


Abstract
Physiologic 18F-FDG uptake in areas of supraclavicular fat in humans (“USA-Fat”) has recently been recognized as 18F-FDG uptake in apparent brown adipose tissue (BAT) using fused PET/CT technology. In this study, we evaluated 18F-FDG uptake in BAT of rats to determine whether pharmacologic or physiologic interventions affect the uptake, knowing that BAT has a high density of adrenergic innervation. Methods: Seven- to 8-wk-old female Lewis rats receiving intravenous 18F-FDG injections were examined under various conditions to evaluate 18F-FDG biodistribution into interscapular BAT and major organs. In series 1, rats were given ketamine-based anesthesia or were exposed to cold (4°C for 4 h) to determine whether these interventions increased 18F-FDG uptake in BAT. In series 2, anesthetized rats (ketamine-based anesthesia) were given propranolol, reserpine, or diazepam intraperitoneally before 18F-FDG injection to determine whether the drug reduced 18F-FDG uptake in BAT. The control and treated groups in series 2 were also evaluated with 18F-FDG PET/CT imaging. Results: In series 1, anesthesia or exposure to cold increased 18F-FDG uptake in BAT to levels 14-fold and 4.9-fold, respectively, greater than the control nonstimulated values. BAT uptake was high, comparable to that in the brain. In series 2, 18F-FDG uptake in BAT was significantly decreased to less than 30% of the control level after propranolol or reserpine (P < 0.05). Diazepam did not significantly decrease 18F-FDG uptake in BAT. 18F-FDG PET/CT findings reflected these biodistribution data: The control and diazepam groups exhibited intense 18F-FDG uptake in BAT, whereas the propranolol and reserpine groups showed only faint to mild 18F-FDG uptake in BAT. Among several organs whose 18F-FDG uptake was affected after predosing drugs, the heart exhibited considerable decreases in tracer uptake with propranolol or reserpine. Conclusion: This rodent study demonstrated that BAT can exhibit high 18F-FDG uptake under stimulated conditions including exposure to cold and that propranolol or reserpine treatment can remarkably reduce the high 18F-FDG uptake in BAT. The effect of these drugs on 18F-FDG uptake in human BAT, as well as on tracer accumulation in other organs, should carefully be evaluated clinically to minimize the USA-Fat artifact.
The advent of fused PET/CT technology has enabled the determination that nonmalignant 18F-FDG uptake is seen clinically in areas of supraclavicular fat (“USA-Fat”) and in other areas of fat (1,2). If not properly recognized, 18F-FDG uptake in these areas may falsely be interpreted as a positive PET finding and may sometimes be indistinguishable from 18F-FDG uptake in lymph nodes, potentially leading to false-negative or -positive findings. The USA-Fat finding has been reported to occur in 2.5%–4.0% of patients undergoing 18F-FDG PET/CT studies, is more common in women, is more common in winter, and now is considered to correspond to uptake in brown adipose tissue (BAT) (1,2).
BAT functions as a thermogenic organ by producing heat to maintain body temperature in many mammals, especially in the young (3,4). BAT is generally in deep cervical regions, including the supraclavicular areas, the interscapular and paravertebral regions, and areas near large vessels. BAT requires glucose not as a direct source of heat production but as a source of adenosine triphosphate. The adenosine triphosphate resulting from glycolysis is required for continued fatty acid oxidation in the mitochondrial uncoupling proteins in BAT, which is a main mechanism for heat production (5). BAT is innervated by the sympathetic nervous system and expresses β1-, β2-, and β3-adrenergic receptors, among which the β3-adrenergic receptor is predominant. BAT is known to exhibit increased glucose uptake when the sympathetic nervous system is activated by cold stimulation and other causes.
In the present study, we evaluated 18F-FDG uptake in the BAT of rats using a biodistribution technique to determine whether pharmacologic or physiologic interventions designed largely to alter adrenergic innervations affect 18F-FDG uptake. We also studied 18F-FDG uptake in BAT using a clinical PET/CT scanner to noninvasively demonstrate whether the administered drugs decrease the 18F-FDG uptake visualized on imaging.
