applied for high-dose radioiodine therapy, and whole-body images were acquired 7 d later to document the therapeutic activity of 131I after the therapy. Whole-body scanning demonstrated iodine-avid tissue in the thyroid bed and in the upper thoracic spine (Fig. 3A). Whole-body PET using 370 MBq 18F-FDG was performed 7 d later, and an increased glucose metabolism was not detected either within the thyroid bed or in the thoracic spine; in contrast, physiologic glucose utilization was observed in the entire body (Fig. 3B).
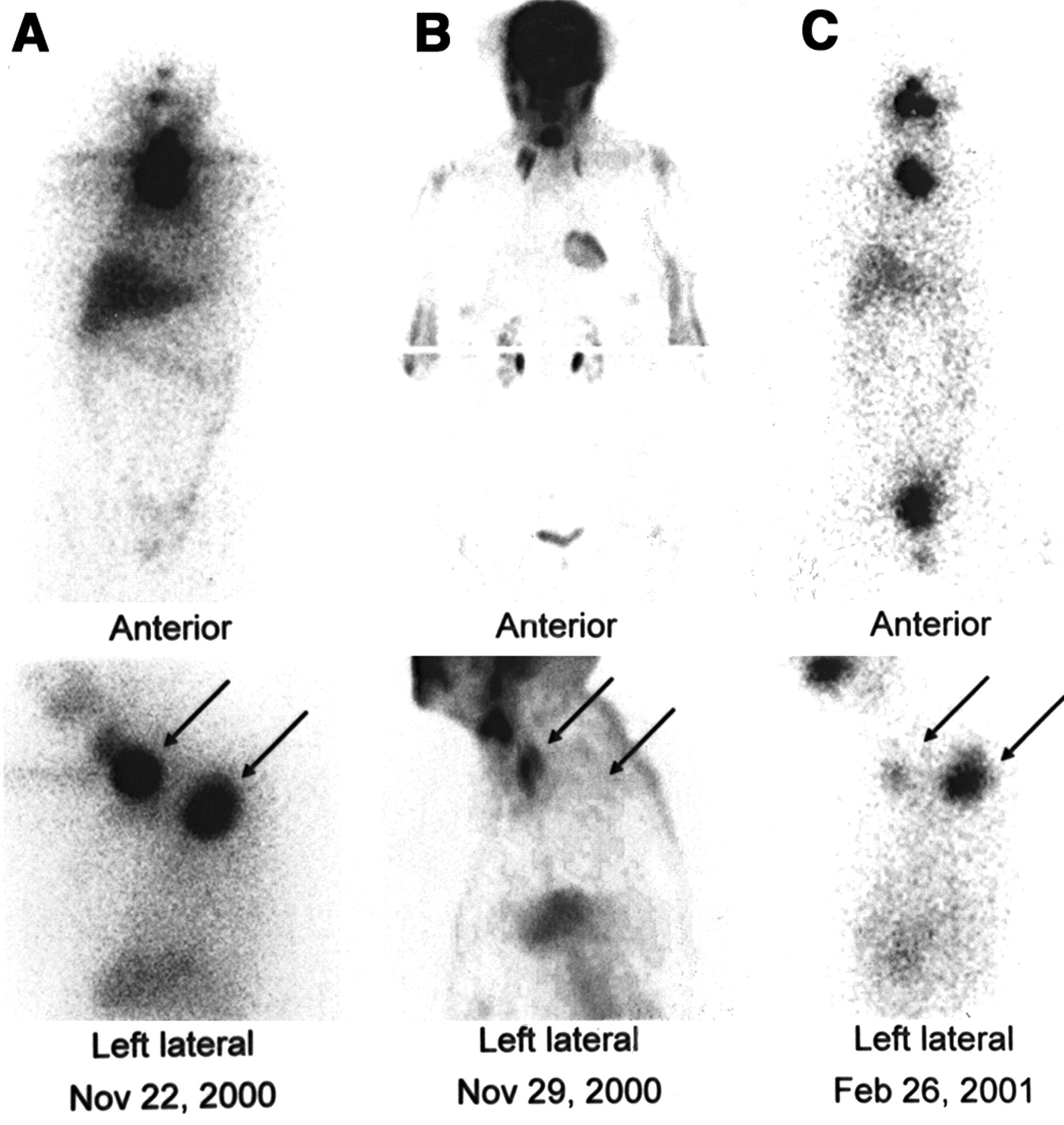
Whole-body scans from anterior views (top row) and spot images from left lateral views (bottom row). Images obtained after first radioiodine therapy (A) show 2 foci of intense iodine uptake (arrows) in thyroid bed and in thoracic spine, whereas images obtained 3 mo later after second radioiodine therapy (C) show significantly decreased iodine avidity in both lesions (arrows), thereby demonstrating therapeutic efficacy. (B) PET images obtained after first radioiodine therapy show no increased glucose metabolism in thyroid bed or in thoracic spine (arrows) but in lateral cervical muscles.
