


Abstract
The objective of this study was to determine whether posttherapy 131I SPECT/CT changed the need for additional cross-sectional imaging or modified the American Thyroid Association risk of recurrence classification. We performed planar imaging and SPECT/CT in a consecutive series of patients after 131I therapy. Methods: Planar imaging and SPECT/CT were performed on 148 consecutive patients with thyroid carcinoma (125 papillary, 2 follicular, 8 Hürthle cell, and 13 poorly differentiated) approximately 5 d after the therapeutic administration of 1,739–8,066 MBq (47–218 mCi) of 131I. The indication for treatment was postsurgical ablation (n = 109) or recurrent or metastatic disease with rising thyroglobulin levels (n = 39). SPECT/CT scans were obtained for all subjects for 1 bed position (38 cm), which included the neck and upper chest. Additional SPECT/CT scans of the abdomen or pelvis were acquired if suggestive findings were noted on planar images. All patients were treated in real time, according to the standard of care in our practice. At that time, clinical decisions regarding thyroid tumor classification were made by our multidisciplinary group based on all data, including operative findings, pathology, imaging, and thyroglobulin levels. In a retrospective analysis, planar and SPECT/CT images were interpreted independently, and sites of uptake were categorized as likely benign, malignant, or equivocal. An experienced thyroid endocrinologist used a combination of surgical histopathology and scan findings to determine whether additional cross-sectional imaging was required and determined if the imaging findings changed the patient's risk category. Results: In 29 patients, 61 additional cross-sectional imaging studies were avoided using SPECT/CT, compared with medical decision making based on the planar images alone. In 7 of 109 postsurgical patients, SPECT/CT findings changed the initial American Thyroid Association risk of recurrence classification. The sensitivity of planar imaging and SPECT/CT for identification of focal 131I uptake in the thyroid bed was similar in the postsurgical and recurrence cohorts. For metastatic disease in the neck, characterization of 131I uptake by SPECT/CT in the postsurgical group was significantly better than that by planar scanning (P < 0.01). Among the 109 postsurgical patients, the characterization of iodine uptake in the lung, liver, and bone was also more accurate using SPECT/CT than planar scanning (P < 0.01). The CT portion of SPECT/CT demonstrated non–iodine-avid lesions in 32 of 148 patients. Conclusion: SPECT/CT data provided information that reduced the need for additional cross-sectional imaging in 29 patients (20%) and significantly altered the initial risk of recurrence estimates in 7 of 109 patients (6.4%), thereby altering patient management recommendations with regard to frequency and intensity of follow-up studies.
Therapy with 131I is effective for thyroid cancer patients who are at an intermediate to high risk for recurrence or intermediate to high risk of dying from their disease (1). Four to 7 d after 131I administration, images of the neck, chest, and whole body are recorded to detect sites of iodine uptake. Depending on the location of these sites, iodine uptake may change the planned patient management and frequency of surveillance; some patients may also require additional cross-sectional imaging or biopsy for evaluation.
SPECT/CT instruments allow contemporaneous SPECT and CT scanning for anatomic localization, which increases the certainty of information available from these posttherapy images (2). The clinical significance of these findings is a matter of ongoing discussions. Not all patients with thyroid cancer require treatment with 131I, and patient management during follow-up after total thyroidectomy will vary depending on the initial risk classification. This risk classification has been updated in the recent guidelines by the American Thyroid Association (ATA) (3). The new system divides thyroid cancer patients into 3 risk groups—low, intermediate, and high risk. Management and follow-up are tailored to the risk of recurrence in the initial assessment after total thyroidectomy. Patients are considered at low risk if they had complete resection of all tumor, no aggressive tumor histology, no invasion of locoregional tissues, no vascular invasion, and no metastases. Patients with microscopic invasion into perithyroidal tissue, cervical lymph node metatases, aggressive histologies, or vascular invasion are classified as being at intermediate risk, and patients with macroscopic gross extrathyroidal extension, incomplete tumor resection, or distant metastases are classified as being at high risk of recurrence.
In this study, we compared posttherapy 131I imaging findings on planar and SPECT/CT scans, assessed the clinical utility of SPECT/CT in clarifying equivocal findings and in detecting additional abnormalities not visualized on planar images, and determined whether and how SPECT/CT would alter the initial risk classification and follow-up care (including the need for additional cross-sectional imaging studies in the immediate period after the posttherapy scan). We addressed these questions separately for patients undergoing initial treatment after total thyroidectomy and patients with suspected or established metastatic disease, because clinical algorithms vary and the initial ATA risk classification pertains only to postsurgical patients. In our institution, most low-risk patients are not treated with 131I after total thyroidectomy. Therefore, this report describes our experience in primarily intermediate- and high-risk patients.