MATERIALS AND METHODS
Seven- to 8-wk-old female Lewis rats (mean body weight, 185 g) were used in this study. Rats are known to have a relatively large amount of BAT in the interscapular region and thus are often used in research dealing with BAT (6,7). This study was performed as a part of the project that has been approved by the animal research committee at the Johns Hopkins Medical Institutions.
Biodistribution Study
In this study, we evaluated 2 matters: whether anesthesia or exposure to cold could increase 18F-FDG uptake by stimulating BAT activity (series 1) and whether the increased 18F-FDG uptake in stimulated BAT could be reduced by pharmacologic interventions (series 2). In the anesthesia group in series 1 and in all groups in series 2, we anesthetized the rats with a cocktail of ketamine and acepromazine (ketamine is known to stimulate the sympathetic nervous system) (8). The same anesthetics were used in the PET/CT imaging studies, which were performed under the same conditions as for series 2. The rats were divided into 3 and 4 groups (n = 4–5 rats each) in series 1 and 2, respectively, and each group received varying pharmacologic or physiologic interventions to modulate BAT metabolic activity.
In all groups in series 1 and 2, each rat received 7.4 MBq of 18F-FDG via the tail vein after overnight fasting. In series 1, the rats in the nonstimulation group received only the 18F-FDG injection. In the anesthesia group, each rat was given intraperitoneal anesthesia composed of ketamine, 30 mg/kg of body weight, and acepromazine, 1.0 mg/kg of body weight, before the 18F-FDG injection. For the cold-exposure group, rats were kept in a cold room (4°C) for 4 h before the 18F-FDG injection. In series 2, the propranolol, reserpine, and diazepam groups were given each drug intraperitoneally after anesthesia, followed by 18F-FDG injection, under the protocol as follows: propranolol, 5 mg/kg of body weight 20 min before 18F-FDG injection; reserpine, 4 mg/kg of body weight 4 h before 18F-FDG injection; and diazepam, 2.5 mg/kg of body weight 30 min before 18F-FDG injection. The dose and time of injection for each drug were determined according to published articles reporting the expected time of onset and maximal pharmacologic effect on target tissues (7,9,10). The control rats in series 2 were defined as those treated only with the anesthetics, since all rats in this group were evaluated under anesthesia.
All rats were sacrificed 60 min after 18F-FDG injection. Blood, major organs, back muscle, interscapular BAT, and white adipose tissue (WAT) surrounding the BAT were removed, and their radioactivity concentrations were counted. The percentage injected dose (%ID) per gram of tissue, standardized by kilogram of body weight (%ID/[g of tissue] × [kg of body weight]), was calculated and compared among tissues. In series 1, all procedures other than the exposure to cold were performed at room temperature in a climate-controlled room. Only commercially available drugs approved by the U.S. Food and Drug Administration were assessed in this study, in view of their potential for clinical application to humans.
To confirm that the soft tissue we considered as interscapular BAT was BAT, histologic (hematoxylin–eosin staining) and immunohistochemical evaluation was performed on a sample obtained from a rat under the same conditions as for the nonstimulation group in series 1 (without 18F-FDG injection). The antimitochondrial uncoupling protein 1 (UCP-1) antibody was used for the immunohistochemical evaluation, since UCP-1 is known to be observed solely in BAT (11). Antibody staining was performed according to the avidin–biotin–peroxidase (avidin–biotin complex, or ABC) method using a dewaxed 5-μm-thick slide provided from a formalin-fixed, paraffin-embedded sample. The details of this procedure were described elsewhere (12). The polyclonal rabbit anti–UCP-1 antibody 1:300 (Sigma) was used as a primary antibody. Samples were reviewed by light microscopy to determine whether brown-stained fat tissue was present.