Three months later, high-dose radioiodine therapy was repeated under identical conditions, and whole-body scanning demonstrated significantly less iodine-avid tissue both in the thyroid bed and in the thoracic metastasis (Fig. 3C). Accordingly, maximum levels of human thyroglobulin measured under stimulation with rhTSH were 361 μg/L, thereby demonstrating the efficacy of the first high-dose radioiodine therapy.
DISCUSSION
Several authors have described the safety and efficacy of whole-body scanning using 131I under stimulation with rhTSH (1,2,5–10). In contrast, few data have been published regarding the application of rhTSH for therapeutic purposes in radioiodine therapy, and serious side effects such as symptoms of hyperthyroidism were reported in several of these studies (1,2,10–12).
We used rhTSH in a slightly different clinical setting of high-dose radioiodine therapy. After subtotal thyroidectomy 14 y ago, our patient suffered from differentiated thyroid cancer metastasized to the thoracic spine, and she developed paralysis of the right leg during the standard preparation for radioiodine therapy—that is, withdrawal of thyroxine for at least 4 wk. Therefore, we chose to perform high-dose radioiodine therapy after stimulation with rhTSH under concurrent medication with thyroxine. We found that rhTSH is both safe and efficacious in this clinical setting. This finding is supported for several reasons. First, although uptake of 131I may be less intensive after rhTSH compared with the standard regimen (3,13), in our patient 131I was taken up in both lesions—that is, the thyroid remnant and the bone metastasis in the thoracic spine—with a high tumor-to-background ratio during the first radioiodine therapy. Second, iodine avidity was significantly less during the second treatment session 3 mo later, thereby demonstrating the efficacy of the first high-dose radioiodine therapy. Third, 18F-FDG PET performed during the first treatment session because of excessively increased human thyroglobulin levels showed physiologic 18F-FDG distribution both in the thyroid bed and in the thoracic spine. These PET findings were in good agreement with the well-differentiated follicular structure described in the histopathologic report as published previously (14). Lastly, we did not observe any severe side effects. In our patient this finding might be caused predominantly by her rather small thyroid remnants, because in healthy individuals thyroid hormone levels are known to increase significantly after injection of doses of rhTSH as small as 0.1 mg (12). Other reasons may be the additional efforts we made to avoid any risk of hyperthyroidism:
Thyroxine substitution was withdrawn for a total of 3 d beginning with the day of injection of rhTSH. In fact, levels of free thyroxine reached maximum levels of 37.8 pmol/L 7 d after the application of rhTSH. However, the patient did not experience any symptoms of hyperthyroidism.
Prednisolone was given initially at a dose of 150 mg/d for 10 d and the dose was then halved for 4 d. The main effects of prednisolone are its antiinflammatory effect, which helped to prevent radiogenic thyroiditis, and its insulating effect on cell membranes, thereby preventing thyroxine from being released from the thyrocytes into the plasma.
Lithium carbonate was given at a dose of 900 mg/d for a total of 10 d. Lithium carbonate increases the intrathyroidal half-life of 131I by an insulation effect on the cell membrane of the thyrocytes, thereby reducing the risk of hyperthyroidism (15–17), and enhances the efficacy of radioiodine retention within metastases (18). In fact, whole-body scans performed after high-dose radioiodine therapy showed an excellent tracer accumulation in both iodine-avid lesions.
CONCLUSION
rhTSH was found to be safe and efficacious in this clinical setting.
Acknowledgments
The authors are indebted to Lutz Hering, MD (Department of Radiology, Hospital Barmbek, Hamburg, Gemany), for providing the MRI and to Jörg Blaudszun, MD (Department of Pathology, Hospital Barmbek, Hamburg, Gemany), for histopathologic analysis. The authors also thank Genzyme GmbH for providing rhTSH.
Footnotes
For correspondence or reprints contact: Karl H. Bohuslavizki, MD, PhD, Nuklearmedizin im Spitalerhof, Spitaler Strasse 8, 4th Obergeschoss, 20095 Hamburg, Germany.
E-mail: bohu{at}nuklearmedizin-spitalerhof.de





{kind=link}
{kind=link}
{kind=link}