MATERIALS AND METHODS
This study included 148 consecutive patients treated with 131I at our institution between April 2006 and December 2007. The data collection and analysis were approved by our Institutional Review Board. These patients were referred either for initial postsurgical 131I ablation or for 131I therapy of recurrent or metastatic disease. Posttherapy imaging was performed at 4−7 d after 131I therapy. 131I planar images of the body were obtained in the anterior and posterior projections using dual-head γ-cameras (Vertex Plus dual 1.6-cm [5/8″] detector camera; Philips) equipped with high-energy general-purpose collimators, at 12 cm/min. Anterior and posterior planar images of the whole body were routinely obtained, supplemented by anterior, posterior, and lateral spot images of the neck and thorax (1 field of view) plus any other region deemed clinically appropriate.
SPECT/CT images of the neck and chest were obtained in all subjects. In most patients, this SPECT/CT scan covered the area from the skull base to the diaphragm. In 6 patients, additional SPECT/CT images were acquired because the planar images demonstrated nonphysiologic focal iodine uptake in the abdomen or pelvis. SPECT/CT was recorded using a Philips Precedence system, which consists of a dual-detector γ-camera with dual 1.6-cm (5/8″) detectors equipped with high-energy general-purpose collimators and an integrated 16-slice helical CT scanner. CT scans were acquired with a tube voltage of 120 kV; the tube current was adjusted for body weight (e.g., 37.5 mAs for 70 kg of body weight). Reconstructed slice width and spacing was 3 mm. CT data were used for attenuation correction and anatomic information. SPECT data were obtained on a dual-head camera in step-and-shoot mode, using a noncircular orbit, a 128 × 128 × 16 matrix, and 32 angles over a total of 180° (per detector); the acquisition time varied between 30 and 60 s per stop, depending on the counting rate. Reconstruction was performed on a Philips JETStream system using the Philips Astonish algorithm.
All patients were treated in real time, according to the standard of care in our practice. At that time, clinical decisions based on all data regarding thyroid tumor classification were made by our multidisciplinary group, including operative findings, pathology, imaging, and thyroglobulin levels. The subject of this paper is a systematic retrospective comparison of planar and SPECT/CT findings. For this purpose, 2 nuclear medicine physicians jointly reviewed planar and SPECT/CT data and recorded findings as benign, malignant, or equivocal. Findings were characterized as benign when iodine uptake localized to physiologic sites, including the salivary glands or the gastrointestinal or urinary tract. Findings were characterized as malignant when localized to lymph nodes, bones, or soft-tissue organs (other than bowel and urinary tract). In each case, focal iodine uptake was compared with CT scan findings and if it corresponded to characteristic CT findings, such as small lung nodules or lytic bone lesions, it was considered positive. Abnormalities on the CT scan were recorded, including lymph node size, lytic or sclerotic bone lesions, and the like.
Abnormalities identified on SPECT and CT were evaluated to determine the incidence of discordant findings. The results were analyzed for the entire cohort of thyroid cancer patients and then separately for the 2 groups of patients with either postsurgical 131I ablation or suspected or proven recurrent or metastatic disease. For each patient, focal 131I uptake on planar or SPECT/CT images was analyzed for the thyroid bed, lymph nodes in the neck, and distant sites in the chest, liver, and bones.
An experienced thyroid endocrinologist reviewed the histopathology and information provided in the planar and SPECT/CT datasets. Findings on planar images were reviewed first, without knowledge of SPECT/CT findings. Then the endocrinologist decided the appropriate patient management (in particular, the need of further tests and dedicated cross-sectional imaging studies, such as contrast CT or MRI of the chest or abdomen or pelvis) to characterize and localize focal 131I uptake, particularly when the uptake was characterized as equivocal or the scan findings were inconsistent with other clinical data. Several weeks later, in a masked fashion, the same endocrinologist reviewed the SPECT/CT findings and the same questions were addressed. In addition, the ATA risk of recurrence was assessed in all postsurgical patients, considering clinical, pathologic, and planar scan findings. The risk of recurrence was then reassessed, taking into account any additional findings from the SPECT/CT scan. For example, if 131I uptake in the lungs or abdomen on the planar scan was shown to be nonspecific or not related to thyroid cancer on the SPECT/CT scan, the classification of many patients would change from high to intermediate risk. Similarly, new distant metastases on the SPECT/CT scan would elevate patient risk from intermediate to high, and new uptake in neck lymph nodes would change a patient from low risk (thyroid bed) to intermediate risk (nodal uptake).