18F-FDG PET/CT Imaging
The control and pharmacologic intervention groups in series 2 (n = 3 rats each) also underwent 18F-FDG PET/CT imaging studies, separately from the biodistribution study. Each rat received 18.5 MBq of 18F-FDG via the tail vein after anesthesia (cocktail of ketamine, 75 mg/kg of body weight, and acepromazine, 2.5 mg/kg of body weight, intraperitoneally) and overnight fasting. About 60 min later, the rats were imaged with a combined PET/CT scanner (Discovery LS; GE Medical Systems) originally designed for human imaging, using a rat-specific protocol (13). In brief, CT for attenuation correction and 10-min emission PET were performed, followed by thin-slice (1.25-mm-thick) CT. PET and thin-slice CT images were reconstructed as 35-cm field-of-view images, and the PET and CT image sections at the same location were manually fused using image analysis software (Photoshop 6.0; Adobe Systems Inc.). The mild 18F-FDG uptake in skin, along with the contours of normal organs, were used as landmarks. The PET and CT images were also intrinsically registered because of their acquisition on the dedicated PET/CT scanner. This manual fusion process was required because the available scanner software fuses only with 5-mm-thick CT images. 18F-FDG uptake in interscapular BAT was evaluated using the PET, CT, and fused PET/CT images.
Statistical Analysis
The data on %ID/(g of tissue) × (kg of body weight) for the drug-administration or cold-exposure group were compared with the nonstimulation (series 1) or control (series 2) data within each series using the Mann–Whitney U test. A P value of less than 0.05 was considered statistically significant.
RESULTS
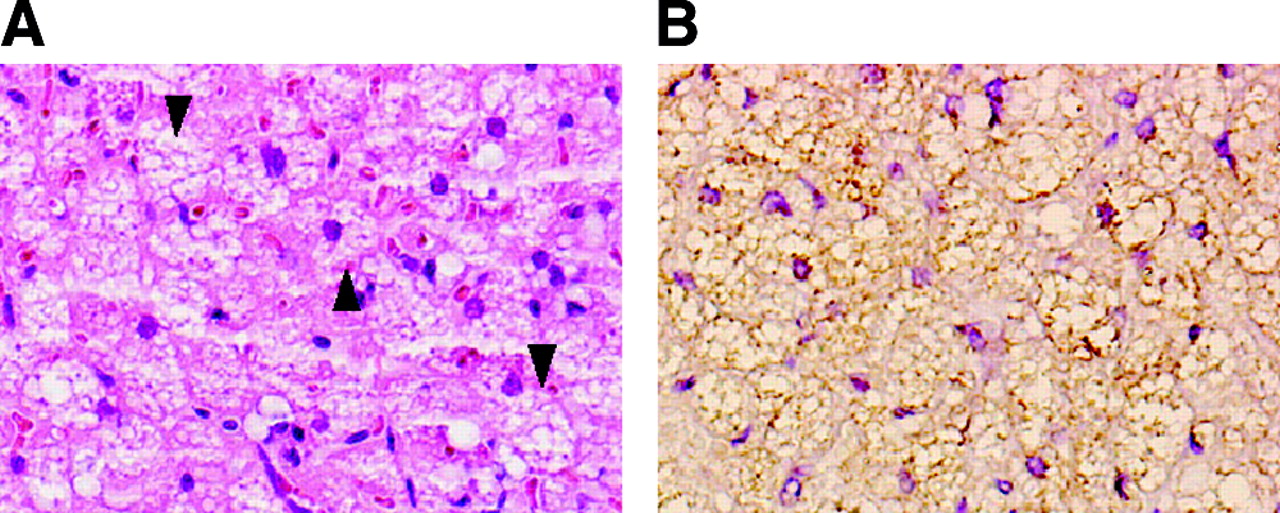
Interscapular BAT was easily located in each rat at the time of dissection. Interscapular BAT in the anesthesia and cold-exposure groups in series 1 and in the control group (all were anesthetized) in series 2, all of which were considered to be under BAT-stimulating conditions, was reddish brown on direct visual inspection, whereas interscapular BAT in the nonstimulated group in series 1 and the pharmacologic intervention groups in series 2 was whitish brown and obviously less extensive than the reddish-brown interscapular BAT. Figure 1 shows the results of staining interscapular BAT with hematoxylin–eosin and anti–UCP-1 antibody. The soft tissue was filled with multilocular cells positive for the anti–UCP-1 antibody, confirming that the tissue really was BAT.
