


Abstract
Double-phase single-tracer scintigraphy with 99mTc-sestamibi is now generally used for parathyroid imaging but, at least in endemic goiter areas, complementary thyroid scintigraphy is recommended. Although 123I-sodium iodide is considered to be the optimal thyroid agent, it is hardly ever used because of high costs and logistic difficulties. Our study presents the results of using the 99mTc-sestamibi/123I subtraction technique in a region with a high goiter prevalence. Special attention was paid to the changes in sensitivity and specificity and their relationship to thyroid volume as well as to autonomous and nodular thyroid disease. Methods: One hundred three scintigraphic parathyroid examinations on 96 patients were included in this study. Fifty-eight of all patients had concomitant morphologic or functional alterations of the thyroid. Initially, 10 MBq 123I-sodium iodide were injected. Then, 150 MBq 99mTc-sestamibi were administered after 3–5 h, followed by planar scintigraphic imaging of the neck and upper chest region using a double-isotope technique. Results: An area with increased tracer uptake on the subtraction image was found in 44 cases. Forty-three of them proved to be true-positive. No suspicious lesions were detected scintigraphically on the remaining 59 examinations. However, histologic examination revealed a parathyroid adenoma or hyperplasia in 11 of these cases. The mean parathyroid volume of these false-negative patients was 0.9 mL. Secondary hyperparathyroidism with multiple enlarged parathyroid glands was found in 4 of these cases. The sensitivity of the parathyroid scintigraphy was 80% (43/54) and the specificity was 98% (48/49). There was a distinct difference in the sensitivity between the subgroups with thyroid volumes of >15 mL and <15 mL (76% vs. 88%), although the resected parathyroid glands had a similar size in both subgroups. The specificity was 97% and 100%, respectively. No significant difference in the sensitivity and specificity was observed between the subgroups with and without morphologic or functional alterations of the thyroid (80% vs. 79% and 96% vs. 100%, respectively). Conclusion: The sensitivity of parathyroid imaging with 99mTc-sestamibi/ 123I subtraction depends mainly on the thyroid and parathyroid volumes rather than on the presence of nodular or autonomous thyroid disease.
The dual-tracer subtraction technique using 201Tl-thallous chloride and 99mTc-pertechnetate, which was already published in 1983 (1), was the first practicable method for parathyroid imaging. In 1989, 99mTc-sestamibi was introduced as a replacement for 201Tl in conjunction with 99mTc-pertechnetate or 123I-sodium iodide (2) and later on proved to have at least a similar efficiency (3). Because the washout rate of 99mTc-sestamibi from parathyroid adenomas was found to be slower relative to that of thyroid tissue, a single-radionuclide double-phase imaging procedure using early and late acquisitions was suggested in 1992 (4) and is now widely used. However, many investigators found that this difference in the kinetics of 99mTc-sestamibi could not be observed in all parathyroid adenomas and, hence, consider complementary thyroid scintigraphy to be mandatory (5–7). Already in 1987, an early study revealed that the combination of 201Tl and 123I may lead to improved detection, especially of low-weight abnormal parathyroid glands, in comparison with the original procedure using 201Tl and 99mTc-pertechnetate (8). Subsequently, the combination of 99mTc-sestamibi and 123I was found to provide better results than those of the single-radionuclide double-phase imaging procedure with 99mTc-sestamibi (9–11) or the 201Tl/ 99mTc-pertechnetate subtraction method (12–14), especially in uremic patients with secondary hyperparathyroidism (15,16). It further provides a higher sensitivity for the detection of parathyroid abnormalities than high-resolution sonography (17,18). Therefore, a 99mTc-sestamibi/ 123I subtraction scan has also been recommended for preoperative localization of abnormal parathyroid glands before initial neck exploration to reduce the average surgery time (19,20) or to support less invasive and less expensive procedures (e.g., unilateral neck exploration or even a limited dissection under local anesthesia) (21). Because associated nodular thyroid disease may lead to false-positive results with the 99mTc-sestamibi single-radionuclide protocol, complementary thyroid imaging is recommended particularly in endemic goiter areas (22), and 123I is considered to be the optimal thyroid agent for dual-tracer parathyroid imaging (21). Unlike 99mTc-pertechnetate, 123I allows delayed thyroid images providing a better contrast, especially in patients under suppressive hormone medication or after recent administration of radiographic contrast material, and hence leads to a higher predictive value regarding autonomous tissue. Furthermore, motion artifacts and prolonged immobilization can be avoided with simultaneous double-window recording of 99mTc-sestamibi and 123I instead of successive image acquisition (10). However, logistic difficulties along with the higher costs of 123I constitute a shortcoming of the method, which explain its limited use.