We addressed how often SPECT/CT findings changed the initial risk stratification, because these changes would affect the intensity and frequency of follow-up in thyroid cancer patients.
Statistical Analysis
A generalized McNemar or Stuart–Maxwell test (4) was used to determine whether the assignment of benign, equivocal, and malignant findings by planar whole-body imaging and SPECT/CT had the same distribution. Analyses were performed separately for posttherapy 131I scans of postthyroidectomy patients and those with suspected or established metastatic disease. All tests were performed in SAS (version 9.1; SAS Institute) and R (version 2.7; SAS Institute) statistical software. All P values reported were 2-sided, and a P value of less than 0.05 was considered significant.
RESULTS
One hundred forty-eight consecutive thyroid cancer patients referred to our service for postsurgical 131I ablation or therapy of suspected or proven metastatic disease were included in this study; the clinical and treatment details are shown in Table 1. One hundred nine of the 148 patients underwent postsurgical 131I ablation of residual thyroid tissue. In the remaining 39 patients, a posttherapy 131I scan was obtained after treatment for suspected or proven metastatic disease based on elevated thyroglobulin levels. The specific 131I activity for thyroid remnant ablation and treatment of suspected or proven recurrence and metastatic disease was determined by a multidisciplinary tumor board on the basis of a patient risk profile including intraoperative findings, tumor size, histopathologic features, baseline and stimulated thyroglobulin levels, clinical parameters, and other imaging studies when available.
Patient Demographics
Localization and Characterization of 131I Iodine Uptake
On planar images, 95 of the 148 patients showed benign findings, 23 patients equivocal, and 30 patients malignant. SPECT/CT confirmed the benign nature of focal 131I uptake in 82 of the 95 patients characterized as such on planar scans; however, in 12 patients, findings were considered malignant and in 1 patient equivocal. Of the 23 patients with equivocal findings on the planar scan, 14 of these patients were characterized as benign, 3 were characterized as malignant, and 6 remained equivocal as determined by the SPECT/CT scan. Finally, among the 30 patients with malignant findings on the planar scan, SPECT/CT confirmed those malignant findings in 27, found benign iodine uptake in 2, and classified findings as equivocal in 1 patient.
We then assessed 131I uptake on the planar and SPECT/CT scans in the 2 separate patient cohorts (postsurgical vs. suspected recurrence) under 3 broad categories: in the thyroid bed, in neck lymph nodes, or at distant sites including lungs, liver, and bone.
Thyroid Bed
Planar and SPECT/CT scans showed close agreement in characterizing foci in the thyroid bed in both postsurgical and recurrence cohorts (data not shown). In the postsurgical group, disagreement was observed only in 2 of the 109 patients, in whom iodine uptake was localized to the thyroid bed on the planar scan but localized to lymph nodes on the SPECT/CT scan. Similarly, in 5 of 39 patients in the recurrence cohort, SPECT/CT localized iodine uptake to lymph nodes, which was thought to be in the thyroid bed on the planar scan.
Lymph Node Disease
Differences between the planar and SPECT/CT scans were significant in characterizing iodine uptake in the neck. In the postsurgical cohort (Fig. 1A), 95 patients showed no 131I uptake in the neck on planar images and thus no evidence for lymph node metastases. On the SPECT/CT scan, no 131I uptake in the neck was confirmed for 83 of the 95 patients (87%). However, 11 patients (12%) showed metastatic focal iodine uptake in neck nodes, and in 1 case mild iodine uptake remained equivocal on the SPECT/CT scan.