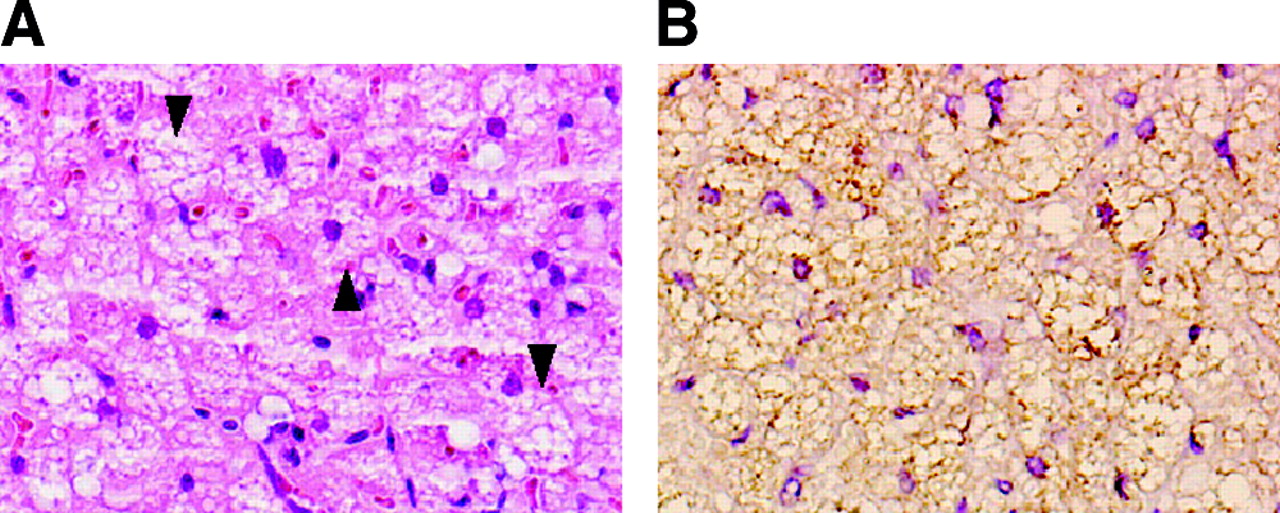
BAT soft-tissue sections stained with hematoxylin–eosin (A) and anti–UCP-1 antibody plus hematoxylin (B). The tissue was filled with multilocular cells (examples indicated by arrowheads), which were positive for the anti–UCP-1 antibody (brown color), consistent with brown fat (×200).
The %ID/(g of interscapular BAT tissue) × (kg of body weight) in the nonstimulated group (without any drugs) showed moderately high 18F-FDG uptake, compared with uptake in normal organs in series 1. In the anesthesia group, BAT exhibited very high 18F-FDG uptake—14-fold greater than the nonstimulated values and the highest of all normal organs. Several organs showed increases in 18F-FDG uptake. The heart and WAT showed, respectively, a 6-fold and a 3-fold increase over nonanesthetized values, but other organs showed a 2-fold or lower increase. Cold exposure 4 h before 18F-FDG injection also increased uptake in BAT (to 4.9-fold the nonstimulation values), but the increase was less than that in the anesthesia group. No other organs in this group showed more than a 1.5-fold increase in 18F-FDG uptake.