Our study presents the results of using the 99mTc-sestamibi/ 123I subtraction method in a region with a high goiter prevalence. Special attention was paid to the changes in sensitivity and specificity and their relationship to thyroid and parathyroid volumes, thyroid nodular disease, and autonomous thyroid adenomas.
MATERIALS AND METHODS
One hundred three scintigraphic parathyroid examinations on 96 consecutive patients (69 women, 27 men), submitted because of hypercalcemia and suspected hyperparathyroidism, were included in this study. Twenty of them (16 women, 4 men), suffering from chronic renal failure and receiving hemodialysis, were referred with suspected secondary hyperparathyroidism. The average thyroid volume in the entire population was 24.6 mL. Eighteen patients had already undergone thyroid surgery before the parathyroid imaging was performed. The average thyroid volume in this subgroup was 6.8 mL (range, 0.5–35 mL). One patient with a thyroid volume of 2.0 mL underwent radioiodine therapy 19 y earlier. The mean thyroid volume in the remaining 84 cases without previous intervention was 28.7 mL (range, 2.4–122 mL). All thyroid volumes were detected by sonography. Fifty-eight of all patients had concomitant nodular thyroid disease; 19 patients presented with autonomous thyroid adenomas. The results of 52 scintigraphic examinations were verified by subsequent surgery. In the remaining 51 cases, scintigraphic findings were validated by a follow-up period (average, 3.3 y) with clinical observation as well as determination of the serum concentrations of calcium and parathormone.
Three to 5 h after injection of 10 MBq 123I-sodium iodide, 150 MBq 99mTc-sestamibi were administered intravenously. Fifteen minutes later, planar scintigraphic images of the neck and upper chest region were obtained with a large-field-of-view gamma camera (APEX-SPX equipped with a low-energy, all-purpose, parallel-hole collimator; Elscint, Haifa, Israel) in the double-isotope technique, using a 128 × 128 pixel matrix. The energy windows were set to 140 keV ± 5% and 159 keV ± 5%, respectively. Phantom studies revealed the scatter of 99mTc contaminating the iodine window to be <1% and the scatter of 123I in the technetium window to be <10% with these settings. The acquisition time in the patient studies was 15 min. Increasing fractions of the iodine scintigram were then subtracted from the sestamibi image to attenuate the thyroid activity in the resulting image until the body of the thyroid disappeared. The final images were investigated visually for focal areas of increased uptake. All interpretations were performed by 2 experienced nuclear medicine physicians. In a few cases, the results of a sonographic examination were available to the investigator. In most cases, however, the investigators were unaware of the findings of previous examinations.
RESULTS
Fifty-two surgical interventions were performed on 49 patients. In 46 cases, a parathyroid adenoma or parathyroid hyperplasia was documented by histopathologic examination. The mean volume of the resected parathyroid glands was 2.7 mL (range, 0.1–14 mL). In 6 patients, who underwent surgery primarily for multinodular goiter, the presence of an adenoma or hyperplasia of the parathyroid glands could be excluded. The outcome of the remaining 51 cases was validated by clinical follow-up. Eight patients with scintigraphically detected parathyroid adenoma refused surgical intervention. They were considered to be true-positive because they showed continuously elevated calcium and parathormone levels during the follow-up period, and no other cause for these findings could be identified. In 39 cases, a different reason for the hypercalcemia was found later, and these patients presented with no more symptoms after adequate therapy. In these negative cases, additional hyperparathyroidism was excluded in the clinical observation period. Four patients underwent a second parathyroid scintigraphic examination after successful resection of the adenoma. No pathologic finding was revealed in any of these cases. Because these patients also presented a normal follow-up, they were classified as true-negative.