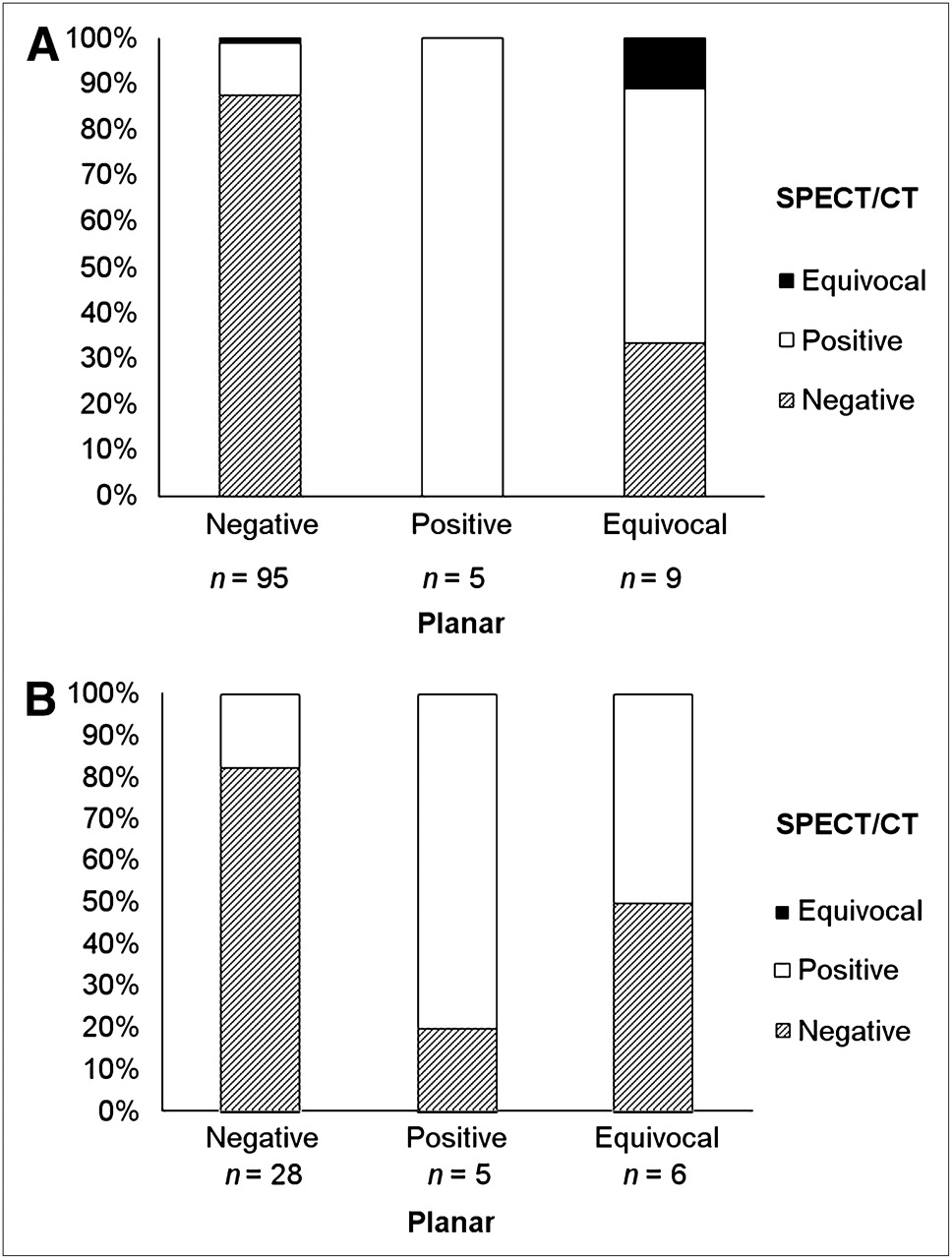
Difference between SPECT/CT and planar imaging in postsurgical (A) and recurrent or metastatic cohorts (B) in terms of characterization of neck lymph node metastases.
Nine patients had equivocal findings in the lateral neck on planar scans, in which possible nodal uptake was not clearly distinguishable from uptake in the thyroid bed. SPECT/CT findings were negative in 3 patients, showed focal uptake in neck nodes (suggestive of metastases) in another 5 patients, and remained equivocal in 1 patient (Fig. 1A). Therefore, in total the lymph node status was changed from N0 to N1+ in 16 of the 109 postsurgical patients (15%).
