

Abstract
After significant trauma to the spleen, small viable splenic fragments may exist in the peritoneal cavity or, less commonly, in the thorax. Thus, the appearance of splenules within the thorax on CT images can easily be mistaken for malignancy and lead to unnecessary intervention. Here, we present a case of multiple pulmonary masses that initially were presumed to be malignancy, leading to CT-guided biopsy, but were eventually confirmed to be thoracic splenules through 99mTc-labeled sulfur colloid scintigraphy.
- correlative imaging
- 99mTc sulfur colloid
- splenosis
- splenic trauma
For evaluation of liver and spleen disease, 99mTc-labeled sulfur colloid scintigraphy is a reliable noninvasive technique. Visualization of radiotracer uptake on 99mTc-sulfur colloid scintigraphy usually indicates normally functioning hepatic and splenic tissue. Here, we present a case of thoracic splenosis detected on 99mTc-labeled sulfur colloid scintigraphy in a patient with a remote history of splenectomy for a gunshot wound.
CASE REPORT
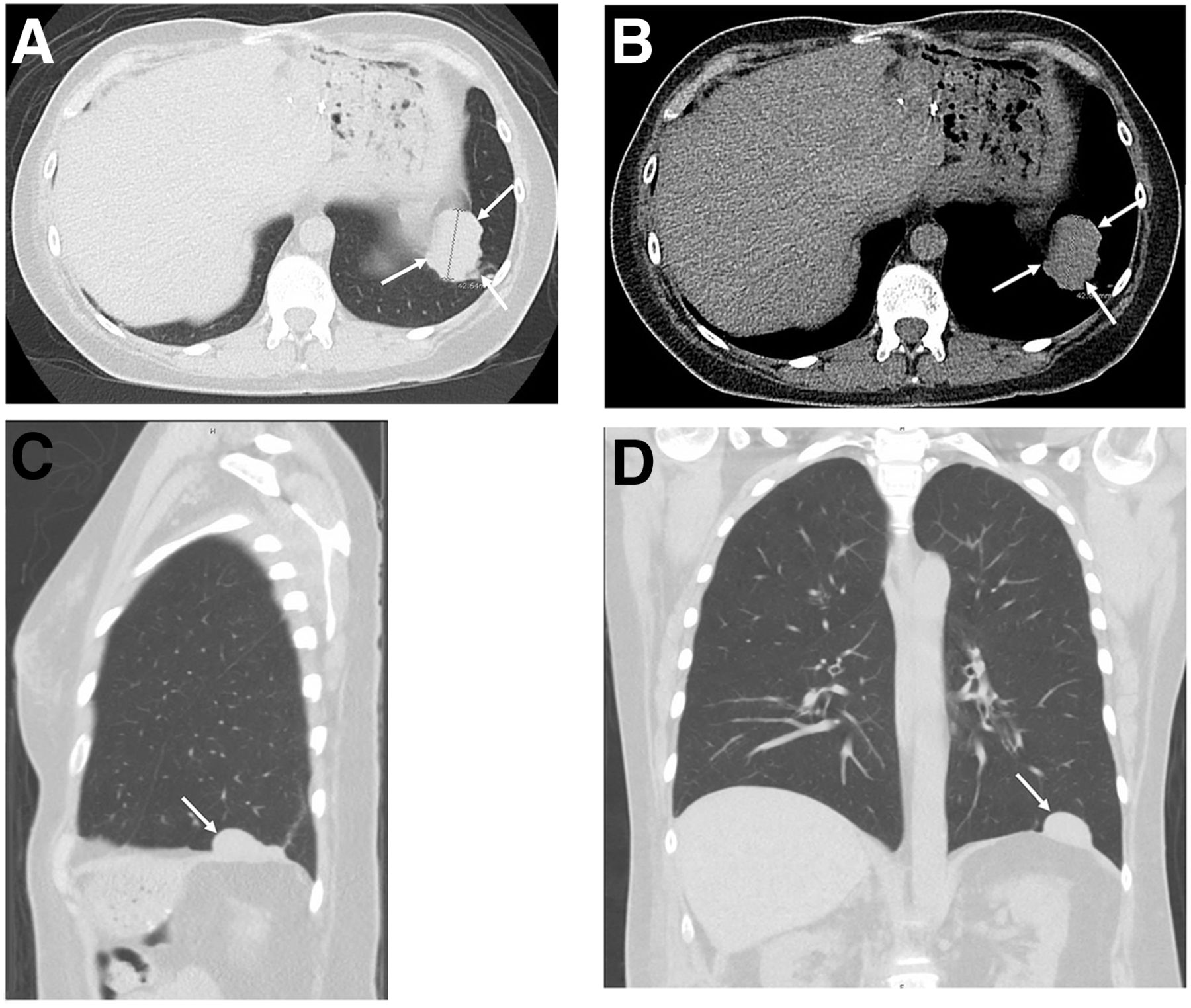
A 46-y-old woman with a remote history of gunshot wound to the abdomen was admitted to the emergency room complaining of abdominal pain. She also indicated a history of chronic nonbloody productive coughing, which she attributed to her 45-year history of smoking. CT of the abdomen and pelvis demonstrated a tissue density measuring 4.2 cm above the left diaphragm. Because no prior images were available, malignancy was suspected. Thus, a needle biopsy guided by dedicated chest CT was performed because of the patient’s smoking history.
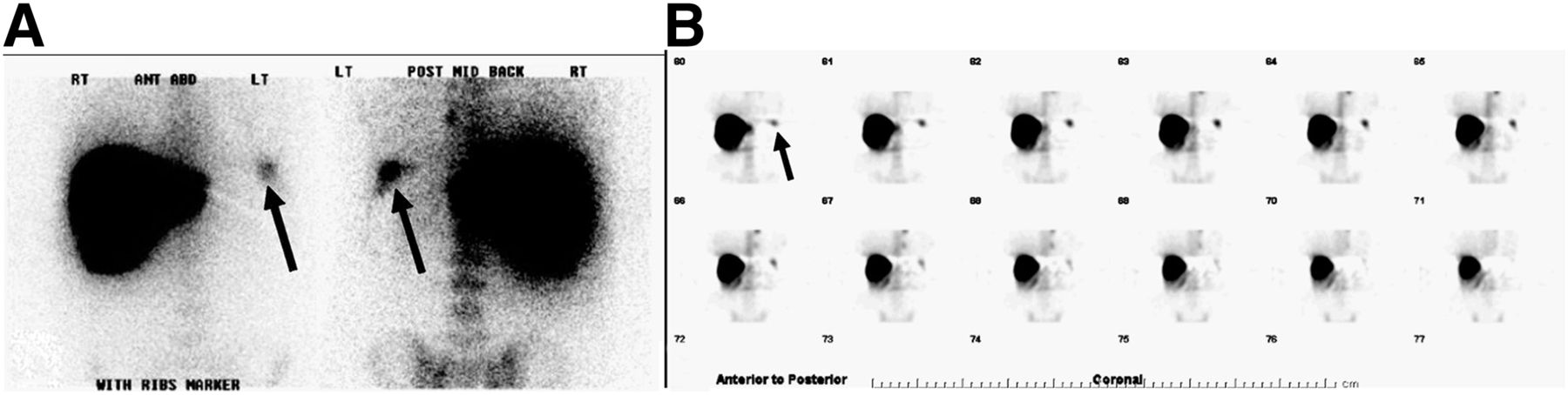
The images (Fig. 1) revealed at least 7 nonspecific soft-tissue densities in the left hemithorax, with no other signs of trauma. Because there was no spleen in the left upper abdomen, a 99mTc-labeled sulfur colloid scan was suggested to confirm accessory splenic tissue. The patient was subsequently injected with 303.4 MBq (8.2 mCi) of 99mTc-labeled sulfur colloid, and planar and SPECT images were acquired. The images revealed elevated radiotracer uptake by implanted tissue thought to be of splenic origin (Fig. 2). Histopathology from the CT-guided biopsy confirmed these findings of thoracic splenosis.