In 44 cases, scintigraphic examination revealed an area with increased tracer uptake on the subtraction image. Forty-three of them proved to be true-positive (35 were confirmed surgically, 8 were confirmed on clinical follow-up). The mean thyroid volume in these cases was 23.6 mL (range, 0.5–89 mL); the average volume of the detected parathyroid glands was 3.6 mL (range, 0.1–14 mL). In the subgroup that refused surgical intervention, the parathyroid volume was taken from sonography. The smallest resected parathyroid adenoma with a volume of 0.1 mL was found in a thyroid with a volume of 11.5 mL without nodular or autonomous disease. The only false-positive patient had a large multinodular goiter with a volume of 122 mL and multiple autonomous thyroid adenomas. In the remaining 59 examinations, no suspicious lesions were detected scintigraphically. However, in 11 of these cases belonging to a group of 16 patients who had to undergo surgery for multinodular goiter, histologic examination revealed a parathyroid adenoma or hyperplasia. The mean thyroid volume of these false-negative cases was 27.5 mL (range, 4.2–68 mL); the average volume of the resected parathyroid glands was 0.9 mL (range, 0.1–3.3 mL). Secondary hyperparathyroidism with multiple enlarged parathyroid glands due to chronic renal failure rather than a single adenoma was found in 4 of these cases. The remaining 48 cases of the scintigraphically negative group proved to be true-negative in the clinical follow-up period. The sensitivity of the parathyroid scintigraphy was 80% (43/54), the specificity was 98% (48/49), the positive predictive value was 98% (43/ 44), and the negative predictive value was 81% (48/59). The overall accuracy of the method was 88% (91/103).
When considering the subgroup with a thyroid volume of <15 mL (n = 34; average parathyroid volume, 1.5 mL [range, 0.1–14.0 mL]; average thyroid volume, 7.4 mL [range, 0.5–14.5 mL]), the sensitivity of the parathyroid imaging was 88% (14/16). The subgroup with a thyroid volume of >15 mL (n = 69; average parathyroid volume, 1.3 mL [range, 0.1–14.0 mL]; average thyroid volume, 33.1 mL [range, 15.3–122 mL]) showed a sensitivity of only 76% (29/38). The Wilcoxon rank sum test revealed no significant difference between the volumes of the parathyroid glands in both subgroups (P > 0.5). On the other hand, the subgroup of the entire patient population without nodular or autonomous thyroid disease (n = 45; average parathyroid volume, 1.5 mL [range, 0.1–14 mL]; average thyroid volume, 13.4 mL [range, 0.5–50 mL]) showed a sensitivity of 79% (19/24), which does not differ significantly from that of the remaining cases (n = 58; average parathyroid volume, 1.2 mL [range, 0.1–8.0 mL]; average thyroid volume, 33.3 mL [range, 2.0–122 mL]) with a value of 80% (24/30). The thyroid volume in the subgroup with nodular and autonomous disease was greater than that in the first (P < 0.001), but there was no significant difference between the parathyroid volumes (P > 0.2). Table 1 summarizes all statistical results of these subgroups. A comparison of the sensitivity and specificity is presented in Figure 1.

Comparison of sensitivity and specificity for scintigraphic detection of abnormal parathyroid glands in different subgroups. Results show decreasing sensitivity with increasing thyroid volume. Outcome is not influenced by nodular and autonomous thyroid disease.
Statistical Analysis of Entire Patient Population and Subgroups
When dividing the collective group with proven hyperparathyroidism into 2 subgroups with parathyroid volumes of >1 mL and <1 mL, the sensitivity was 86% (25/29) in the first group (n = 29; average parathyroid volume, 4.3 mL [range, 1.1–14 mL]; average thyroid volume, 28.4 mL [range, 0.5–89 mL]; 19 cases with thyroid nodules, 4 cases with autonomous thyroid disease) and 72% (18/25) in the second group (n = 25; average parathyroid volume, 0.5 mL [range, 0.1–0.9 mL]; average thyroid volume, 19.9 mL [range, 1.2–44 mL]; 11 cases with thyroid nodules, 4 cases with autonomous thyroid disease). There was no significant difference between the thyroid volumes of both groups (P > 0.1).