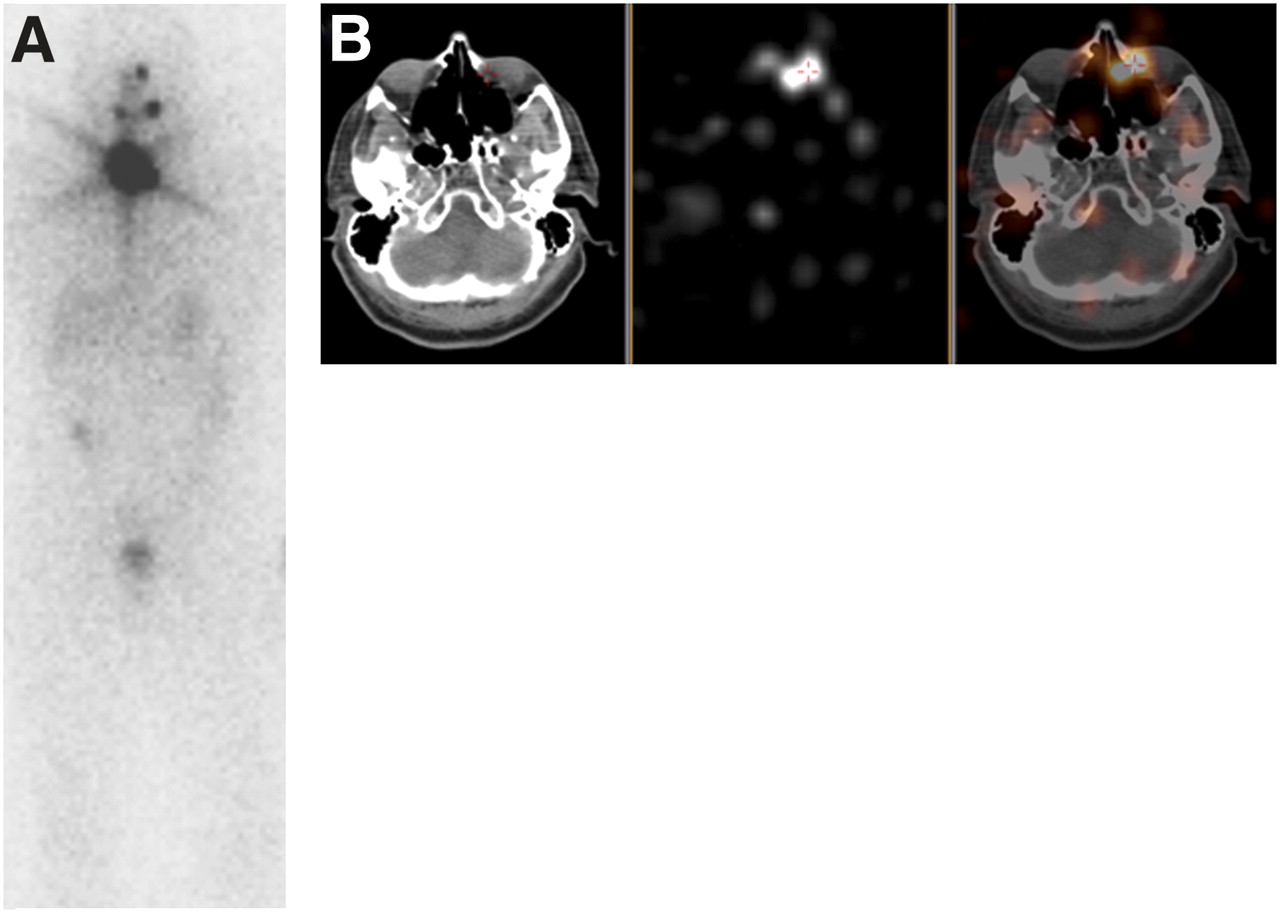
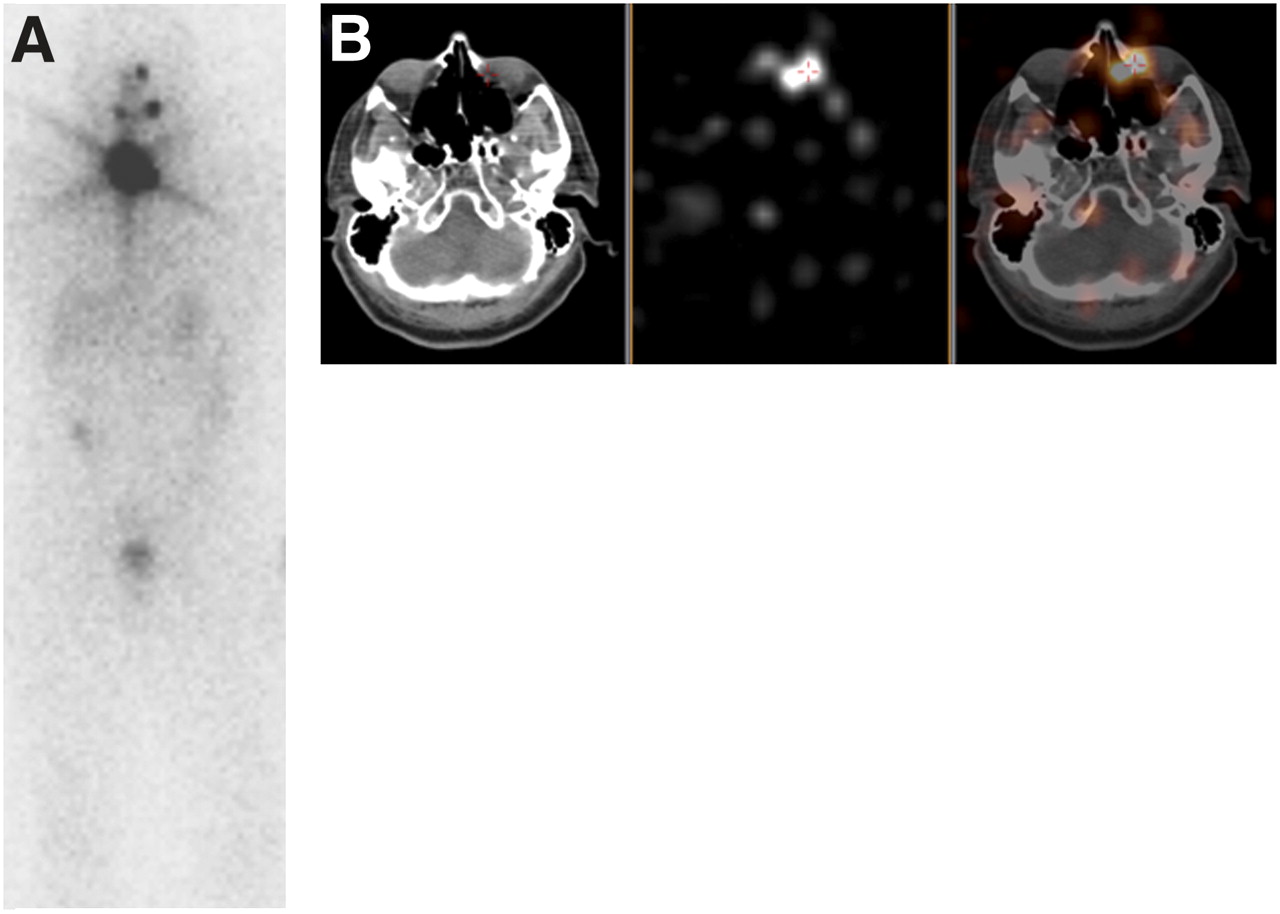
In the 39 patients with suspected recurrence (Fig. 1B), 28 patients showed no evidence of neck nodal disease on planar images. In 5 of these patients (18%), the SPECT/CT scan showed iodine uptake in neck lymph nodes and confirmed the absence of neck disease in the other 23. Six patients showed equivocal findings on the planar scan. SPECT/CT was able to resolve the equivocal status and classified 3 patients as negative and 3 other patients as having focal iodine uptake in neck nodes (Fig. 2). In summary, the lymph node status was changed from N0 to N1+ in 8 of the 39 patients in the suspected-recurrence group (21%).

Planar posttherapy 131I scan (A) in 16-y-old boy, postthyroidectomy, demonstrating multiple foci of uptake in neck. Three-dimensional maximum-intensity-projection axial CT, SPECT, and SPECT/CT images (B) show uptake in bilateral lower neck indicating supraclavicular lymphadenopathy. SPECT/CT image (C) also shows iodine-avid left posterior neck node.
Overall, we noted significantly more neck node metastases on SPECT/CT than on planar scanning (P < 0.01 and 0.02 for postsurgical and recurrence cohorts, respectively). Nodal size was measured on the CT portion of the SPECT/CT and was 3–5 mm in all but 2 patients (1 patient had a 2-cm retrotracheal or periesophageal node, the other a 5 × 3 cm retrosternal mass; both were better localized on the SPECT/CT scan). No difference in detection of central compartment versus lateral neck nodes on the SPECT/CT scan was observed.