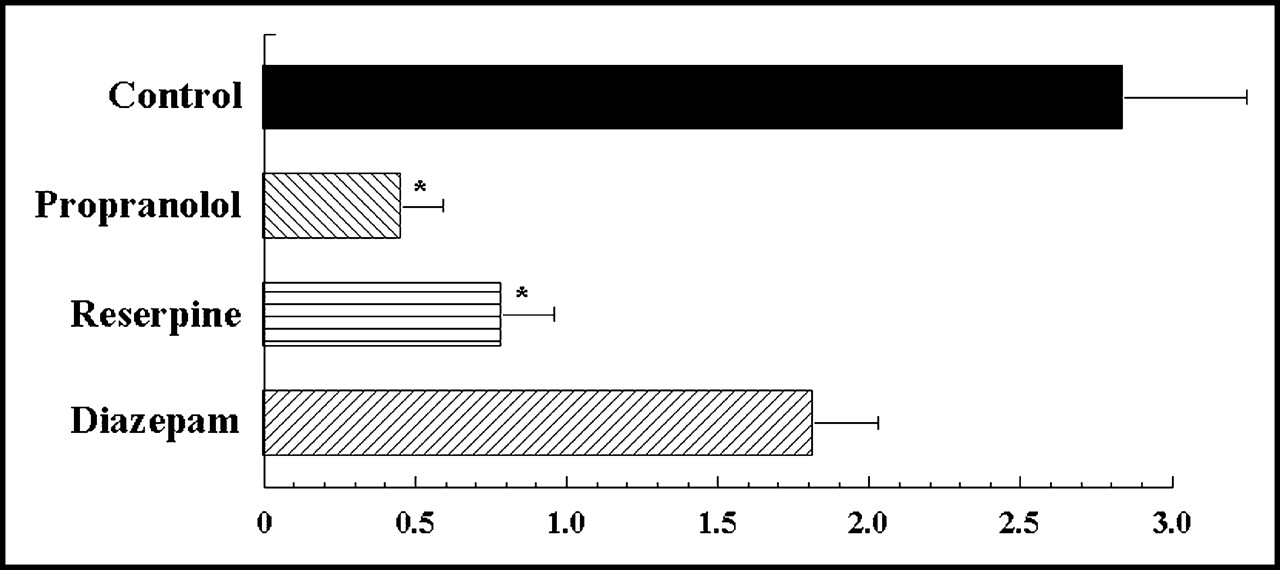
The data on %ID/(g of tissue) × (kg of body weight) in series 2 are shown in Table 1. The data on interscapular BAT in series 2 are summarized in Figure 2. BAT in the control group (with the anesthetics) showed very high 18F-FDG uptake, the highest of all normal organs. Propranolol or reserpine pretreatment significantly decreased 18F-FDG uptake in interscapular BAT—to 16% and 28% of the control values (P < 0.05), respectively. After diazepam, the 18F-FDG uptake was 64% of the control values, but this modest decline was not statistically significant (P = 0.46). Changes in 18F-FDG uptake were observed in various samples other than BAT in the drug administration groups, mainly in the propranolol group. Blood and liver in the reserpine group exhibited substantial increases in 18F-FDG uptake, whereas heart in the propranolol and reserpine groups and muscle in the propranolol group showed notable decreases in 18F-FDG uptake. The decreases of 18F-FDG uptake values in heart were considerable in the propranolol and reserpine groups, at 30% and 40% of the control values, respectively.

%ID/(g of tissue) × (kg of body weight) for BAT in series 2 (with ketamine-based anesthesia). 18F-FDG uptake in the control group was high, the highest of all normal organs in this group. Propranolol and reserpine significantly decreased 18F-FDG uptake in BAT, to 16% and 28% of the control values, respectively. Diazepam also decreased 18F-FDG uptake, to 64% of the control values, but statistical significance was not achieved. *P < 0.05.
Results of Series 2 Biodistribution Studies
PET/CT imaging clearly demonstrated intense 18F-FDG uptake in the interscapular BAT of a representative control rat, which was considered to be under conditions of increased uncoupling activity (Fig. 3). In the propranolol- and reserpine-treated groups, BAT exhibited only faint to mild 18F-FDG uptake (Fig. 3), whereas the brain showed the expected intense 18F-FDG uptake similar to that of the control group. However, in the diazepam group, BAT exhibited intense 18F-FDG uptake (Fig. 3), which was similar to the uptake in the brain. Thus, the PET/CT imaging findings were concordant with the biodistribution results in series 2.