DISCUSSION
Our results suggest that parathyroid scintigraphy with the 99mTc-sestamibi/123I subtraction method is hardly affected by nodular or autonomous thyroid disease. The sensitivity and specificity in the subgroups with and without morphologic and functional alterations were similar, although the first group also showed a greater average thyroid volume. The only false-positive patient had a large multinodular goiter (122 mL) with multifocal thyroid autonomy.
The volume of the thyroid gland as well as that of the parathyroid glands influenced mainly the detection rate. Although some very small parathyroid adenomas with a volume as low as 0.1 mL could be located scintigraphically, this was possible primarily in thyroid glands with a normal or reduced size or in case of an extrathyroidal location of the adenoma. In the other cases, a small volume with mismatch in the uptake of 99mTc-sestamibi and 123I due to a parathyroid lesion is likely to be masked by the large thyroid mass, especially if the respective parathyroid gland is located behind the thyroid contour. Interestingly, in 1 patient the parathyroid adenoma accidentally remained after the initial surgery; only nodular lesions of the thyroid itself were resected. Because of continuously elevated parathormone levels, another 99mTc-sestamibi/123I subtraction scintigraphic examination was performed after this operation, which showed the parathyroid adenoma in exactly the same location. However, the contrast was now much better after removal of the surrounding thyroid tissue. Figures 2 and 3 show the scintigraphic images before and after thyroid resection.

Parathyroid scintigraphy in patient with moderate nodular goiter and solitary left inferior parathyroid adenoma, partly overlying thyroid contour (arrows), before initial surgery. MIBI = methoxyisobutylisonitrile.
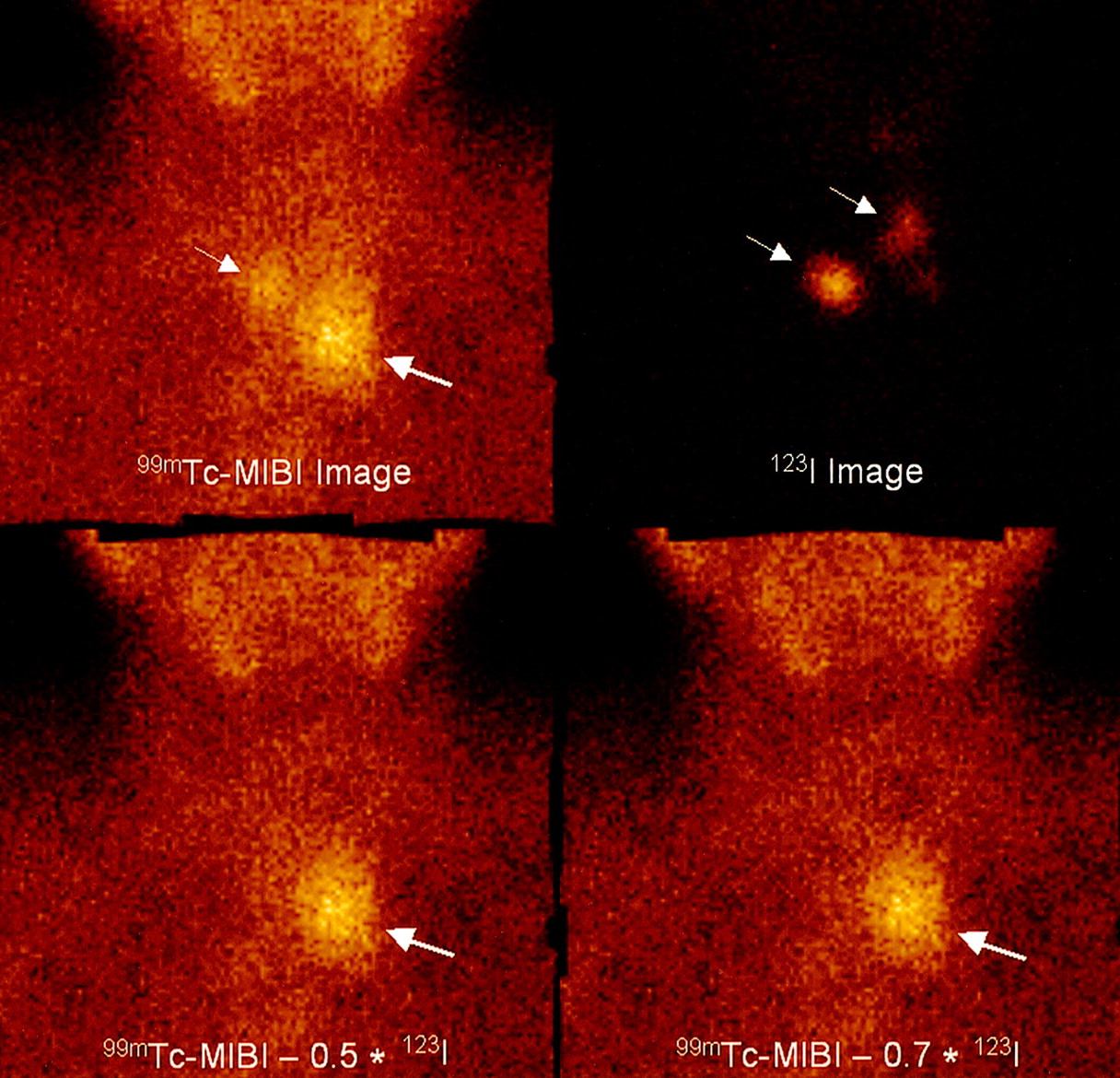
Thyroid remnants after resection (small arrows) with remaining left inferior parathyroid adenoma (large arrows). Subtraction images show markedly better contrast of the parathyroid adenoma without overlying thyroid tissue. MIBI = methoxyisobutylisonitrile.
Basically, a limited sensitivity of parathyroid scintigraphy due to overlying thyroid tissue does not seem to affect the common therapeutic approach because a large goiter already constitutes an indication for surgery. The parathyroid glands can easily be explored and resected in the same session by an experienced surgeon as long as they are placed in the typical locations. In many cases less invasive procedures, such