Distant Metastatic Disease
The distribution of findings between the planar and SPECT/CT scans was significantly different in the postsurgical cohort (P < 0.01). The largest disagreement was observed in 11 patients with equivocal iodine uptake on the planar scan: in 9 patients (82%), SPECT/CT proved the benign nature of this uptake (e.g., physiologic iodine accumulation in bowel, urinary tract, and the like), whereas metastatic disease was proven in 1 patient, and findings in 1 patient remained equivocal (Fig. 3A).

Difference between SPECT/CT and planar imaging in postsurgical (A) and recurrent or metastatic cohorts (B) in terms of characterization of distant metastases in lungs, liver, and bone.
In the group with suspected recurrence (Fig. 3B), there were 6 patients with equivocal iodine uptake on the planar scan. In 2 of these 6 patients, for whom the planar scan suggested abnormal uptake in bone, the SPECT/CT finding was normal (Fig. 4). In another 3 patients, osseous metastatic disease was shown on the SPECT/CT scan, and findings in 1 patient remained equivocal. However, the overall characterization of focal iodine uptake outside the neck by planar scanning or SPECT/CT did not differ (P = 0.08), possibly related to our small sample size in this group.
A 44-y-old man with papillary thyroid cancer, postthyroidectomy, and 131I therapy with 5,550 MBq (150 mCi). Planar posttherapy scan (A) demonstrates uptake in left frontal skull. Axial CT, SPECT, and SPECT/CT images demonstrate this uptake to be benign secretion in left nasolacrimal duct.