Unenhanced CT chest images reformatted in axial (A and B), sagittal (C), and coronal (D) projections showing intrathoracic soft-tissue mass abutting left hemidiaphragm (arrows).

{kind=link}
{kind=link}
99mTc-labeled sulfur colloid planar images in anterior and posterior projections (A) and SPECT images in coronal projection (B) showing radiotracer uptake by thoracic masses (arrows). These findings confirmed tissue to be of splenic origin.
DISCUSSION
Because of the patient’s remote history of gunshot wound to the abdomen and evidence of posttraumatic splenectomy more than 20 years previously, the soft-tissue masses were easily confirmed as being of splenic origin. Tobacco use increases the incidence of malignancy in the lungs, gastrointestinal tract, liver, kidneys, and bladder (1), among other locations. Unexplained ectopic tissue in these organs must therefore be further worked up. Similarly, splenic implants may be mistaken for lung cancer (2), renal cancer, and peritoneal seeding in patients with a history of bladder carcinoma, primary or metastatic hepatic malignancy (3), or nonmalignant causes such as endometriosis (4). Given the patient’s long history of smoking, the likelihood of malignancy could not be comfortably excluded and further work-up was necessary.
In a patient with a history of trauma requiring splenectomy, we may expect to find splenic implants in the abdomen and pelvis, with intrathoracic implants being a remote possibility. According to the 2015 ACR-SPR guidelines for spleen scintigraphy, if there is suspicion that trauma may have ruptured the diaphragm, the chest should be imaged as well. (5). Additionally, in an effort to preserve some immune functionality, surgeons may attempt autotransplantation of splenic tissue, which will then be evident on imaging with 99mTc-labeled heat-damaged red blood cells or 99mTc-labeled sulfur colloid (6). Figure 2 demonstrates increased radiotracer uptake by the pulmonary masses in the thorax after injection of 99mTc-labeled sulfur colloid, demonstrating benign ectopic intrathoracic splenosis.
CONCLUSION
This case demonstrates that scintigraphy using the readily available tracer 99mTc-labeled sulfur colloid can be an easy confirmatory test in a patient with suspected thoracic splenosis, thus eliminating the need for invasive tissue biopsy.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 4, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- Received for publication May 24, 2016.
- Accepted for publication July 5, 2016.