as unilateral neck exploration or even more limited dissections, which mainly constitute the indication for parathyroid scintigraphy before the initial operation, cannot be performed anyway. Therefore, in the endemic goiter area, scintigraphy plays an important role especially in cases of suspected parathyroid adenoma in ectopic sites distant from the thyroid. The sensitivity of the scintigraphic imaging should not be affected then as long as a sufficient counting rate is acquired and the subtraction image is also carefully inspected for focal areas with only slightly increased uptake using various window settings.
Nevertheless, with the ongoing development of less invasive surgical approaches, parathyroid scintigraphy seems to be in need of a further optimization to support these modalities even in nodular goiters. Variations of the imaging technique, such as use of a pinhole collimator or side views, may be beneficial in certain cases. Many of the patients referred to our department are taking thyroid hormone medication and, hence, show a suppressed iodine uptake. We also frequently see patients shortly after having received radiographic contrast material. Both lead to an iodine image of very low contrast, even if delayed scintigrams on the following day are acquired. In these cases, the methoxyisobutylisonitrile image already shows a much higher intensity with the relatively low activity of 150 MBq. On the other hand, a higher activity of 99mTc-sestamibi or iodine could be beneficial in unsuppressed goiters to compensate for the higher absorption of large thyroid volumes. Thus, an individual adaptation of the ratio between the administered iodine and methoxyisobutylisonitrile activities, depending on thyroid volume, the presence of nodular or autonomous disease, thyroid medication, or administration of radiographic contrast material may allow a further optimization of the procedure.
CONCLUSION
Parathyroid imaging with 99mTc-sestamibi/123I subtraction provides a high specificity even in large multinodular goiters with autonomous disease. The sensitivity of parathyroid imaging with 99mTc-sestamibi/123I subtraction depends primarily on the thyroid and parathyroid volumes rather than on the presence of morphologic or functional alterations.
Footnotes
Received Oct. 22, 2001; revision accepted Apr. 26, 2002.
For correspondence or reprints contact: Thomas Rink, MD, Department of Nuclear Medicine, Municipal Hospital, Leimenstrasse 20, 63450 Hanau, Germany.
E-mail: Rink@em.uni-frankfurt.de




{kind=link}
{kind=link}
{kind=link}