Relevant CT Findings
The CT portion of the SPECT/CT provided additional information about non–iodine-avid lesions in 32 of the 148 patients. Nineteen of these 32 patients had tiny lung nodules, 10 had neck or mediastinal lymph nodes less than 5 mm, and 3 had osteolytic bone metastases (2 of these patients also had tiny lung nodules and 1 had pleural effusions and atelectasis [the latter showing mild iodine uptake]).
Management Implications
In light of the medical history, the endocrinologist would have requested 90 cross-sectional imaging studies (in 60 of the 148 patients) to clarify findings on the planar scan. In contrast, only 29 cross-sectional studies (in 29 patients) were requested on the basis of SPECT/CT reporting. These 29 cross-sectional studies included 24 high-resolution CT scans of the chest, 1 neck ultrasound, one 18F-FDG PET/CT scan, 1 MRI scan of the breast, and 2 MRI scans of the abdomen and pelvis. Therefore, SPECT/CT, compared with medical decision making based on the planar images alone, avoided 61 cross-sectional imaging studies in 29 patients—that is, additional imaging studies were avoided in 48% of the patients for whom they would have been considered necessary on the basis of planar scanning alone, or 20% of our entire patient population.
On the basis of patient age, pathology, and findings on the planar scan after therapy, the 109 postsurgical patients were risk-classified using the ATA criteria as follows: 22 were classified as low risk, 65 as intermediate risk, and 22 as high risk. In contrast, on the basis of the SPECT/CT findings, 23 patients were reclassified as low risk, 69 as intermediate risk, and 17 as high risk. In 7 of these 109 patients, the SPECT/CT findings changed the risk classification: 6 patients were assigned to a lower risk group (including reclassification from high to low risk in 1 patient, and from high to intermediate risk in 5 patients), and 1 patient was assigned to a higher risk group (Table 2).
Change in ATA Risk Classification After Planar Scanning Versus SPECT/CT
DISCUSSION
The utility of SPECT/CT is under study in patients with thyroid carcinoma (2,5–11). Studies have shown that SPECT/CT has an incremental diagnostic value over planar imaging and that it may change management in 25%–50% of patients (2,6,8). Our study confirms some of these data, but it differs in several important aspects. We consistently applied SPECT/CT in the posttherapy 131I setting in a consecutive series of patients and applied the new ATA risk criteria for thyroid cancer. We found that SPECT/CT helped to localize focal iodine uptake and characterize it as either normal or abnormal, thereby reducing the need for additional imaging studies. In postthyroidectomy patients, SPECT/CT findings affected the ATA risk classification, with implications for management by changing the interval for clinical follow-up and the need for additional imaging and laboratory tests.
We elected to evaluate the role of SPECT/CT in the posttherapy setting, because the administered activity is 10- to 30-fold greater than that used for diagnostic studies, and the longer interval between activity administration and imaging increases target-to-background contrast, resulting in the detection of more sites of radioiodine-avid disease, compared with the diagnostic study (12–14). Other authors also evaluated SPECT/CT in this setting, but in some studies SPECT/CT was obtained only in light of equivocal planar scans (2,6,11,15). In contrast, we obtained SPECT/CT scans of the neck and chest in 1 field of view routinely, thus avoiding any selection bias while addressing 2 of the most important metastatic disease sites—that is, the neck nodes and lungs. This is important because SPECT/CT demonstrated iodine uptake in neck lymph nodes in 5 of 35 (14%) patients with suspected recurrence in whom the planar scan localized the iodine uptake to the thyroid bed. These patients would not have been included if the decision to perform SPECT/CT had been triggered only by equivocal (with regard to nature of iodine uptake or location) planar findings. In contrast, we performed additional SPECT/CT of other body regions only to clarify equivocal findings on planar scans because the probability for distant disease would be estimated on the basis of initial risk classification and it would be unusual to have distant metastases in light of a negative planar scan result.
Our study found a 15% change in nodal status from N0 to N1+ or Nx to N1+ in the postsurgical group. This change is similar to that found by Schmidt et al. (8), who noted a change in nodal status with SPECT/CT in 8 of 57 patients (14%). Our study also showed a 20% change in patient management, based on the elimination of additional imaging studies. This number is again similar to the numbers reported in prior studies (6,8,9,11,15).