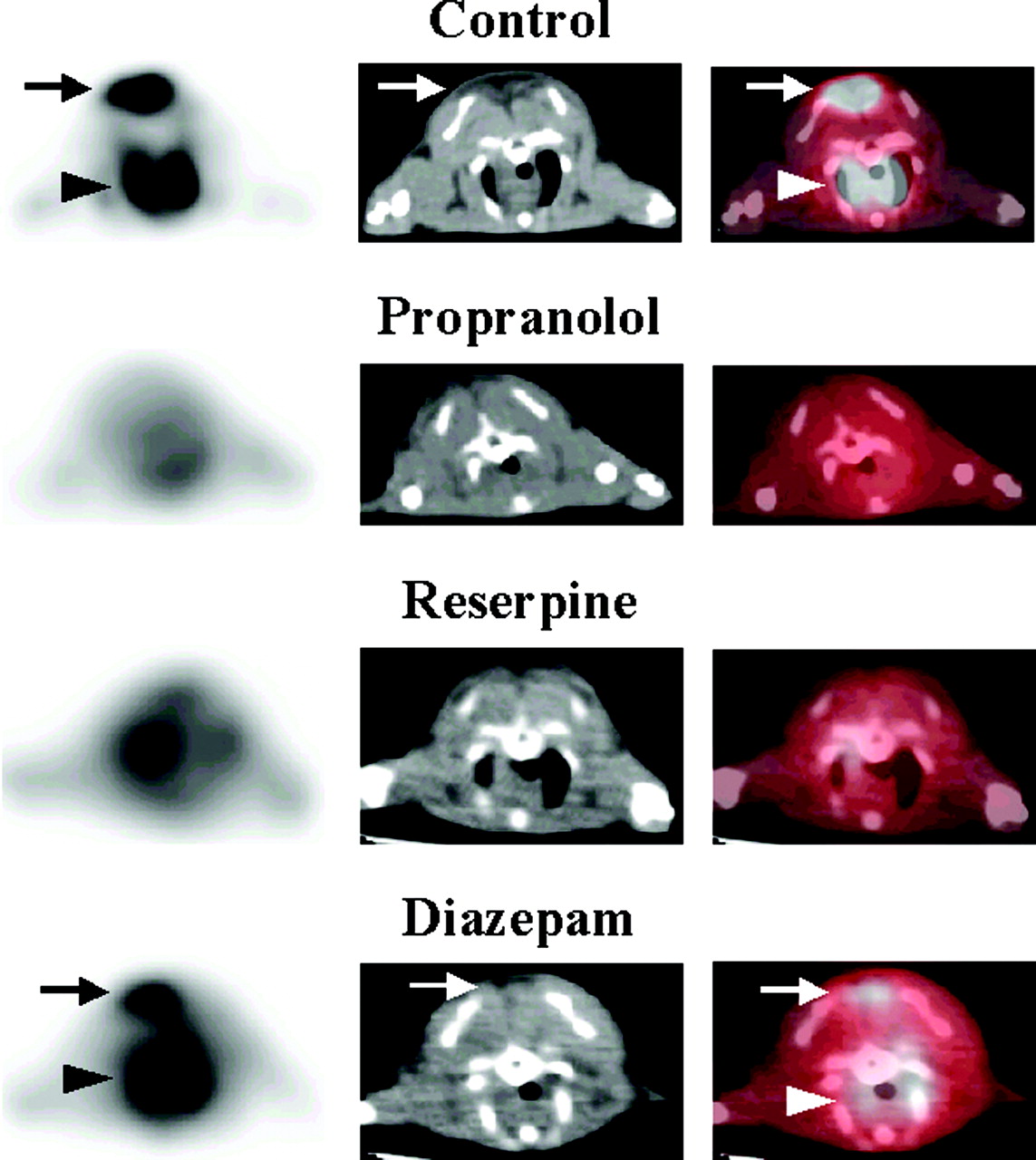
PET (left), CT (middle), and fused PET/CT (right) images of rats with or without predosing drugs in series 2 (with ketamine-based anesthesia). Intense 18F-FDG uptake (arrow on PET and PET/CT) was observed in the interscapular BAT (arrow on CT) in the control group. No significant 18F-FDG uptake was observed in the propranolol and reserpine groups. In the diazepam group, intense 18F-FDG uptake (arrow on PET and PET/CT) was still observed in the interscapular BAT (arrow on CT). The artifact (arrowhead on PET and PET/CT), which was probably caused by intense 18F-FDG uptake in the heart shining through to this slice, was also observed only in the control and diazepam groups.