Some prior studies investigated the role of combined SPECT/CT in patients after thyroidectomy but before treatment with 131I (7,9). In 1 of these studies (9), SPECT/CT findings changed the therapeutic management in 21 of 108 patients by better selection of surgery or 131I therapy. Although the management of thyroid cancer varies widely among institutions, in our practice pretherapy 131I SPECT/CT would not alter patient management in a meaningful manner, because the decision to administer 131I after thyroidectomy and the patient-specific dose are based on overall risk of recurrence. Risk assessment includes patient age and intraoperative and histopathologic findings. It is unlikely that larger lymph node metastases would have been missed intraoperatively, especially given the widespread use of preoperative ultrasound. Even if SPECT/CT showed iodine uptake in nodes after thyroidectomy, the true extent of nodal disease would still be underestimated significantly because of the limited administered activity in diagnostic scans and high frequency of microscopic nodal metastases. However, microscopic metastases do not seem to affect prognosis adversely, and their presence, by itself, would not be a major factor in determining the appropriate activity for 131I treatment after thyroidectomy.
In thyroid cancer, risk stratification is used to predict the probability for death from this disease, for local recurrence, and for treatment failure (16). To our knowledge, the effect of posttherapy SPECT/CT on risk stratification per the new ATA guidelines has not been addressed.
One parameter determining the risk for recurrence is the presence of abnormal 131I uptake on the first postablation iodine scan. For example, the low-risk group is defined by an absence of 131I uptake outside the thyroid bed on the first postablation radioiodine scan, the intermediate-risk group shows 131I uptake in the neck outside the thyroid bed on the postablation scan, and the high-risk group shows 131I uptake in distant metastases on the first postablation scan. In our study, SPECT/CT changed the risk classification for 7 of the 109 postsurgical patients, thereby altering the methods and intensity of required follow-up assessment. This number may appear low. However, findings on 131I scans and lymph node status are only 2 factors in the assignment of ATA risk. For example, a patient with the tall cell variant of papillary carcinoma is considered to be at intermediate risk based on histology, regardless of a potential change in nodal status from N0 (planar scan) to N+ (SPECT/CT scan). Similarly, a patient with gross extrathyroidal extension in the histopathologic specimen is always considered to be at high risk (with or without distant metastases noted clinically or at imaging). Therefore, although SPECT/CT better defined individual lesions, it often did not change the ATA risk. One other reason for the low frequency of change in risk classification is the fact that we do not administer 131I routinely in low-risk patients who had total or near-total thyroidectomy in the hands of experienced head and neck surgeons at our center. Therefore, our patient population is preselected and would largely include patients at intermediate and high risk, in whom 131I therapy is considered essential. Thus, it would be nearly impossible for SPECT/CT to change a patient's risk classification from low to any higher grade because patients at low risk (based on clinical and histopathologic features) are not usually referred to our nuclear medicine clinic.
Our study had some limitations. For instance, patient follow-up is too short to assess clinical outcome (probably 5–10 y would be necessary). Thus, we do not know if all SPECT/CT-based management decisions were appropriate. However, in a smaller study of 55 postsurgical patients, Aide et al. (10) showed that a positive posttherapy SPECT/CT finding predicted treatment failure at 2 y better than did a positive whole-body planar scan. We do not know if surgical procedures or other therapeutic interventions were avoided or altered. However, scan findings are just 1 factor in clinical decision making. For instance, identification of nodal disease on posttherapy scans will alter risk classification but may not automatically trigger neck dissection, especially with small nodal volume. In our retrospective analysis, only 1 physician made all the decisions regarding appropriate patient management based on either planar scan findings or SPECT/CT findings. This may introduce bias because physician preference and clinical practice patterns may vary (e.g., work-up of findings on posttherapy scan); however, this bias is mitigated by the fact that the same bias was applied uniformly to all patients. Our results chiefly apply to patients in the intermediate- and high-risk groups. As stated before, at our institution most low-risk patients are not treated with 131I; the utility of SPECT/CT in this setting remains uncertain, but we believe that it would likely be low. We acknowledge that the accuracy and predictive power of the new ATA risk stratification remain to be proven. Finally, although it is conceivable that our approach may save costs by eliminating dedicated additional imaging studies, the issue of cost-effectiveness should be addressed in future work.
CONCLUSION
SPECT/CT significantly reduced the number of equivocal findings on posttherapy planar 131I scans and enabled more accurate characterization of focal iodine accumulation in 20% of patients. This improved accuracy helped avoid additional imaging studies in 48% of patients for whom they would have been necessary based on planar scans alone and led to a change in ATA risk classification in 6.5% of our intermediate- and high-risk patients, with implications for follow-up. Therefore, we recommend that SPECT/CT be strongly considered in intermediate- and high-risk patients after treatment with 131I. We now perform SPECT/CT in all posttherapy patients and believe that this has streamlined patient management and avoided additional imaging studies at later time points.
Footnotes
↵* Contributed equally to this work.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication February 4, 2010.
- Accepted for publication May 11, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}