DISCUSSION
In this study, we demonstrated that BAT in rats exhibits high 18F-FDG uptake, especially under stimulated uncoupling conditions. 18F-FDG uptake in BAT was extremely high after ketamine-based anesthesia, which was presumed to have stimulated the sympathetic nervous system. 18F-FDG uptake with anesthesia was 14-fold that without anesthesia and was highest of all samples. These results were reasonably consistent with the data published by Paul et al., the only available biodistribution data on 18F-FDG uptake in BAT in rats (14). Other studies demonstrated high 14C-deoxyglucose uptake in BAT in rats or mice (15–17). We also demonstrated this high 18F-FDG uptake in stimulated BAT in rats in PET/CT imaging studies. The intense 18F-FDG uptake in BAT was comparable visually to the intense tracer uptake in the brain and heart.
The intensity of 18F-FDG uptake in stimulated BAT appears to be high in humans as well. Cohade et al. reported that USA-Fat visually and semiquantitatively exhibited high 18F-FDG uptake that was quite comparable to the uptake in pathologic lymph nodes or soft-tissue masses in the supraclavicular areas (1). To avoid diagnostic errors, those who interpret 18F-FDG PET images must be cognizant of the possibility that BAT exhibits high 18F-FDG uptake.
All 3 drugs assessed in this study appeared to decrease 18F-FDG uptake in BAT on biodistribution data, in which high 18F-FDG uptake was observed in BAT in the control group (with the anesthetics alone), although the effect of diazepam did not reach a statistically significant level. Propranolol and reserpine decreased 18F-FDG uptake in BAT to less than 30% of the uptake in the control group. On PET/CT images, the decreased 18F-FDG uptake was demonstrated as faint to mild uptake, which was almost indistinguishable from the surrounding tissue uptake. Considering that reserpine considerably reduced 18F-FDG uptake in BAT on the PET/CT imaging study even if the values for %ID/(g of tissue) × (kg of body weight) were higher than those in the propranolol group, lower doses of propranolol may have been enough to minimize the 18F-FDG uptake in BAT. If used clinically, lower doses of propranolol, with the 18F-FDG–suppressing effect on BAT, would seem more desirable in view of the drug’s potential to affect the function of normal organs. In this study, we had to inject reserpine 4 h before 18F-FDG administration to deplete stores of norepinephrine in the nerve terminals at BAT, in accordance with the expected time course of drug action (7). Although this preclinical study provided potentially valuable information about the effectiveness of adrenergic blockade on 18F-FDG uptake in BAT, further studies are obviously required, especially about the optimal drug and its administration method, including the evaluation of drugs such as the recently developed β3-selective blockers (18).
In 1996, Barrington et al. reported that diazepam was useful to reduce symmetric “muscle” 18F-FDG uptake in the neck and paravertebral region of the thoracic spine (19). After examination by a fused PET/CT method, Hany et al. suspected the “muscle” findings to be due to BAT (2). Although we used a relatively high dose of diazepam (10), the effect of this drug on BAT was not clearly demonstrated in either biodistribution or 18F-FDG PET imaging in this study. In addition, in our clinical 18F-FDG PET/CT studies, we have experienced some patients whose USA-Fat findings did not diminish even after administration of diazepam. It is possible that in humans the central antianxiety effect of diazepam may relieve the sympathetic nervous system activity and thus reduce 18F-FDG uptake in BAT. The central antianxiety effect may not have been present in rats in this study. BAT has been reported to have benzodiazepine receptors (20), to which diazepam binds as an agonist. Nonetheless, in our rodent studies, propranolol or reserpine appears to be considerably more suitable than diazepam in reducing 18F-FDG uptake in BAT, since BAT is rich in β-adrenergic receptors.
A potential concern in the clinical use of propranolol or reserpine is the unwanted effect on the function of normal organs. Our study assessed changes in 18F-FDG uptake after drug administration. Many organ samples exhibited such changes. The heart exhibited a considerable decrease in 18F-FDG uptake both after propranolol and after reserpine. In the biodistribution studies, myocardial 18F-FDG uptake decreased to 30%–40% of control values for both the propranolol group and the reserpine group. PET/CT images demonstrated only mild 18F-FDG uptake in the heart in both groups. Muscle, spleen, and WAT should also be carefully evaluated in clinical situations according to the same biodistribution data. Although no reports are yet available regarding the effect of adrenergic blockade on 18F-FDG uptake in tumors, this effect should also be clarified in clinical situations, as some tumors, such as neuroendocrine tumors, are known to have adrenergic receptors. However, active tumors and inflammation generally show intense 18F-FDG uptake, regardless of BAT 18F-FDG uptake status, in our experience. This fact may suggest that 18F-FDG uptake in many tumors or in inflammation is independent of the adrenergic stimulation status.
Exposure to cold 4 h before 18F-FDG administration increased 18F-FDG uptake in BAT in series 1. Cohade et al. recently reported a higher incidence of USA-Fat findings in clinical 18F-FDG PET studies during the coldest period of the year (21). Hany et al. also postulated cold stress as a cause of this phenomenon (2). The results of this study support the association between increased 18F-FDG uptake in BAT and cold stress in clinical situations, although cold stress is not considered the only cause of the phenomenon. Because humans have much less BAT per body mass than do rats, keeping patients warm from before the 18F-FDG injection to the end of PET scanning may be effective for reducing the frequency of USA-Fat findings and also warrants further study.
Our study demonstrates that stimulated BAT in rats avidly accumulates 18F-FDG, detectable on both biodistribution studies and PET imaging. Further, our methods show changes in BAT activity with varying pretreatments, suggesting the potential usefulness of 18F-FDG PET imaging in obesity research, which focuses on BAT activity in terms of energy consumption. It has been reported that the recently developed β3-adrenergic receptor agonists may be promising for treating obesity by increasing or inducing energy consumption activity not only in BAT but in WAT or muscles (22). In this regard, 18F-FDG PET imaging may be useful for predicting treatment response by detecting changes in energy consumption after administration of β3-adrenergic receptor agonists.
CONCLUSION
This rodent study showed that BAT exhibited high 18F-FDG uptake under stimulated uncoupling conditions. Predosing with reserpine and propranolol decreased this high 18F-FDG uptake to less than 30% of the control values in biodistribution studies. These decreases were reflected as faint to mild 18F-FDG uptake in BAT on 18F-FDG PET images, in contrast to the intense uptake in the control group. The effect of these drugs on 18F-FDG uptake in BAT and on the function of other organs should carefully be evaluated clinically as a method to improve the accuracy of PET imaging of tumors.
Acknowledgments
The authors thank the imaging technologists and the radiochemistry and radiopharmacy staffs of the PET center of Johns Hopkins Hospital for their excellent technical assistance.
Footnotes
Received Oct. 15, 2003; revision accepted Jan. 14, 2004.
For correspondence or reprints contact: Richard L. Wahl, MD, Division of Nuclear Medicine, Department of Radiology, Johns Hopkins Medical Institutions, 601 N. Caroline St., Room 3223A, Baltimore, MD 21287-0817.
E-mail: rwahl@jhmi.edu





{kind=link}
{kind=link}
{kind=link}